Introduction
The potential significance of an asymmetrical posterior lumbar facet in the pathogenesis of low back pain was proposed by Putti [1] in 1927, who introduced the term ‘facet tropism’ (FT). FT was described in 1929 by Brailsford [2] as an asymmetry between the left and right vertebral (apophyseal) facet joint angles with one joint having a sagittal orientation of 5° or 7° more than the other. Despite several studies conducted, there is no consensus on the relation between sagittally aligned facet (SAF) joint and lumbar disc herniation (LDH). The hypothesis that FT is correlated with the presence of disc herniation is still debated. Some studies have suggested that the SAF joint contributes to disc degeneration and subsequent degenerative spondylolisthesis (DS). However, the role of FT in DS is still unclear. The aim of this study was to clarify the relationship of both FT and the SAF joint with LDH and DS. Further, we calculated the relationship between the side of disc herniation and that of the SAF joint.
Materials and Methods
Between June 2015 and December 2017, magnetic resonance imaging (MRI) scans of 250 consecutive patients who underwent surgery for LDH and DS were analyzed. Data were classified according to the predetermined criteria, and the patients were divided into the LDH and DS groups. Only MRI scans with complete records were selected until the intended number of 250 was achieved for each group. Institutional ethical committee clearance was not required as the study was only conducted on the images.
1. Measurement of the facet angle
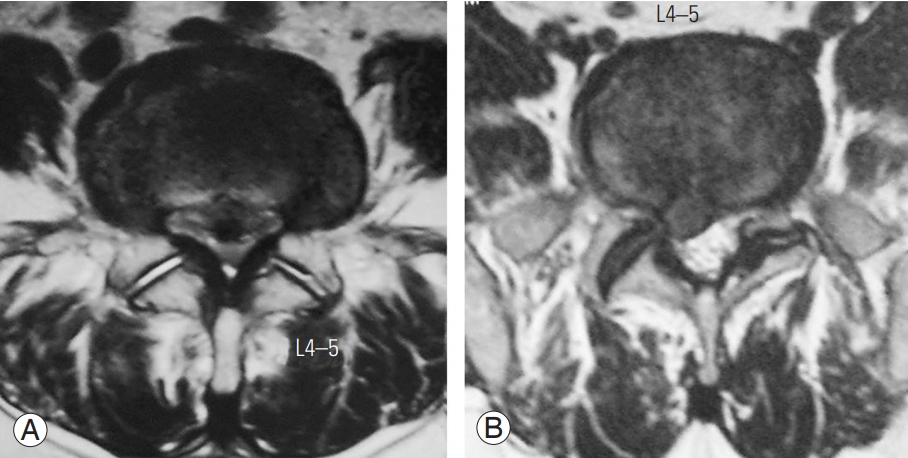
The orientation of the facet angles was measured on the axial T2-weighted MRI images using the method described by Noren et al. [3] from the third lumbar to first sacral vertebrae. MB Angle software (Markus Bader-MB software solutions ver. 5.3; MB Software Solutions, Iffezheim, Germany) was used to calculate the left and right facet joint angles. On the T2 axial image that bisected the intervertebral disc, one line was drawn in the midsagittal plane of the vertebra passing through the center of the disc and center of the base of the spinous process, and another line was drawn between the anteromedial and posterolateral edges of the superior articular facets bilaterally (Fig. 1). All facet angles were measured as the angle between the oblique line and the sagittal plane on both sides. The cutoff angles of 36° at L3–4, 42° at L4–5, and 45° at L5–S1 were set as indicators for SAF joints. The difference between the two angles (FT) was calculated. According to the method described by Vanharanta et al. [4], moderate tropism was defined as a difference of 7° to 15° and severe tropism as more than 15°.
2. Data and statistical analysis
All the observations were recorded on a standard Excel sheet (Microsoft Corp., Redmond, WA, USA). The average facet angles including standard deviation were calculated at each level on both sides. The incidence of sagittal facet angles and FT based on the criteria set was noted at each level. In the LDH group, the distribution of the level of disc herniation and side of herniation at different levels was recorded. In addition, the association between SAF and FT in relation to the side of herniation at each lower lumbar level was analyzed. In the DS group, a similar analysis was performed for each lower lumbar level in terms of SAF and FT. Chi-square test was used to determine the relationship between the previously mentioned criteria. A p-value <0.05 was considered significant.
