Introduction
Ankylosing spondylosis (AS) is a well-known chronic inflammatory entity that mainly affects the axial skeleton. In Japan, the incidence of AS has been reported to be approximately 0.04% of the population [1], less than the reported prevalence in Caucasians, which is about 1% of the population [2]. Over the course of this disease, fracture is a major problem due to the combination of stiffness and osteoporosis [2,3]. The cervical spine is the main affected site for fracture, often caused by minor trauma such as falls [2]. A higher risk of concomitant neurological involvement is also a characteristic of cervical fracture in AS patients [2,3]. Both conservative treatment and surgery for spinal fractures in AS patients have been reported. However, each approach has drawbacks, and thus, controversy exists over the best treatment strategy [2-6]. We report the case of an elderly AS patient who sustained a cervical fracture with neurological involvement that was treated successfully by posterior fusion using the RRS Loop Spine System (DePuy Spine, Raynham, MA, USA).
Case Report
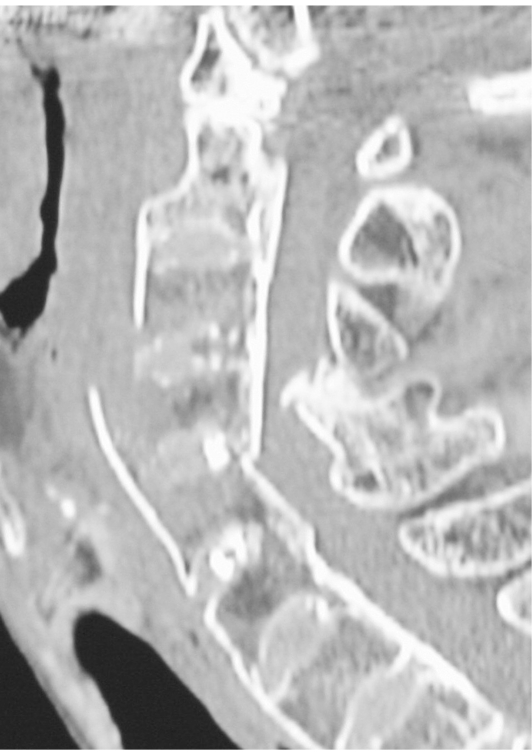
An 80-year-old woman presented with neck pain and moderate paraparesis of Frankel grade C after falling on stairs. A plain radiograph revealed a fracture of an ossified anterior longitudinal ligament at the C3-4 level with marked osteoporosis of the cervical spine and ossification of each disc, making the border between the endplate and disc unclear (Fig. 1). Computed tomography showed the fracture line more clearly, indicating a fracture of the posterior longitudinal ligament at the C4-5 level, and an ossification mass that was encroaching on the spinal canal at the C3 to C4 level was identified (Fig. 2). A plain radiograph of the sacroiliac joint showed complete ankylosis and typical features of bamboo spine of the lumbar column that were consistent with AS. The patient's neurological status did not change despite improved cervical alignment at the fracture site and neck pain relief after Halo immobilization. These neurological deficits were a burden due to the elderly and paralytic status of this patient and caused diminished motivation and nocturnal delirium. Moreover, poor adaptation to the Halo-vest due to the patient's thoracic kyphosis and scoliosis led to a decubitus ulcer formation on her back. As a result of these conditions, surgery was selected as the treatment strategy.
