Introduction
Primary tumors of the sacrum are very rare entities, constituting approximately 1%–7% of primary spinal tumors, which in turn constitute only a mere 10% of primary bone tumors [1]. Low-grade primary tumors are often diagnosed late, owing to their clinical resemblance to degenerative lumbar spine disorders, while high-grade tumors might have an early and a more dramatic presentation [1,2]. Primary sacral tumors can be benign or malignant and, based on their origin, can be predominantly grouped as primary osseous or primary neurogenic. The most common malignant sacral lesions are chordomas, which are low-grade tumors, whereas the most common benign lesions are giant cell tumors (GCT), which are locally aggressive and potentially recurrent [2].
The management of these tumors is based on numerous factors, such as tumor pathology, the upper limit of the tumor extent, involvement of neural structures, and distant metastasis [3]. Nevertheless, surgery remains the cornerstone for treating nonmetastatic primary sacral tumors [1–4]. The complex sacral anatomy, including the neural structures, adjacent visceral relationships, biomechanical role in load transmission, and late presentation of sacral tumors often poses a surgical challenge, making the surgery a multidisciplinary affair. These operations were once considered long, bloody, and morbid procedures; however, a multidisciplinary approach and recent advances have helped achieve significant breakthroughs in the treatment paradigm of primary sacral tumors. Aggressive sacral resections can cause varying degrees of neurological (bladder, bowel, motor, and sexual) dysfunction based on the level [1,5]. In the end, achieving good disease control and minimizing neurological complications are paramount in reaching positive treatment outcomes.
In our study, we present a group of 15 patients with primary sacral tumors that include bony tumors, neural tumors, and sarcomas, which were treated accordingly. Based on a literature review and our experience, we propose a protocol for managing primary sacral tumors entailing a multidisciplinary approach.
Single Institution Experience of Primary Sacral Tumors
We studied the case records of patients with primary sacral tumors treated between 2011 and 2020 in Sakra World Hospital, Bengaluru, India which is a tertiary spine care center, a tertiary spine care center. We included case records only of patients with a minimum 2-year follow-up. Patients with sacral lesions that were ultimately infections and metastatic lesions were excluded, given these cases were beyond the scope of our study. Ultimately, 15 patients were included, and their medical records, radiological images, and pathology reports were retrospectively reviewed. Given that the study was conducted using only the patients’ in-patient and follow-up records, ethical approval for the study was waived.
All of our patients had undergone a uniform management protocol starting with a thorough neurological and clinical (including per rectal) examination, which was followed by X-rays, computed tomography (CT) and magnetic resonance imaging (MRI) to assess soft tissue extension. Positron emission tomography (PET) CT was also performed to search for distant metastasis when necessary. A percutaneous CT-guided biopsy of the lesion was performed by our interventional radiology team with the patient under local anesthesia to obtain a histological diagnosis. After the investigations had been concluded, the management was planned based on (1) the clinical presentation, especially neurological dysfunction; (2) the tumor pathology, as per the histopathological examination; (3) the upper extent of the lesion (MRI); (4) the soft tissue extent and local invasion of adjacent structures (MRI); and (5) the presence of metastasis (PET). All cases were subjected to a tumor board review comprising the treating surgeon, radiologist, pathologist, medical oncologist, plastic surgeon, urologist, and radiation oncologist for the decision-making process regarding treatment. Radiotherapy or chemotherapy was administered for inoperable advanced malignant lesions.
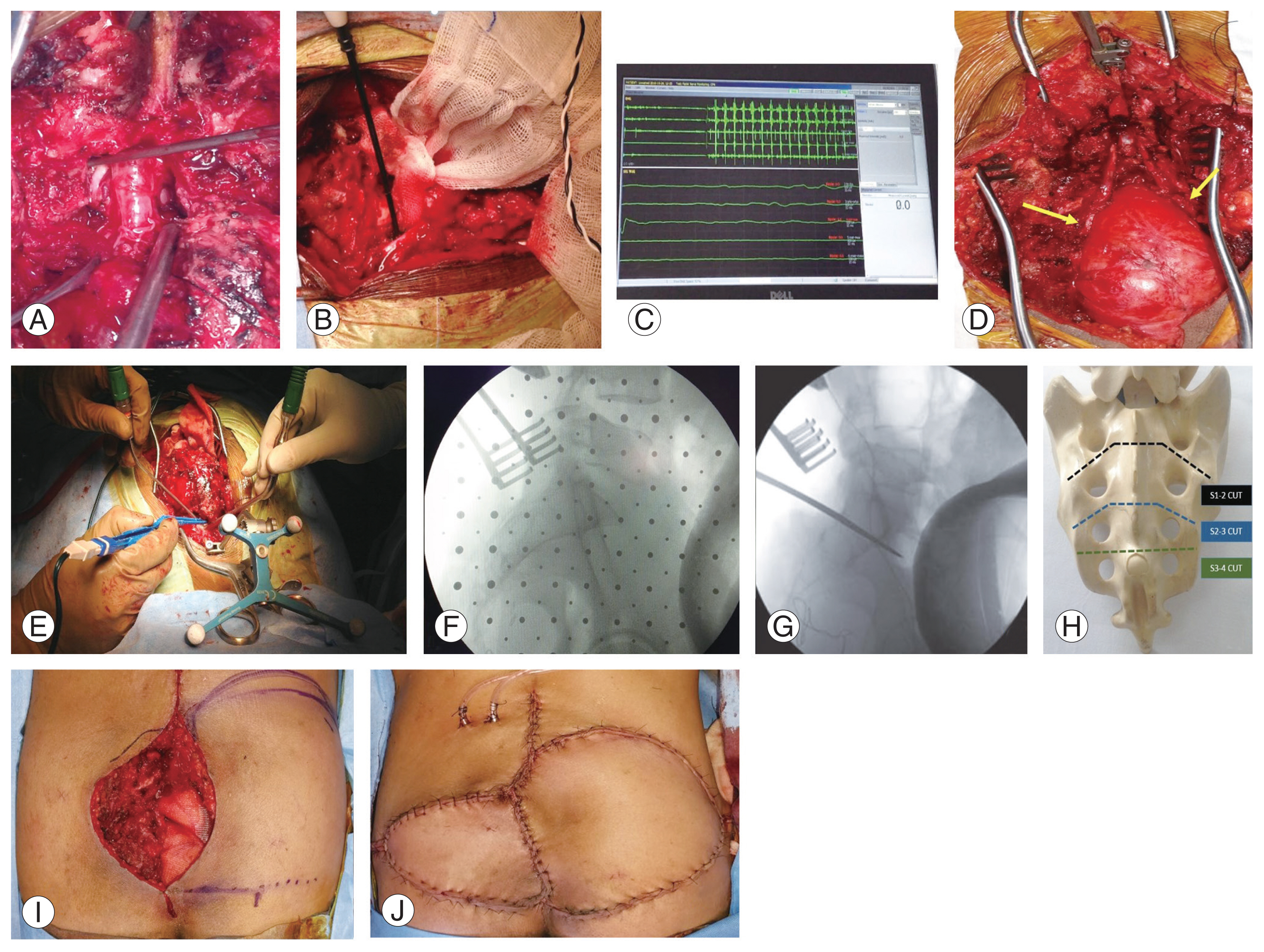
Clear surgical principles were considered for all cases, which included (1) an all-posterior approach; (2) sacrectomy with wide excision to achieve clear margins to minimize recurrence; (3) preservation of S1 and sacroiliac joint integrity to prevent lumbopelvic fixation, if possible (except in one case in which S1 was removed to achieve wide excision); (4) preservation of at least one S2 nerve root to preserve bladder function; and (5) plastic reconstruction with advancement flaps when necessary. Neural tumors were treated by laminectomy and lesion excision. Regardless of the sacrectomy level, neural dissection was started at L5–S1 through a laminectomy and traced distally to preserve at least one functional S2 nerve root (Fig. 1A–D). The functional status of the nerve roots was identified using triggered electromyography of the foot muscles and anal sphincter muscles, a component of intraoperative neural monitoring. Seeding of tumor tissue was avoided by total excision of the tumor and excision of the biopsy tract after its identification by methylene blue injection. Preoperatively, cytoreduction was attempted in chemosensitive tumors such as Ewing’s sarcoma (ES). Digital subtraction angiography (DSA) followed by a preoperative transarterial embolization (TAE) in hypervascular tumors such as GCTs was performed to reduce blood loss.
