Introduction
Neck pain and low back pain are common complaints all over the world. Clinical practice guidelines recommend that people with neck pain or low back pain should undergo exercise therapy [1-4]. Oe et al. [5] reported the cut-off values and factors that negatively influenced the Neck Disability Index (NDI). This study suggested that the negative factors in males were manual work and cervical malalignment on a whole-spine standing radiograph and in females were lower body fat percentage, lower hand grip strength, and a lack of sporting activity. It is also reported that cervical sagittal malalignment on a whole-spine standing radiograph deteriorates along with patientreported outcome (PRO) [6-8]. However, it remains unclear why females with no cervical malalignment show poor scores on the NDI.
It is well-known that neck pain is more frequent in females than in males [9-11]. Cagnie et al. [12] reported in their internet study that the incidence of neck pain in females (54.7%; 123 of 225 office workers) was significantly higher than that in males (38.3%; 110 of 287 office workers) and sex was a significant risk factor contributing to neck pain. Moreover, they reported that the incidence of neck pain among people who do not participate in sporting activities (56.7%; 111 of 196 office workers) was also significantly higher than those who do participate in sporting activities (38.6%; 122 of 316 office workers). However, there are very few studies that support the theory that sporting activity is effective for improving neck pain. Some studies though have demonstrated that psychosocial stress is also an important risk factor in neck pain and back pain [9,10,13,14]. The purpose of this study is to investigate how sporting activity can affect the parameters of whole-spine standing radiography, EuroQol-5 dimension (EQ-5D), Oswestry Disability Index (ODI), and NDI, as well as to assess psychosocial stress by sex.
Materials and Methods
1. Institutional review board approval
The study protocol was approved by the institutional review board of Hamamatsu University School of Medicine, Shizuoka, Japan (IRB approval no., 201201).
2. Subjects
The participants of this study were 870 volunteers who lived in Toei town in Aichi prefecture, Japan. They participated in a health screening study called the TOEI Study in 2016 after responding to public notices. They joined this study on a voluntary basis. All of the participants provided their written informed consent.
3. Inclusion criteria
The inclusion criteria were as follows: (1) age 40 years old or more and (2) informed consent for participation in this study.
4. Exclusion criteria
The exclusion criteria were as follows: (1) no available whole-spine radiographs in the standing position; (2) no questionnaire returns; (3) Cobb angle >25° in the coronal plane on radiographs; (4) symptomatic osteoporotic fractures with severe wedge-shaped vertebrae of grade 3 according to semi-quantitative grading [15]; and (5) history of instrumented spinal surgery or joint arthroplasty.
5. Data collection and radiographic parameters
The following demographic characteristics were evaluated: age, height (cm), weight (kg), body mass index (BMI, kg/m2), grip strength in right hand (kg), hand grip strength, body composition (amount of muscle; kg, percent of body fat, and basal metabolism; kcal/day), and bone mineral density (BMD). Body composition was measured using bioelectrical impedance analysis via a Tanita Dual-Body Composition Monitor (DC-430A; Tanita Corp., Tokyo, Japan). This device was validated for the precise evaluation of body composition [16]. BMD of the total proximal femur was measured using dual-energy X-ray absorptiometry and expressed as a percentage of the young adult mean (%YAM). The total proximal femur was evaluated in this study because the lumbar spine was affected by degenerative changes, especially in the elderly. The questionnaire items were as follows: (1) sporting activity “Are you currently in the habit of participating in sports? What kind of sport is it?”; (2) number of births; (3) ODI, EQ-5D, and NDI for evaluating (PRO); and (4) Hospital Anxiety and Depression Scale (HADS) for evaluating mental status [17]. HADS is a 14-item scale in the form of a self-administered questionnaire. These items are divided into anxiety (HADS-A; seven items) and depression (HADS-D; seven items). Each item was scored on a 4-point scale from 0 (good) to 3 (bad). Possible total scores (HADS-T) range from 0 to 42. Higher scores indicate a more severe anxiety or depression status. All volunteers answered these questionnaires when they attended the health screening.