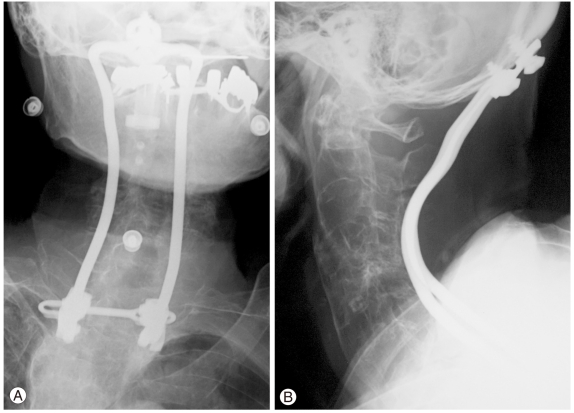
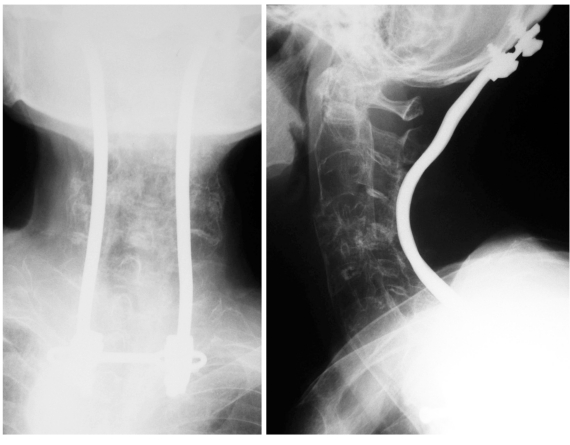
The patient was set in a prone position with a Halo-vest and pillows underneath her body. The back side of the Halo-vest was removed temporarily to provide access for surgery. A posterior longitudinal incision was made from the external occipital protuberance to the T3 level. The posterior bony elements were clearly so brittle that the end of a spinal process broke merely on pinching with fingertips. The laminae of C4 and C5 had sunk between C3 and C6, but the fracture site was unclear. An RRS Loop Spine System (DePuy Spine) was applied from the immobilized occipital bone to T3. Laminar hooks were placed in the T3 lamina, and sublaminar banding using polyethylene tape (Nesplon, Alfresa Pharma, Osaka, Japan) was added at the C2, C7, and T1 laminae to secure fixation (Fig. 3). The laminae and ossified ligamentum flavum of both C4 and C5 were removed for decompression; no extradural hematoma was observed. Her postoperative course was unremarkable. The Halo-vest was removed immediately after surgery, and a cervicothoracic orthosis was fitted. Her neurological state recovered to Frankel D1, and she noticed the clumsiness in her hands was alleviated. Although neurological improvement was minor, her motivation increased, and pain from her neck and the decubitus ulcer disappeared. Progressive bone formation was confirmed on a plain radiograph three months after surgery (Fig. 4). She lived at the rehabilitation institute after discharge from our hospital and had no complaint of neck pain 17 months after surgery although improvement in her daily activities was limited (Fig. 5).
Discussion
The rigid spines in AS are susceptible to fractures, and the cervical spine is a major site of those injuries; furthermore, the rate of neurological involvement is high [1,4,7,8]. Although definite guidelines have not yet been established for the best treatment option of such fractures, reports of surgical treatment have increased while devices used in treatment have improved [3,4,8]. Posterior longer internal fixation with a bone graft has become mainstream using a lateral mass screw or pedicle screw system; if necessary, some surgeons also prefer concomitant anterior plating. In the current case, a fracture line ran obliquely from the anterior C3-4 level to the posterior C4-5 level and was associated with great instability. Long and rigid internal fixation was essential due to the marked osteoporosis induced by both AS and aging; however, only C2 and C3 seemed to be usable anchors on the proximal side for fixation. Additionally, the patient's small physique and relatively small bones made screw insertion difficult at the upper cervical level. Therefore, we designed a long fusion from the occipit to the upper thoracic level to achieve a rigid internal fixation. On one hand, more rigid fixation would be expected extending fixation-end to the occipit, but on the other, there is a drawback of obliterating the mobile segment at the craniovertebral junction. Additional unintended surgery seemed to be difficult in this patient when loosening or dislodgement of screws occurred, and we chose the long fusion from occipit to upper thoracic spine. The RRS Loop Spine System developed by Shimizu et al. [5] (Fig. 6) is an instrumentation device for occipitocervical or occipit-upper thoracic fixation and has a unique occipit screw that has a design inspired by the screw used to bind a snow ski to its binding. This occipit screw enables secure fixation monocortically between the occipit bone and device. The rod, 4.76 mm in diameter, also contributes to rigid fixation of the spinal column. In the literature, the diagnoses of patients treated with this system have been mainly rheumatoid arthritis-related disorders or unstable anomalies of the craniocervical junction [5,6,9]. This system could provide the solution for hyperextension injuries of the cervical spine, especially in the upper cervical region. Using the occipit as an anchor, stable fixation could be accomplished even in the case of an elderly patient or complex high-energy fracture with great instability [10]. The connection between rod and vertebra is via a pedicle screw, hook, or sublaminar wiring in a similar manner to other instrumentation devices. We selected sublaminar banding by polyethylene tape and hook placement at the lower end lamina so that the stress caused by the instrumentation would be dispersed evenly through the occipit to the upper thoracic spine in this markedly osteoporotic patient. Our procedure seems to be one of the surgical methods that can successfully stabilize the spinal column depending on the fracture site despite the disadvantage of fixation to the occipit bone.