Results
Of the 500 patients studied, 51% were males and 49% were females. The mean age was 49.1 years (range, 15–88 years). A total of 1,500 lumbar levels (3,000 facet angles) were considered, including L3–4, L4–5, and L5–S1. The patients were divided into two groups, the LDH group and the DS group, based on the diagnosis.
In the LDH group, 17 (6.8%) had disc herniation at L3–4, 135 (55.2%) at L4–5, and 98 (39.2%) at L5–S1. SAF at L3–4 (<36°) was 57%, L4–5 (<42°) was 47.8%, and L5– S1 (<45°) was 35.6%. FT was noted to be 30.8% at L3–4, 35.6% at L4–5, and 45.2% at L5–S1 as shown in Tables 1 and 2. There was a positive relationship observed between SAF and LDH at L4–5 and L5–S1 with a p-value of 0.02 (<0.05). FT showed a positive association with LDH at L4–5 (p-value=0.047) but not at L3–4 or L5–S1.
In the DS group, 16 had degenerative listhesis at L3–4, 180 at L4–5, and 54 at L5–S1. SAF at L3–4 was 65%, L4–5 was 64.6%, and L5–S1 was 49%. FT was noted to be 32.8% at L3–4, 26.4% at L4–5, and 39.2% at L5–S1 as shown in Tables 3 and 4. SAF showed a positive relationship with a p-value of <0.001 at L4–5 but not at L3–4 or L5–S1. FT showed a significant relation at L4–5 (p-value <0.001) but did not show positive association at L3–4 and L5–S1.
Discussion
Facet joint orientation seems to play an important role in lumbar biomechanics. Asymmetry in the orientation of the facet joints is estimated to occur in 10%–70.5% of the population [5]. Our study revealed an overall incidence of FT of 52.5% (55.8% in the DS group and 49.2% in the LDH group) in the 500 spinal units studied. The severity of FT increased from L3–L4 (32.8% in the DS group and 30.8% in the LDH group) to L5–S1 (39.8% in the DS group and 45.2% in the LDH group). The intervertebral disc and both facet joints make a three-joint complex, each structure affecting the biomechanics of the other (coupling effect). Theoretically, facet joints share load mainly during compression and extension of the lumbar spine. They also protect the disc from excessive rotational strain and anterior shear forces. It therefore has been postulated that a more sagittal alignment of the joint leads to anterior gliding due to a reduced resistance to anterior shear forces [6-8]. These forces are particularly large in the lower two segments of the lumbar spine, as lordosis and horizontal vertebral tilt increase. The presence of coronal orientation at the L5– S1 facet joint compared to L3–4 and L4–5 indicates the natural mechanism for overcoming these forces. Our study findings were consistent with regard to the presence of more SAFs at L3–4 (57% in the DS group and 65% in the LDH group) and coronally oriented facets at L5–S1 (35.6% in the DS group and 49% in the LDH group).
1. Relation between sagittally aligned facet and lumbar disc herniation
Studies relating SAF and the development of LDH have yielded variable results (Table 5). Having more SAF joints offers little or no mechanical resistance to rotational forces, resulting in the inability to protect the disc from injury. Farfan and Sullivan [6] concluded that a more obliquely oriented facet would allow increased rotation toward the oblique side. In a cadaver-based study, Cyron and Hutton [7] noted that specimens with tropism were inclined to rotate toward the more oblique facet when an axial load was placed on the spine segment. A computed tomography (CT) scan study by van Schaik et al. [8] revealed that with greater degrees of asymmetry, there was an increased incidence of unilateral disc protrusion toward the side of the more coronally oriented joints. Although a majority of studies correlate the occurrence of disc herniation toward the more obliquely oriented facets, a few studies, such as that of Adams and Hutton [9] demonstrated that this angular rotation was not significant in the etiology of disc prolapse. However, in the present study, a significant correlation was observed between the side of SAF joint and LDH at L4–5 and L5–S1 levels. The L3–4 level did not demonstrate association with SAF or FT. We noted that there was a tendency for the occurrence of disc prolapse on the more sagittal side whenever there happened to be a combination of sagittal and coronal facets at the same level especially at L4–5 but not at L3–4 or L5–S1. We hypothesize that whenever the lower lumbar spine is loaded during flexion-extension, the more oblique side resists the angular motion, and the more SAF allows angular motion as well as rotation in order to compensate for the other facet. Thus, this rotational movement indirectly applies tensile stress on the annulus of the disc, leading to prolapse on the sagittal side (Fig. 1B).