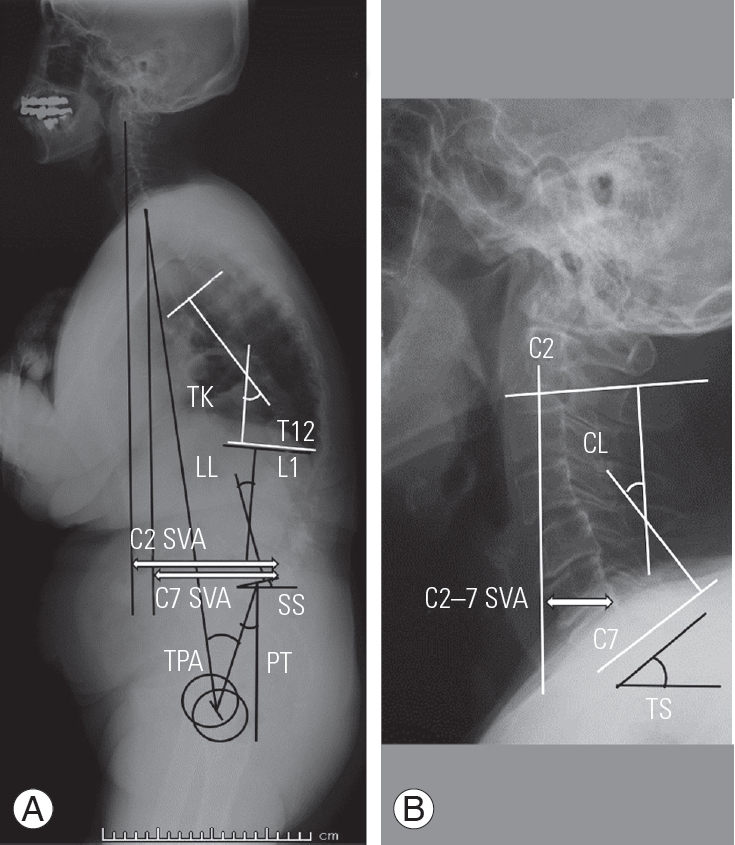
The evaluated radiographic parameters were as follows (Fig. 1): (1) sacral slope (SS); (2) pelvic tilt (PT); (3) pelvic incidence (PI); (4) lumbar lordosis (LL; L1–S1); (5) PI minus LL (PI-LL); (6) thoracic kyphosis (TK; T5–T12); (7) T1 slope (TS); (8) cervical lordosis (CL; C2–C7); (9) TS minus CL (TS-CL); (10) C2–7 sagittal vertical axis (C2–7 SVA; distance between a plumb line from the center of the C2 vertebra and the posterior superior corner of C7); (11) C7 SVA; (12) C2 SVA; and (13) T1 pelvic angle (TPA; the angle between a line from the femoral heads to the center of the T1 vertebral body and a line from the femoral heads to the center of the superior sacral end plate). The digitized radiographs were transferred to an imaging software (Surgimap Spine; Nemaris Inc., New York, NY, USA), and each parameter was measured by seven board-certified spine surgeons in Hamamatsu University Hospital.
6. Statistical analysis
Statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA). The independent t-test or chi-square test was used to detect differences according to the sporting activity. The factors associated with a sporting activity were investigated using multiple logistic regression analysis. A p-value of <0.05 was considered statistically significant.