Prophylactic antibiotic prophylaxis was with 1 g intravenous ceftriaxone administered 30 minutes prior to the surgical procedure and was repeated every 4 hours if necessary. Intraoperative blood loss was reduced by the usage of tranexamic acid infusion in patients who could not tolerate significant blood loss. Neuro-navigation was utilized to perform an accurate sacral resection at the planned level (Fig. 1E–H). The plastic surgery team was involved in cases of large skin or soft tissue defects to plan and perform an appropriate flap cover (Fig. 1I, J). Postoperatively, the same antibiotic was continued intravenously until the day of surgical site drain removal after wound inspection.
Follow-up records of patients at 1 month, 6 months, 1 year, and 2 years were reviewed along with their respective radiological images. Treatment outcomes considered in our study were (1) functional outcome (pain-related disability and neurological function) before and after treatment; and (2) disease control (recurrence and metastasis) after completion of treatment. The Visual Analog Scale was used to assess pain-related disability. The assessment of neurological function, including motor, bladder, and bowel function scoring, was as adapted from Biagini et al. [6] and is shown in Table 1.
The continuous variables are expressed as mean±standard deviation and the categorical variables as frequencies and percentages. For comparison analysis, the Wilcoxon signed rank test was used due to the non-normal data distribution. The data were analyzed using IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA).
The characteristics of all 15 cases included in our study are shown in Table 2. A total of 15 patients with primary sacral tumors were reviewed, of which 10 were men and five were women. Two patients had extracompartmental recurrent chordomas after prior surgery elsewhere. All 15 patients had back pain as a presenting symptom; six had radicular symptoms or signs; five had bladder and bowel dysfunction. The most common diagnosis was chordoma (n=7). The proximal extent of lesions was up to S1 in four patients. However, only two were surgically treated. A total of 11 patients underwent surgery, including eight partial sacrectomies (without any instrumentation), one total sacrectomy (GCT involving S1) with lumbopelvic fixation and two patients with neural tumors treated with laminectomy and tumor excision. The average duration of surgery was 6.5 hours, with a mean blood loss of approximately 900 mL. The patient with a GCT underwent wide excision after TAE considering the aggressive nature and potential recurrence. One patient with ES received neoadjuvant chemotherapy (NAC) and underwent partial sacrectomy after cytoreduction. Four patients were treated with chemotherapy (one non-Hodgkin lymphoma; one adenocarcinoma; chemotherapy with radiotherapy in one case of inoperable ES; and NAC in one operable ES). Two inoperable patients underwent radiotherapy, which included one recurrent chordoma and one ES. One patient with mucinous cystadenoma had to undergo an additional anterior procedure and colostomy.
The mean follow-up was 29±9.8 months. Of eight patients who underwent partial sacrectomy (without additional stabilization), seven patients had no stability-related complications. One patient in whom the sacral cut was taken through the S1 body had an S1 stress fracture in follow-up and could be managed conservatively. Only one patient (out of five) who had preoperative bladder and bowel dysfunction regained reasonable function post-surgery, whereas the remaining four patients had no recovery and were taught self-intermittent catheterization. None (n=11) of the patients who had intact bowel and bladder function preoperatively worsened post-treatment. Two patients had postoperative surgical site infection, among which one patient needed debridement. One patient with recurrent chordoma had a second recurrence after partial sacrectomy surgery. Two patients (one with adenocarcinoma and one with mucinous cystadenocarcinoma) had a distant spread at the last follow-up and was followed up with chemotherapy. One patient with ES (treated with NAC and partial sacrectomy) developed pneumonia following a compromised immune status and ultimately succumbed to systemic sepsis. The results of our study have been summarized (Tables 3, 4).
