Introduction
Kyphotic deformities of the spine are complex surgical problems and can develop secondary to multitudinous pathologies [1-5]. Although degenerative scoliosis and spondyloarthropathies diffusely involve almost the entire spine [6,7], pathologies in other congenital, postinfective, posttraumatic, or iatrogenic deformities tend to be predominantly limited to a few vertebral segments [3-5]. In addition, although some of these deformities such as ankylosing spondylitis are associated with the underlying rigid spine [6], certain conditions such as postinfective or posttraumatic kyphosis occur consequent to bony or soft tissue deficiencies of the involved vertebrae [3-5]. Considering such diverse associated issues, an appropriate management of these deformities necessitates a complete understanding and a thorough assessment of all global and local factors related to the spinal column [1-7]. Therefore, the development of a universal nomenclature and a classification system incorporating each of these individual factors is of utmost significance to ensure the best possible treatment protocol for managing these complicated sagittal deformities [8-11].
The classifications proposed by King et al. [10] and Lenke et al. [11] have standardized and streamlined the management of coronal deformities in idiopathic scoliosis. However, such comprehensive classifications that could guide the management protocol in sagittal kyphotic deformities were not available in the past [9]. An ideal classification system helps in good communication among physicians, and such a system should be simple and easy to apply, reproduce, and focus specifically on the characteristics that are most relevant to the treatment planning and prognostication [8]. In 2018, Rajasekaran et al. [9] had proposed the new classification system, taking into consideration major factors, including flexibility of the spine, magnitude of the sagittal deformity, extent of deficiency of the anterior or posterior vertebral columns, and the osteotomy type that would be typically recommended for the deformity. This classification has demonstrated good reliability and accuracy when applied among surgeons in the parent institution. However, till date, no study has analyzed the inter-rater reliability of this classification among surgeons from different institutions. Therefore, the present international, multicentered, collaborative research project involving 12 spine surgeons from six different countries was conducted to evaluate the interobserver reliability of this classification, the diagnostic accuracy of each type of deformity, and the reliability of treatment recommendations based on this classification.