Results
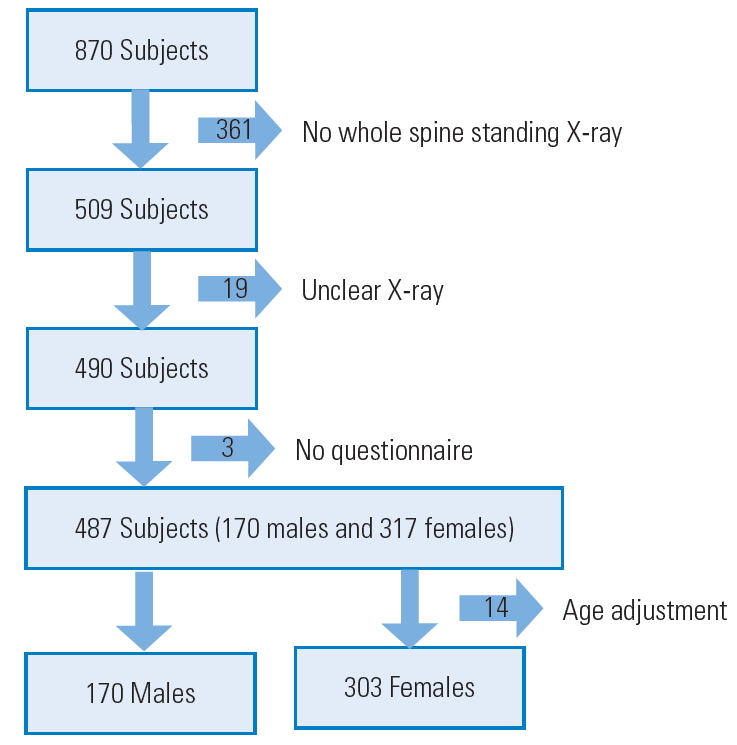
The volunteer recruitment process is shown in Fig. 2. A total of 397 volunteers were excluded for the following reasons: no whole-spine standing radiograph (n=361; they did not wish to undergo radiography); unclear radiograph (n=19; it was impossible to evaluate the radiographic parameters); no questionnaire returns (n=3); and age adjustment (only 14 females). In the females, there was a gap of the age between the no sporting activity group (NS group, lower age) and the sporting activity group (S group, higher age). Therefore, 14 females were excluded for age matching in both groups. Finally, 170 males and 303 females were recruited for this study.
1. Demographic data among volunteers
Table 1 shows the demographic data among the volunteers by gender. There were 101 and 69 male volunteers in the NS group and S group, respectively. There were 178 and 125 female volunteers in the NS group and S group, respectively. In the NS group, the mean age of the males was 74.9 years and of the females 73.6 years. In the S group, the mean age of the males was 74.6 years old and of the females 73.9 years, after age adjustment. There was no significant difference between the males in the S group and the males in the NS group in terms of height, weight, BMI, grip strength, muscle mass, body fat percentage, basal metabolic rate, YAM value, and number of births. A similar result was found when the females in the S group were compared with the females in the NS group. Moreover, HADS-A, HADS-D, EQ-5D, ODI, and NDI did not differ in the males in the S and NS groups. However, unlike the males, the females in the S group had significantly better scores for HADS-A (NS group:S group, 6.1:5.1; p=0.024), HADS-D (NS group:S group, 4.3:3.3; p=0.012), HADS-T (NS group:S group, 10.4:8.4; p=0.009), EQ-5D (NS group:S group, 0.787:0.857; p=0.000), ODI (NS group:S group, 16.8%:11.8%; p=0.001), and NDI (NS group:S group, 12.0%:8.9%; p=0.007).
2. Radiographic parameters among volunteers
Radiographic parameters in both males and females are shown in Table 2. There were no significant differences in lumbo-pelvic (SS, PT, PI, LL, and PI-LL), cervico-thoracic (TK and TS), and global alignment (C7 SVA, C2 SVA, and TPA) in the males in the S and NS groups. However, there were significant differences in CL (NS group:S group, 17.4°:21.6°; p=0.044) and TS-CL (NS group:S group, 9.8°:5.9°; p=0.040), which represents cervical alignment.
In terms of the lumbo-pelvic (SS, PT, PI, LL, and PI-LL) and cervico-thoracic (TK, TS, CL, TS-CL, and C2-7 SVA) parameters, there were no significant differences in the females in the S and NS groups. However, global alignments, except for TPA, were significantly worse in the female NS group than in the female S group (C7 SVA, NS group:S group, 28.4:14.0 mm; p=0.025; C2 SVA, 36.6:21.9 mm; p=0.036).
3. Significant factors correlated with sporting activity participation using multiple logistic regression analysis
We used a multiple logistic regression analysis to identify the factors most affected by participation in sporting activities and to investigate why sporting activity was effective in females for a good PRO score. The dependent variables were set as participation in sporting activities and non-participation in sporting activities. In the males, the independent variables were set as LL, CL, and TS-CL based on the results shown in Tables 1 and 2. However, there were no significant factors associated with participation in sporting activities. In the females, the independent variables were set as HADS-A, HADS-D, HADS-T, C7 SVA, and C2 SVA. The only significant factor associated with participation in sporting activities in the females was HADS-T (p=0.010; odds ratio, 0.950; 95% confidence interval, 0.913–0.987).