Literature Review
Primary sacral tumors are rare, accounting for approximately 1%–7% of primary spinal tumors [1]. The majority of sacral tumors are metastatic lesions from breast, prostate, lung, or colon carcinomas [1], and their therapeutic approach differs completely from primary tumors [2]. Primary tumors can be classified based on their origin as osseous, neural (e.g., schwannoma), notochordal (e.g., chordoma), primitive neuroectodermal (PNET) (e.g., ES), hematopoietic (e.g., lymphoma, myeloma), and tumor-like (e.g., aneurysmal bone cyst) [2]. They can also be grouped into benign and malignant tumors. The most common malignant tumor of the sacrum is chordoma, followed by chondrosarcoma, myeloma, malignant nerve sheath tumors, ES, and lymphoma [2,5]. The common benign tumors include GCTs, schwannomas, and aneurysmal bone cysts. However not all benign tumors are low-grade lesions; e.g., GCTs, which can be locally aggressive. Hence, more usefully, the primary tumors can be grouped as (1) low-grade tumors (chordoma, chondrosarcoma), which are slow-growing with nonspecific clinical symptoms; and (2) high-grade tumors, such as ES, osteosarcoma, and GCT, which can have a more aggressive clinical presentation and recurrence [3]. As reported in the literature, chordoma was the most common primary tumor in our study (seven cases), followed by primary neural tumors and ES (two cases each).
MRI followed by CT is the most informative radiological investigation, given it provides a host of information, such as the possible epicenter of the lesion, presence of soft tissue matrix, probable tumor pathology, and most importantly the extent of tumor, which primarily dictates the level of sacral resection to be planned in cases needing a wide excision [1,7]. PET scan could be an important prognostication tool to opt between a curative treatment or a palliative treatment based on distant metastasis [7]. Given the pathology is the most decisive factor determining the prognosis and treatment of sacral lesions, CT-guided biopsy is a critical component in their diagnostic algorithm. Safaee et al. [8] reported a positive biopsy in up to 95% of sacral lesions, with correlation rates approaching 100%. Excision of the biopsy tract following CT-guided biopsy is less likely to cause tumor contamination of the surgical plane compared with open biopsy. We used methylene blue injection for the identification of the biopsy tract in our patients. Primary sacral tumors are treated principally based on four factors: (1) tumor pathology (based on biopsy); (2) the proximal extent of the tumor; (3) neurological dysfunction; and (4) contiguous spread and distant metastasis. The treatment modalities are chemotherapy, radiotherapy, and surgery, with surgery as the cornerstone of curative treatment in nonmetastatic primary tumors [2–4].
Various surgical approaches have been employed for sacral resections. Conventionally, total and high sacrectomies have been performed via combined anterior-posterior approaches [9–11]. The stand-alone posterior approach was initially advocated for distal sacral resections [12] and was later extended to en-bloc total sacrectomy with a few modifications by many authors [9,13–16]. The various literature discussing the applicability of an all-posterior approach has been listed (Table 5). The feasibility of an all-posterior surgical approach for sacrectomies is based on the anterior extent, proximal limit, and accessibility of the tumor [9,16]. An all-posterior approach has been shown to have lesser morbidity and blood loss compared with the combined approach [9,15,16]. The surgeries we performed in all the cases with no anterior visceral involvement employed only a posterior approach. The anterior extent of the tumor was preoperatively decided based on per rectal clinical examination and by MRI. We could remove the tumor en bloc even in lesions involved up to S1 employing a stand-alone posterior approach, starting the dissection caudally by division of ligaments and proximal blunt dissection deep to the presacral fascia and mobilization of pelvic structures. One patient in whom the primary lesion was a mucinous cyst adenocarcinoma contiguously involving the colon underwent an additional anterior bowel resection procedure along with a colostomy.
Wide excision with clear margins is the preferred treatment in aggressive benign and malignant tumors. Based on the level of resection, the surgeries have been termed as low, mid, high, hemi, and total sacral resections with predictable degrees of bowel, bladder, and sexual dysfunction [1,6,17]. Total sacral resections (involving the S1 body) could also result in lumbopelvic instability and warrant lumbopelvic fixation [18]. An optimal outcome could be obtained by minimizing disease recurrence by balancing a wide excision, concurrently preserving at least the S1 body to maintain stability and a few functional sacral roots contributing to the pudendal nerve to preserve bowel and bladder function. The necessary sacral roots to be preserved for good bowel and bladder function has been debated in the literature (Table 6). Various authors have recommended the preservation of the S3 root [19–26], with few among them reporting good function with preservation of one or more S2 nerve roots [12,17,27–29]. In our patients, irrespective of how high the sacrectomy, functional sacral roots (at least one S2 root) were preserved, provided they were not encased in the tumor seven of 11 surgical patients had intact bowel and bladder function before surgery; as a result of preserving at least one S2 root, none of them lost bowel or bladder function postoperatively. In our study, of eight patients who underwent partial sacrectomy, one patient (chordoma involved up to S1–S2) in whom the resection was performed through the S1 body had an insufficiency fracture of redundant S1 body (Fig. 2), whereas all seven remaining patients had no stability-related pain. The use of neuro-navigation helped in making precise osteotomy cuts where desired without destabilizing the sacroiliac joints, in addition to reducing the operating time and the amount of radiation exposure to the operating room personnel. One patient who underwent a total sacrectomy had additional lumbopelvic fixation.
Preoperative TAE of the feeding vessel after a DSA is known to reduce intraoperative blood loss and surgical time in all vascular sacral tumors [30]. Its effectiveness in treating chordoma and GCT are well reported in the literature [31,32]. We used preoperative TAE in one patient with a GCT extending up to S1, followed by total sacrectomy and reconstruction, which helped reduce intraoperative blood loss to less than 1,000 mL.
Neural monitoring is a useful adjunct in preserving neurological function by the identification of functional sacral roots. The activity of the anal sphincter can be extrapolated to the activity of the external urethral sphincter because both are innervated by the pudendal nerve, with a root value of S2, S3, and S4. Surgeon-triggered stimulation of these nerve roots can be picked up by sphincter electrodes during surgery [33], indicating the functional status of the nerve roots and warranting their preservation. Large sacral wound defects might require myocutaneous flaps for good healing. Bilateral gluteal musculocutaneous advancement (BGMA) flaps are sufficient in primary tumors treated without radiotherapy and preserved gluteal vessels, whereas trans-pelvic ventral rectus abdominal myocutaneous (VRAM) flaps need to be considered otherwise. Free flaps are considered if VRAM flaps have been scarred by previous abdominal surgeries [34]. Five of our patients had significant dead spaces after sacral resections. Two of them (one GCT treated with total sacrectomy and one patient with a large recurrent chordoma with resection up to S1–S2) were managed by BGMA flaps performed by our plastic surgery team (Fig. 1I, J). Two were managed by a V-Y myocutaneous advancement flap. These four patients had good healing without any wound complications. One patient with a partial sacrectomy in which the dead space was not managed by a plastic procedure developed a deep wound infection and needed wound debridement and subsequent treatment with intravenous antibiotics.