Materials and Methods
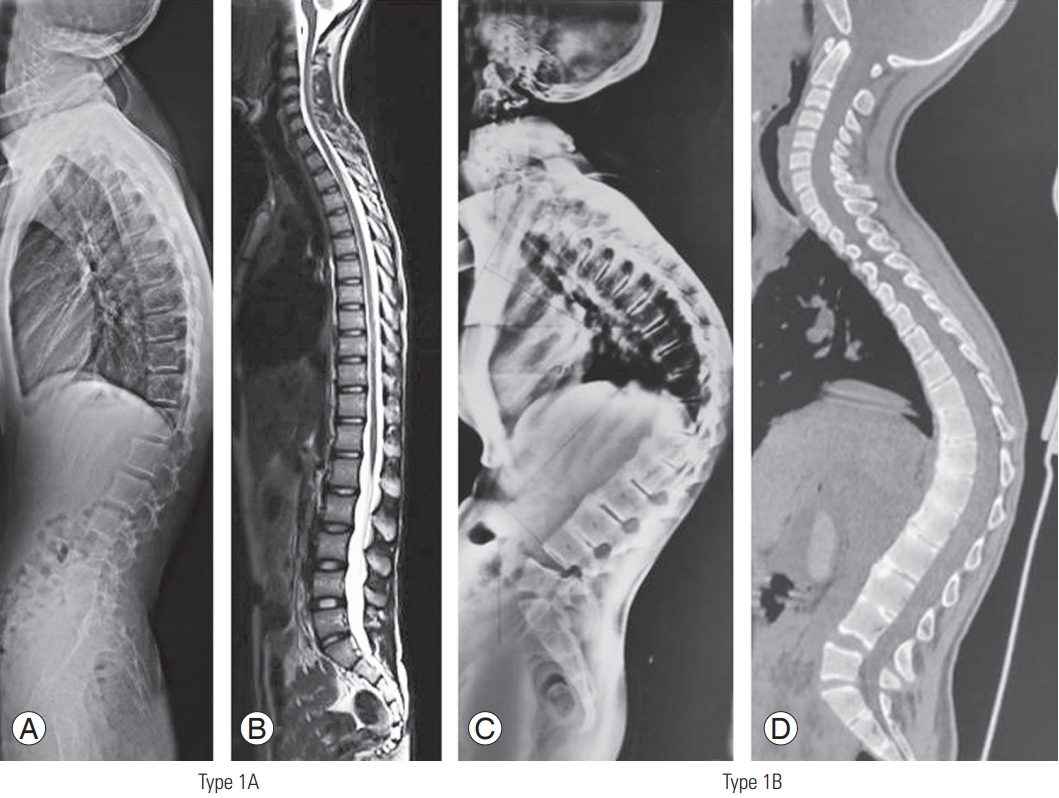
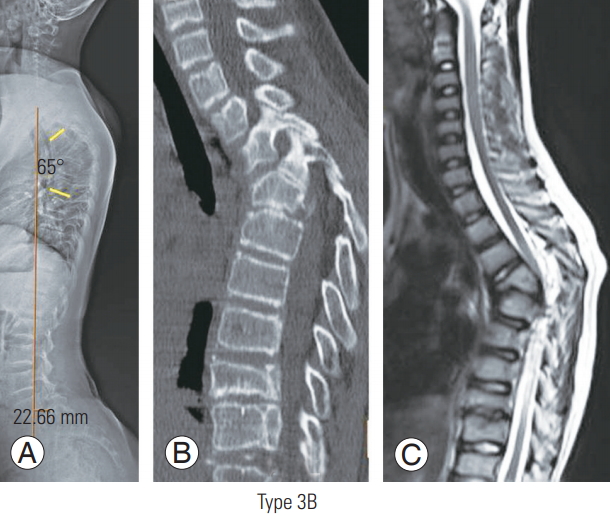
A total of 30 sets of images, including plain whole spine radiographs (anteroposterior and lateral views), computed tomography scans, and magnetic resonance imaging scans, were classified based on the novel kyphosis classification system as described by Rajasekaran et al. [9]. This is a morphology-based classification system based on the following major factors: (1) extent of anterior and posterior deficiency, (2) magnitude of curve deformity, (3) flexibility of spine, and (4) type of osteotomy (Figs. 1–5).
All images were classified initially by one senior spine registrar and one senior spine fellow, who are well trained in this classification system independently, and further ratified by two senior authors (A.P.S. and R.M.K.), both from the same institution as the primary developer of this classification. These recommendations were considered as the standard for the purpose of analysis. Institutional Review Board approval was obtained from the institute of the primary investigator (IRB approval no., 2019/02/01; Ganga Medical Center and Hospital, Coimbatore, India), from where all the images were obtained, before the commencement of this study. All patients provided written informed consent for the publication of clinical details and images.
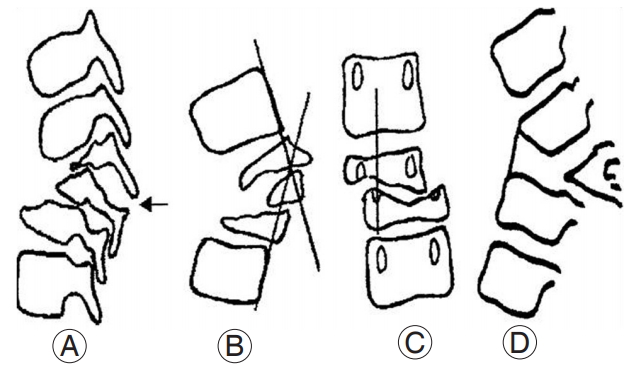
Based on the column deficiency, the curves were broadly classified as type 1 (no column deficiency), type 2 (one-column [anterior or posterior] deficiency), and type 3 (both columns deficient). Type 1 curves were further subdivided as follows: 1A (flexible disc spaces present) and 1B (immobile disc spaces; e.g., ankylosing spondylitis). Type 2 curves were subdivided based on the column that is deficient as follows: 2A (deficient anterior column only) and 2B (deficient posterior column only). Type 3 curves were further subclassified into the following three categories: 3A (Cobb angle <60°) 3B (Cobb angle >60°), and 3C (buckling collapse present). Two additional modifiers were included in this classification, one for global sagittal balance and the other for coronal deformity. The global sagittal balance was assigned M- (sagittal vertical axis [SVA] deviation of <5 cm) or M+ (SVA ≥5 cm). The coronal modifiers were C- for coronal Cobb angle <20° and C+ for coronal Cobb angle ≥20°. Based on the recommendations of this classification system, the management protocol for each deformity type was put forth.