Discussion
Oe et al. [5] reported the factors associated with a negative influence on NDI, and our results suggested that in the males, these factors were cervical sagittal malalignment on the whole-spine standing radiograph, and in the females, lack of participation in sporting activities and the possibility of sarcopenia. There are many reports that sporting activities are effective for improving neck or back pain [1-4]. However, the purpose of this study was to clarify why a lack of participation in sporting activities was a factor in female NDI and not in males. As shown in Table 1, there was no significant difference in PRO (EQ-5D, ODI, NDI) in males regardless of their participation or non-participation in sporting activities. On the other hand, females with sporting habits had significantly better outcomes on the EQ-5D, ODI, and NDI.
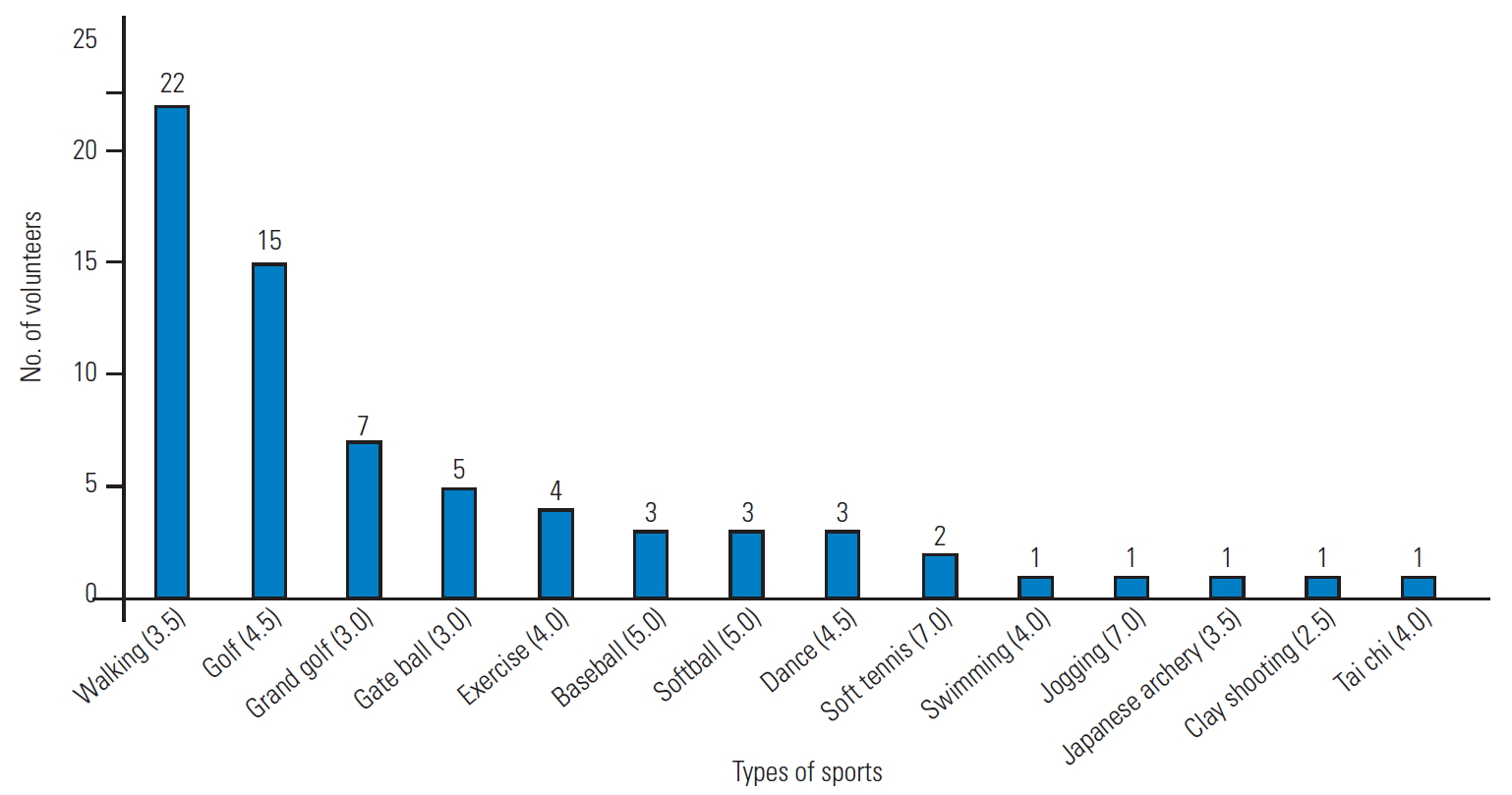
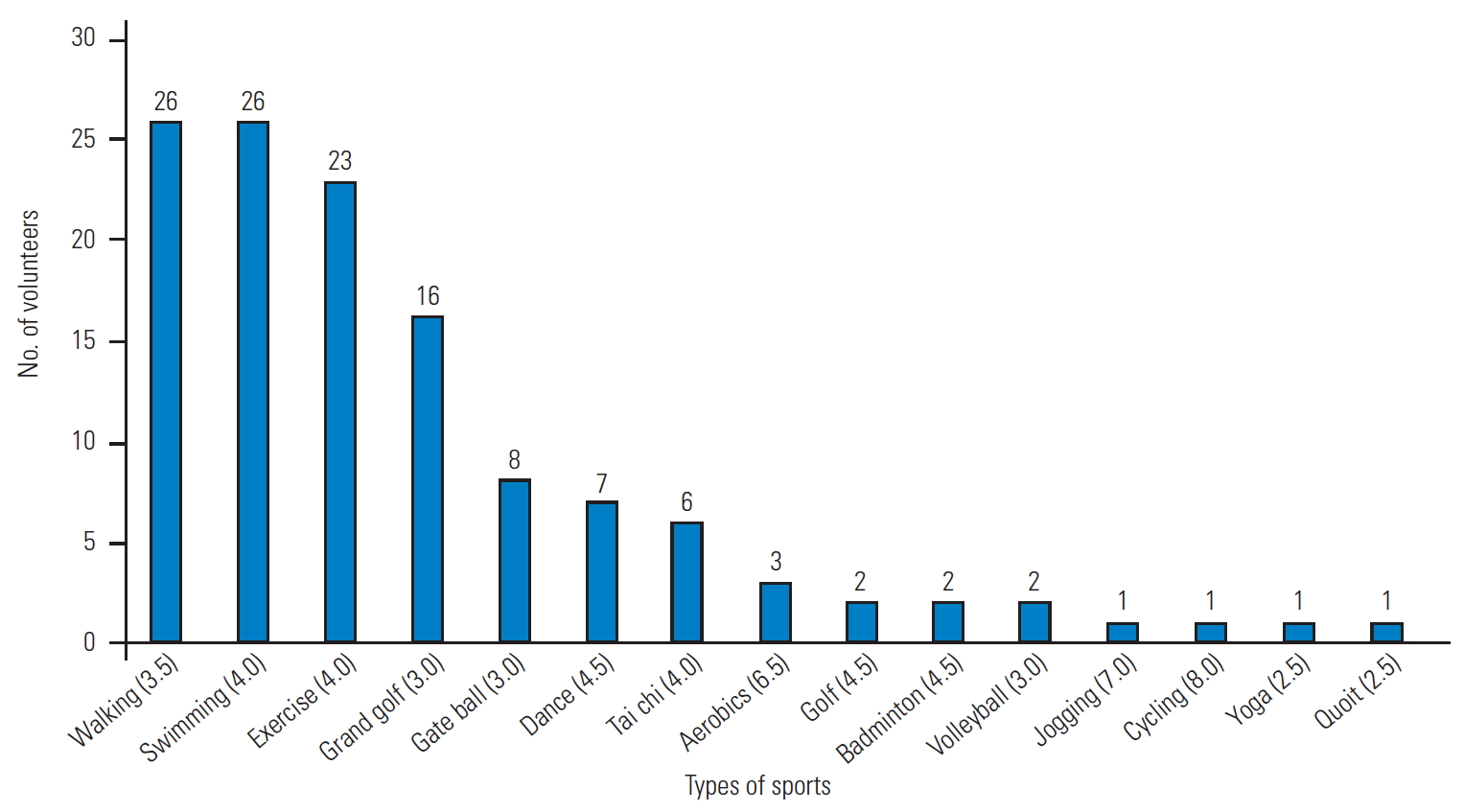
Details regarding the types of sporting activities by sex were shown in Figs. 3 and 4. Exercise intensity was evaluated using metabolic equivalent (MET) [18]. The mean exercise intensity was 4.0 METs in the males and 3.8 METs in the females. There was no significant difference with regard to the exercise intensity of each sporting activity undertaken by the males and females (p=0.223). Despite this, we did find that HADS-T was the most relevant factor according to participation and nonparticipation in sporting activities in the females. Table 3 shows the correlation coefficients between HADS-T and PRO. In the males, the correlation coefficient with HADST was −0.436 for EQ-5D, 0.441 for ODI, and 0.517 for NDI, whereas in the females, they were −0.396 for EQ-5D, 0.431 for ODI, and 0.546 for NDI. These results suggested that HADS-T was strongly correlated with all PRO. As shown in Table 1, the females who are engaged in sporting activities have significantly lower