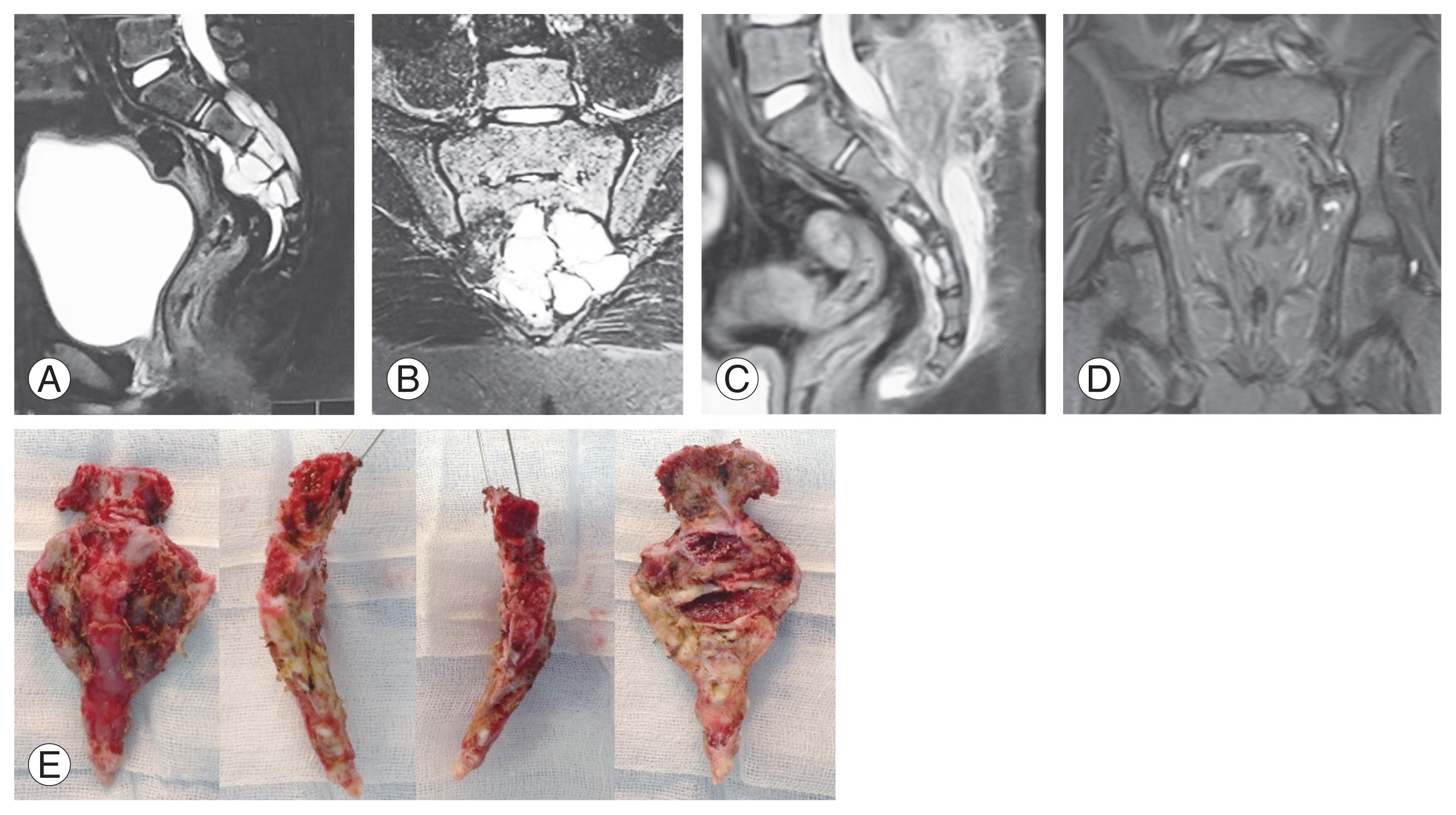
Chordomas are rare low-grade, slow-growing malignant bone tumors arising from the midline skeleton, most commonly from the sacrum. They are the most common primary sacral tumors and usually present after the fifth decade owing to their slow-growing nature and nonspecific clinical symptoms [35]. The extracompartmental extension at the time of presentation is the main predictor of the patient’s life expectancy [36]. Chordomas are known to have poor sensitivity to chemotherapy and radiotherapy, making surgical resection the gold standard treatment [35]. Surgical margins are defined according to the Enneking classification system as intralesional, marginal, wide, and radical. A meta-analysis by Yu et al. [35] concluded that the surgical margin is the most decisive factor in achieving good disease control in sacral chordomas. Recurrence rates were lower in patients with wide surgical margins in contrast to inadequate (intralesional and marginal excision) margins [35,37]. Most of the studies report a median overall survival rate of >5 years, and local recurrence and metastasis contributes to morbidity and mortality in these patients [35]. DSA followed by a preoperative TAE helps reduce blood loss and the time needed for surgical resection [31]. Seven of 17 patients in our study had chordomas, constituting the majority of our patients. Five cases were primary chordomas and were treated with en bloc resection with Enneking appropriate wide margins. An example of a surgically treated primary chordoma is illustrated (Fig. 3). There has been no recurrence to date (follow-up 1.5 to 5 years). Two patients had recurrent chordomas, one of who was treated with partial sacrectomy. The margins were inadequate on histopathological examination, and the patient had a recurrence at 2-year follow-up despite radiotherapy (Fig. 4). The other recurrent case was inoperable, with a large extracompartmental lesion and intrapelvic extension, and was treated with radiotherapy. More recent advents, such as carbon ion radiotherapy, proton beam therapy, and molecular targeted therapy agents (e.g., imatinib, temsirolimus) have been promising in treating recurrent inoperable chordomas [38–40].