2. Relation between facet tropism and lumbar disc herniation
A similar controversy exists as regards the correlation between FT and LDH (Table 5). Farfan and Sullivan [6] were the first to suggest the correlation between FT and the development of LDH. Studies by Ishihara et al. [10] and Karacan et al. [11] further reported the same association. Recent studies by Chadha et al. [12] also suggested that FT is associated with LDH at the L5–S1 motion segment but not at the L4–L5 level. In this study, they found that the disc has herniated toward the sagittally oriented facet in 13 out of 19 cases with tropism; however, the sample size was small and insufficient. The degree of FT has been reported to play a role in the development of posterolateral as well as far-lateral disc herniation in a study by Park et al. [13]. However, several studies have disproved this hypothesis [4,14-19]. Our study demonstrated that FT is related to LDH at the L4–5 level but not at L3–4 or L5–S1.
3. Relation between sagittally aligned facet and degenerative spondylolisthesis
The mobility between two adjacent motion segments is determined by the orientation of the plane of facet joint articulations. In comparison with other portions of the spine, facet joints in the lower lumbar spine have a closer orientation to the coronal plane and are more rigid during lateral bending [20]. Previous reports have demonstrated that facet orient ation is significantly associated with DS [21-29]. In an MRI-based study, Boden et al. [21] reported that both the left and the right facet joints were more sagittally oriented in patients with DS. Additionally, some of these studies reported that, in patients with DS, the transverse plane of facet joints was more sagittally oriented. Our study found that the SAF joint was significantly associated with DS only at L4–5, which was the most commonly affected level. In contrast to other studies, the L3–4 and L5–S1 levels did not demonstrate any positive association.
4. Relation between facet tropism and degenerative spondylolisthesis
The relationship between FT and DS remains a debatable issue. Berlemann et al. [30] reported that facet joint asymmetry does not seem to play a major role in the development of DS. A study by Kong et al. [31] found no association between FT and translational segmental motion. In an MRI-based study, Grannum et al. [32] suggested that sagittally oriented facets are not associated with the causation of DS. However, a recent study by Pichaisak et al. [29] reported a positive association between SAF and FT and the development of DS [33]. Our study demonstrated that the L4–5 level appears to be related to FT, but no significant relationship was observed between FT and DS at L3–4 and L5–S1.
5. Limitations and strengths
There were several limitations with regard to the current study. Initially, this was a cross-sectional observational study conducted only on surgically treated patients. The primary source of error could be in the identification of the reference plane and the margins of the facet joint, which is operator-dependent. The characteristic of hypertrophic ‘lipping’ of the superior facet can lead to errors in the measurement of facet joint angle; nevertheless, an established method was used for measurement, with proven consistency through interobserver reliability studies. The discrepancy in SAF or FT cutoff angles has been described to be varied in literature, and we have used only one methodology, which is the only applicable approach. Neither did we include sagittal balance, lumbar lordosis, other pelvic and angular parameters, body mass index, and other demographic features that may individually influence the development of LDH or DS. Although the measurement of facet joint angle from an MRI axial T2- weighted image is less accurate than that from a CT image, we found the reliability of this measurement method was comparable and consistent with several previous studies. The strengths of the present investigation include the use of a large sample size. We have analyzed the facet orientation and tropism in each level and side of disc herniation, highlighting new concepts that can be useful for future longitudinal studies. Many previous studies have used the adjacent segment as a control to determine the results. However, we have used the same segment bearing a greater significance than the adjacent segment controls in performing comparisons. The measurement technique was highly reproducible, and the actual measurements were consistent with values reported in several previous studies whereby CT scans were used. Our methodology provided normative data as well as evidence of the clinical relevance for further studies on the orientation of the lumbar facet joint and FT.
Conclusions
In the present study, we found that the L4–5 level was significantly associated with SAF and FT in LDH and DS. SAF at L5–S1 demonstrated a positive association with LDH. These findings can provide useful information for future longitudinal studies. Nevertheless, further randomized epidemiological studies are needed to confirm such associations and also to elucidate the possible causes for such phenomenon.