HADS-A, HADS-D, and HADS-T scores compared with the females who are not. However, no significant difference was observed for HADS-A, HADS-D, and HADS-T in the males, regardless of participation or non-participation in sporting activities. In the males, the mean HADS-T score was 8.2 in both the NS and S groups. In the females, the HADS-T scores were significantly higher in the NS group (10.4) than in the S group (8.4), which was similar to the HADS-T scores in the NS and S groups in males. In other words, as shown in Table 1, females initially have higher HADS-T scores than males, but participation in sporting activities may improve their mental statuses. As a result, this can make the PRO better. Indeed, it has been reported that sporting activities can improve anxiety and depression [19,20]. However, in the males, there was no change in the HADS score based on participation in sporting activities, but this result was because male HADS was not initially high. Therefore, we cannot conclude that participation in sporting activities is not effective for anxiety and depression in males.
In this study, we also investigated how participation in sporting activities influences various radiographic parameters (Table 2). In the males, TS-CL, which is an index of cervical malalignment, was significantly better in the S group. In the females, C2 SVA and C7 SVA, which are indexes of global alignment, were significantly better in the S group. It might be effective to maintain muscle power due to sporting activity. Oe et al. [7] reported that deteriorated alignment originated from the cervical spine in males and from the pelvis in females. These results suggest that sporting activities may prevent deterioration of spinal malalignment with age.