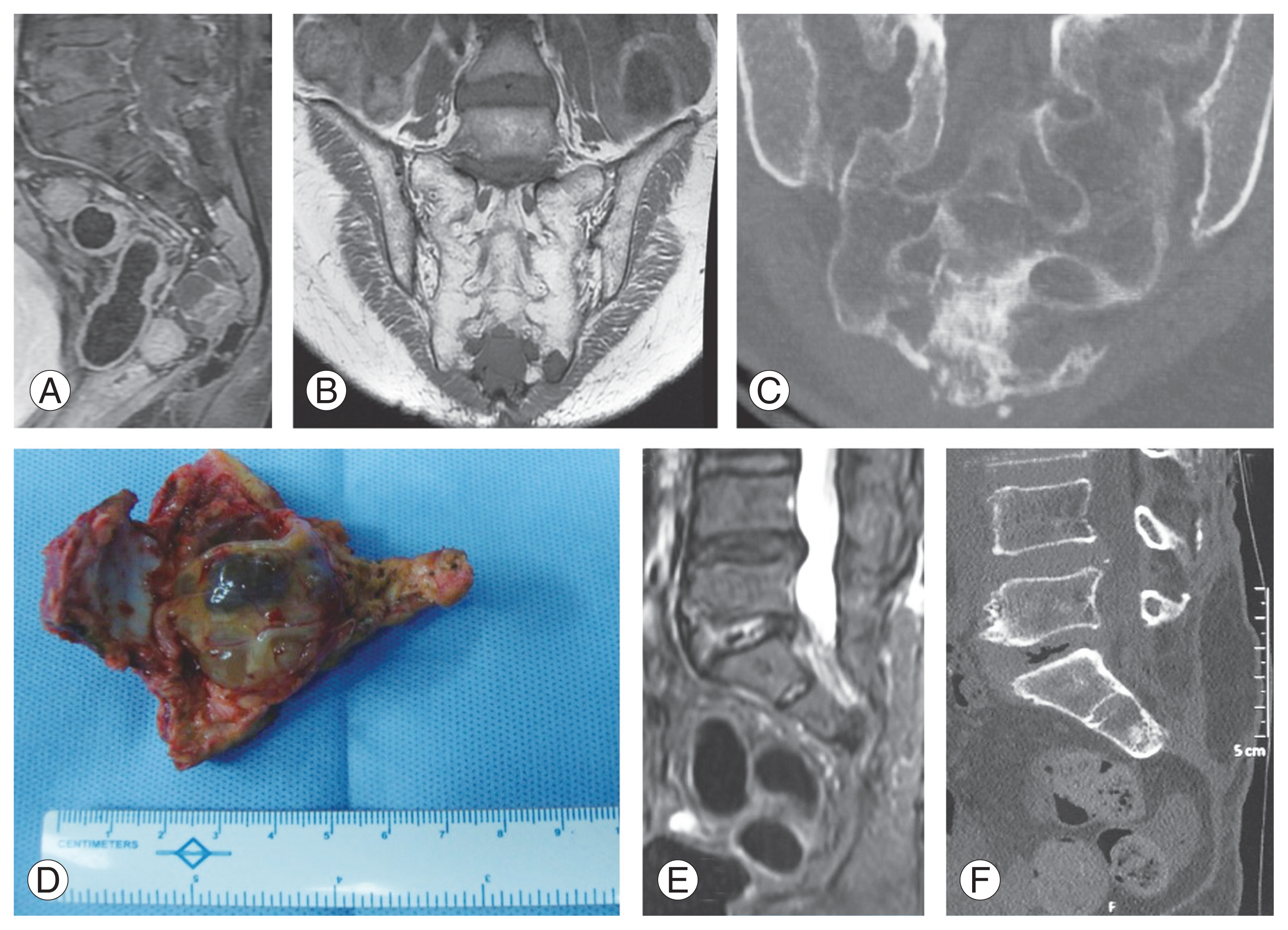
Schwannoma and neurofibroma are the two common benign tumors arising from intrasacral neural elements and are sometimes associated with giant presacral components in addition to intrasacral component. Despite the evolution of treatment strategies, surgical resection remains the optimal treatment [41]. A laminectomy is often sufficient to remove intrasacral tumors. However large presacral lesions might require partial sacral amputations: a blunt dissection of the tumor from the rectum before removing them. Owing to their benign nature, these neural tumors can be managed by marginal excision, given they have a distinct pseudo-capsule. We had two such patients with no presacral components who were managed by laminectomy/hemilaminectomy and marginal excision, taking care to preserve the sacral nerve roots using intraoperative neural monitoring. One of them is illustrated (Fig. 5). The local recurrence rate varies between 7% and 21%, and no treatment might be necessary unless symptomatic [41]. The neurological symptoms resolved completely in both of our patients, with no disease recurrence at follow-up.
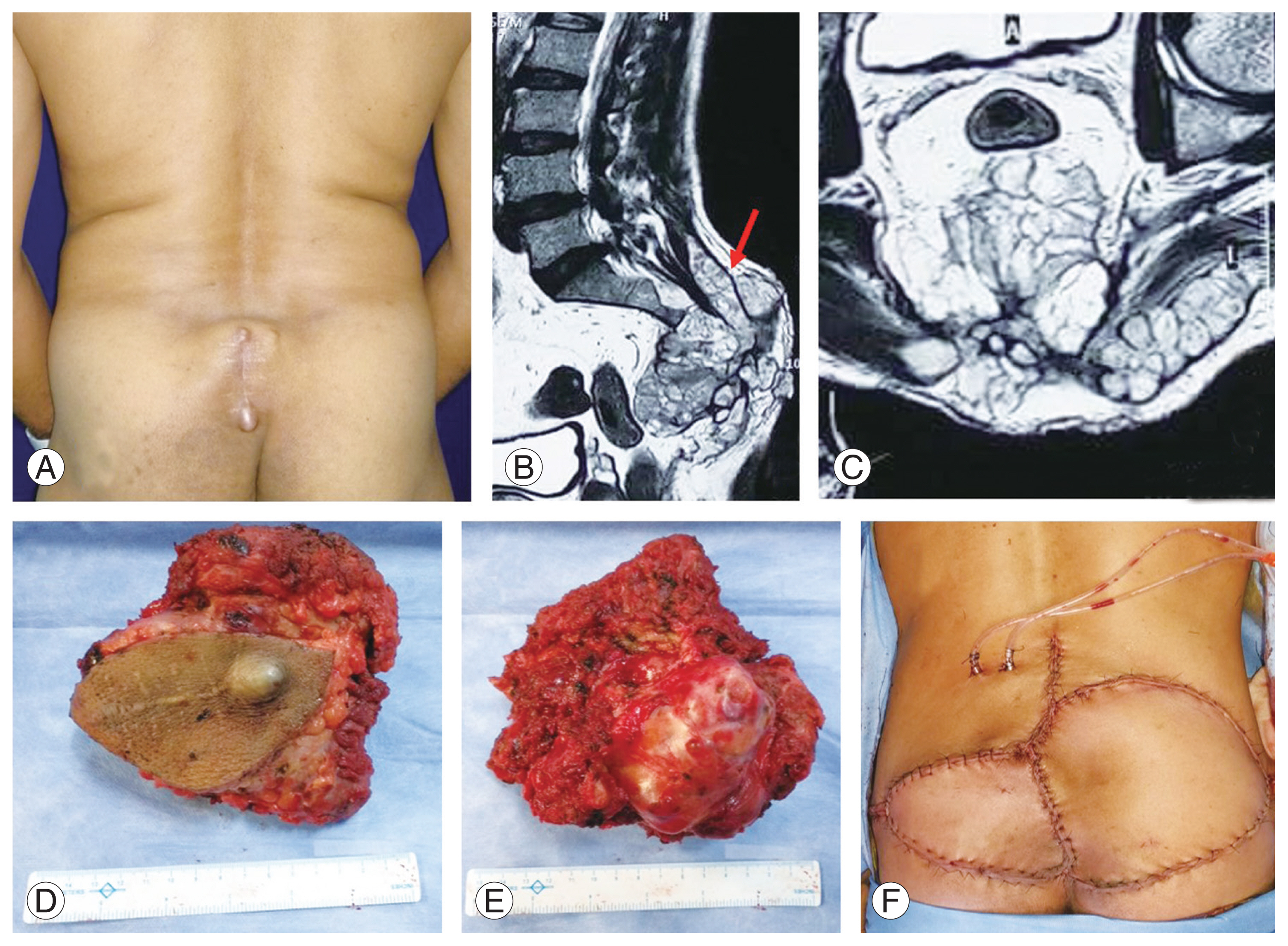
ES of the sacrum is a malignant tumor belonging to a group of small, round, blue cell neoplasms, differentiated from the other PNETs by neural and immune histochemical markers. They usually present in the first 2 decades of life and have an aggressive course. They are highly chemosensitive, making multiagent chemotherapy (neoadjuvant and adjuvant) the cornerstone of their treatment. Local disease control can be achieved by wide en bloc excision, radiotherapy, or both [42]. The superiority of either surgery or radiotherapy is still debated. Unlike ES of the extremities, surgery for sacral ES is complex because of the anatomy, with potential neurological compromise and inadequate margins. Although many authors advocate wide resection of the tumor as the only way of curing the disease locally [42,43], surgery with inadequate margins is associated with a high recurrence rate and a poorer prognosis. Following ES resection, chemotherapy-induced tumor necrosis is an important prognostic predictive factor to evaluate the efficacy of chemotherapy. With recent advances, radiotherapy provides good local control for ES, justifying its evaluation as an alternative to surgical treatment [42,44,45]. Hence, radiotherapy has a clear advantage over surgery in locally advanced tumors. We had two cases of sacral ES. One patient was an 11-year-old presenting with a large ES extending from S2 to S5, with bowel and bladder incontinence. He underwent six cycles of NAC (VAC/IE [vincristine+doxorubicin+cyclophosphamide alternating with ifosfamide+etoposide] regimen) over a 12-week period, which showed drastic shrinkage of the tumor (by 80%). He later underwent partial sacrectomy and adjuvant chemotherapy (Fig. 6). He regained bowel and bladder control and showed