This study has several limitations. First, 397 (45.6%) of the 870 volunteers who participated were excluded. The majority of these people (361 people) were excluded because they did not want to undergo whole-spine radiography. Radiography involves radiation exposure, which is why we could not strongly recommend radiographic examination. This exclusion might involve selection bias. Second, as the subjects were relatively elderly people living in mountainous areas, these results may not be generalizable to young people and those living in urban areas. Third, the data were based on the questionnaire of self-report. Therefore, the definition of sporting activity also depended on them. In other words, it was defined as sporting activity if volunteers considered it sporting activity. However, it was controversial whether low MET activity could be a sporting activity for training muscle because the actual frequency and intensity of the sporting activity were unclear. Fourth, spinal alignment was affected by not only sporting activity but also multiple factors (i.e., genetics, lifestyle, and work). Further study associated with spinal alignment should be necessary. Finally, in this study, we could not deny the possibility that people with good mental status liked to play sporting activities. Furthermore, longitudinal studies are required to investigate the changes that result from participation in sporting activities.
Conclusions
In conclusion, our results suggested that people with sporting activities had good spinal alignment, especially cervical spine alignment in males and global alignment in females. Sporting activities might also prevent deterioration of the spinal alignment with age. In addition, the HADS scores were significantly correlated with PRO. Therefore, females with sporting activities had good score of EQ-5D, ODI, and NDI because the HADS scores were significantly better. However, if PRO does not improve even after surgical treatment or medications, it is necessary to investigate the mental status of the patient.