no signs of recurrence at the 1-year follow-up. Unfortunately, he succumbed to pulmonary infection and systemic sepsis later. The other patient with ES had a locally advanced tumor involving pelvic organs and was treated with chemotherapy and radiotherapy. He had no signs of local disease progression at 2-year follow-up.
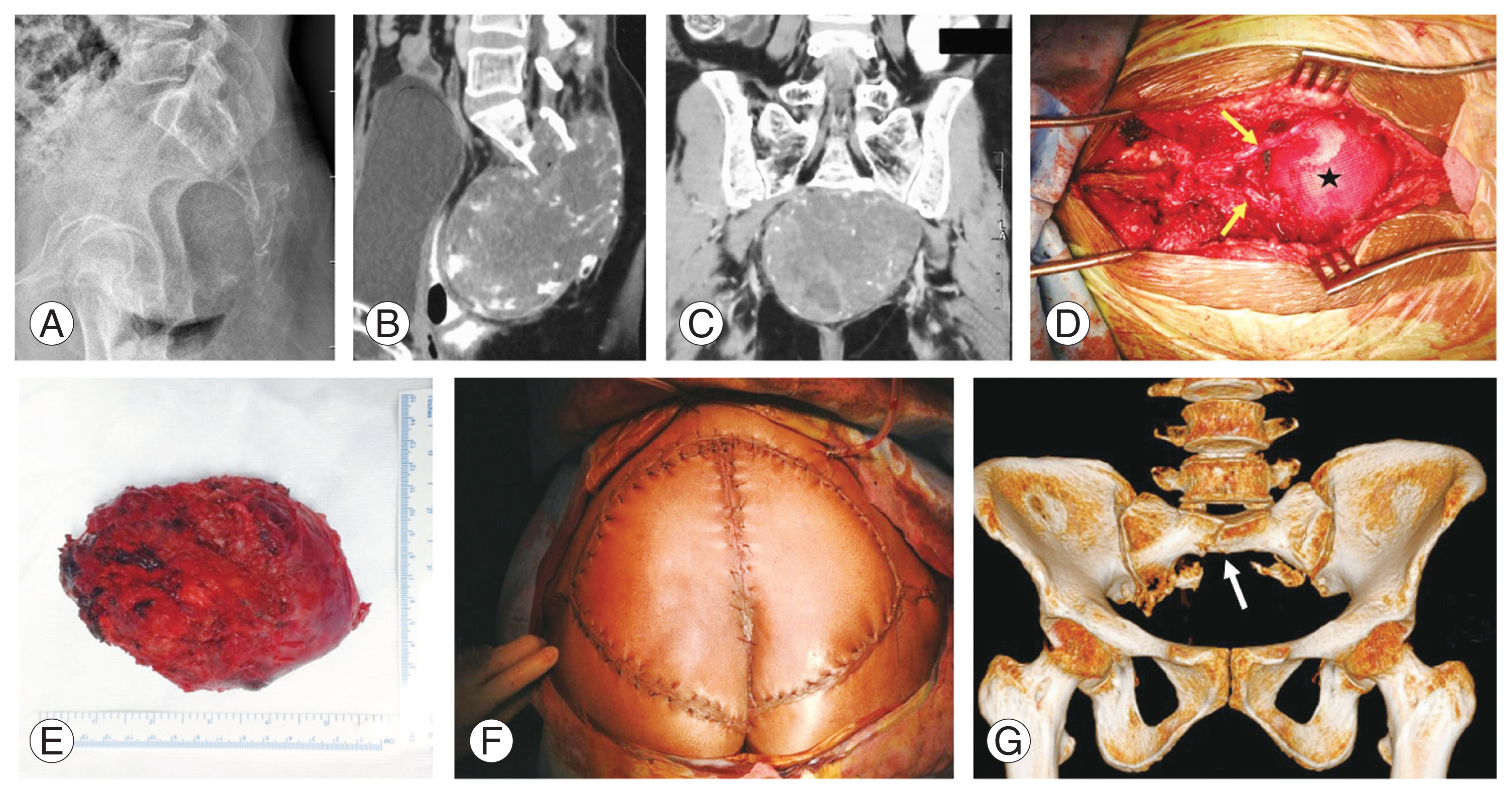
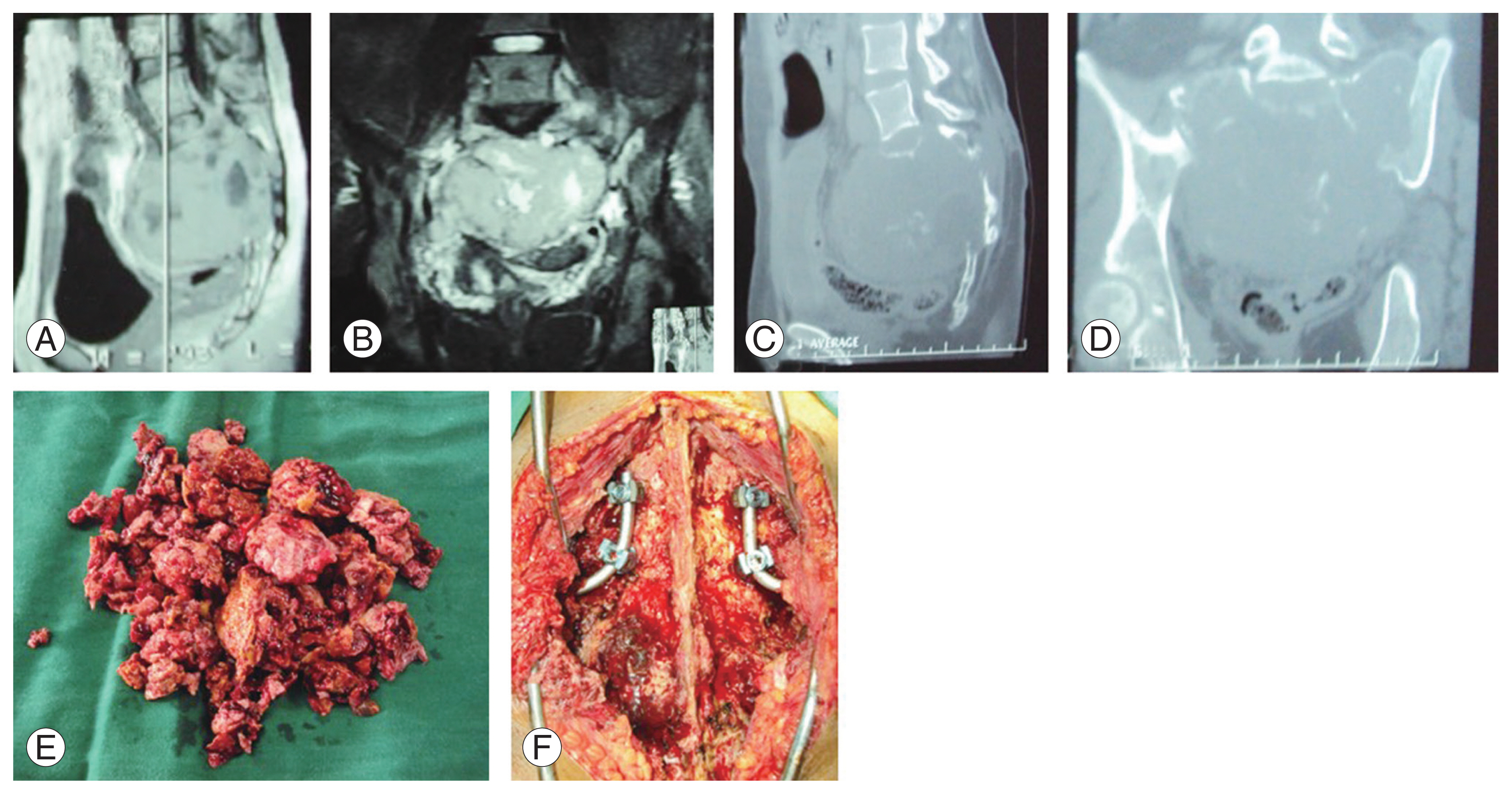
GCT is the most common benign sacral tumor in the literature [2,5,32]. Despite being termed benign, they possess locally aggressive characteristics and can metastasize to the lung [46]. Treatment options include surgery (intralesional curettage; marginal excision; wide excision), TAE, and radiotherapy. Intralesional curettage and marginal excision in high sacral GCTs might help preserve sacroiliac joint stability but are associated with higher recurrence rates and blood loss [32,46]. Adjuvants such as bone cement and liquid nitrogen have been proposed to reduce recurrence with limited results [47]. Wide excision with clear margins offers the lowest recurrence rates and less blood loss at the expense of stability, given the GCTs are often large and their wide resections involve the sacroiliac joint [48]. Preoperative TAE following a DSA helps in reducing blood loss and surgical time by reducing tumor vascularity [30]. Given our patient had a lesion extending up to S1, a total sacrectomy was performed after TAE, and lumbopelvic mesh reconstruction and stabilization were necessary (Fig. 7). Isolated radiotherapy in inoperable cases has been reported, with a high recurrence rate and risk of developing radiation-induced sarcomas [49]. Serial TAE has also been shown to cause shrinkage of large GCTs, with good pain relief and disease control, and can be useful for inoperable cases [50].
One patient in our study had a mucinous cystadenocarcinoma, which is a rare malignant tumor typically arising from the ovary, colon, or pancreas. They can also arise from the soft tissue surrounding the rectum with contiguous involvement of the sacrum [51]. Such isolated sacral lesions with no distant metastasis can still be surgically resected [52]. Our patient presented with urinary dysfunction and back pain and was diagnosed based on MRI showing a large presacral mass with a destructive lesion in the sacrum, and needle biopsy confirmed the diagnosis. The metastatic workup was negative. The patient underwent partial sacrectomy, with an added anterior procedure for removal of the rectal lesion and a colostomy. Postoperative chemotherapy and radiotherapy were also administered. The patient had no recurrence at 18-month follow-up.
Primary sacral lymphomas are very rare tumors presenting as destructive lesions with or without neural involvement. These are predominantly non-Hodgkin’s B-cell lymphomas (NHBL). They are highly chemo- and radiosensitive and rarely need surgical removal in instances such as severe neural dysfunction. Chemotherapy employing the chemotherapy regimen has been the standard of care. The recent advent of monoclonal antibodies such as rituximab demonstrates good disease-free survival in up to 85% of patients, especially when combined with field radiotherapy [53]. One of our sacral lesions turned out to be an NHBL and was treated by chemotherapy and radiotherapy with complete resolution of symptoms.
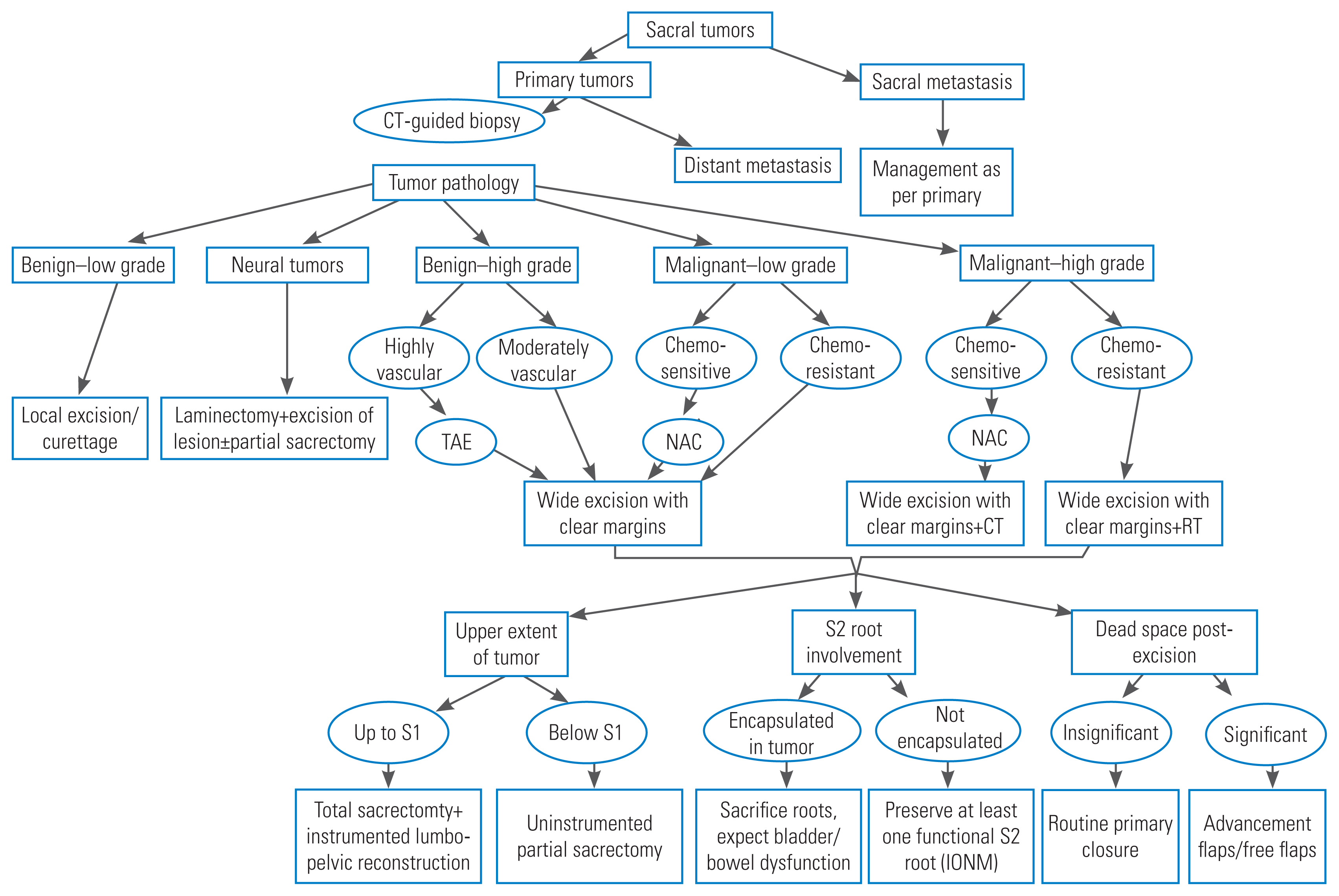
Based on our institutional experience and with input from the literary review, we have formulated a management algorithm to guide the investigation and treatment of primary sacral tumors (Fig. 8).
Limitations
We do recognize the limitations of our study. Being a retrospective study with a relatively small sample size, a prospective study on a larger group of patients is needed to generalize surgical outcomes. However, our recommended approach to any primary sacral tumor was based on our experience and a detailed review of the literature.
Conclusions
Management of primary sacral tumors needs a multidisciplinary approach comprising a team of specialists to optimize patient outcome. A stand-alone posterior approach can be used to treat most of the sacral lesions extending up to S1. An en bloc wide resection is the optimal treatment of primary malignant and aggressive benign tumors such as GCTs. Preservation of the S1 body and sacroiliac joint integrity is paramount to avoid lumbopelvic fixation. Preservation of at least one functional S2 nerve root is imperative to preserve bowel and bladder function.