We shared all the images with 12 different spine surgeons from the Asia-Pacific region in three different phases. The surgeons were initially educated about the classification system by sharing detailed power-point presentations describing the classification and osteotomy recommendations. This multicentered study was supported by the financial grant provided by the Asia-Pacific Spine Society.
Next, a questionnaire was shared with each participant spine surgeon involving the following questions: (1) What is the type of deformity based on kyphosis classification (as described by Rajasekaran et al. [9]); (2) What is the global sagittal modifier (M- or M+)?; (3) What is the coronal modifier (C- or C+)?; and (4) What is the surgical approach or intervention that you would consider for this deformity (including any additional procedures)?
All the questions and responses from each responder were entered on the online survey development cloud-based software “SurveyMonkey” (SurveyMonkey, San Mateo, CA, USA). All responses and entries made in the registry were blinded. After the completion of all the three phases of data collection, the obtained data were compiled by two independent researchers (one senior fellow and one junior spine consultant). All data were analyzed and presented, vide infra.
The inter-rater reliability and accuracy were calculated (by comparing each evaluator’s recommendations with the standard recommendations) for each type of deformity and surgical recommendations using percentage (%) correlation and kappa (Cohen and Fleiss) correlation, Kendall correlation coefficient, and intraclass correlation. Furthermore, the internal consistency among the evaluators was compared using Cronbach’s α correlation and correlation matrices.
Results
We received responses from all 12 volunteers during phase 1 evaluation, from 11 volunteers during phase 2 evaluation, and from only 10 volunteers during phase 3 evaluation (Table 1). For detailed validation analyses, complete evaluations from only the first 10 respondents could be included. Based on our evaluations (by surgeons of our institution), there were six patients with type 1 deformity, two patients with type 2 deformity, and 22 patients with type 3 deformity. Thus, a majority of patients belonged to type 3 deformity.
1. Deformity classification
With respect to the type of deformity, the surgeons of the parent institution had classified five deformities as type 1A, one each under types 1B, 2A, and 2B; five deformities as type 3A; 15 deformities as type 3B; and two deformities as type 3C. Among those patients whom the surgeons of the parent institution had classified as having types 1A and 1B deformities, 86.4% and 83.3% of the respondents had classified under the same category, respectively. Similarly, among the deformities that were diagnosed by the parent institution surgeons as types 2A and 2B, 50% and 58.3% were classified by the volunteers under the same subtypes, respectively. Among those patients whose deformities were classified under types 3A, 3B, and 3C, 33.9%, 67.1%, and 95.5% were also respectively classified under the same category by the other evaluators. The distribution of the different types of deformity, as classified by each surgeon, is shown in Tables 1 and 2.
Overall, when the response of each evaluator (with regard to the deformity type) was individually compared with the standard, the percentage correlation ranged between 56.7% and 86.7%, and Cohen’s kappa coefficient ranged between 0.43 and 0.81 (Kendall coefficient ranged between 0.73 and 0.90, and intraclass correlation coefficient was 0.97) (Table 3). Excellent inter-rater reliability is defined by a kappa coefficient >0.80. We observed a fairly good internal consistency among the evaluators based on Cronbach’s α ranging between 0.958 and 0.963 (Table 3).
There was an excellent consistency between the surgeons in the reporting of types 1A, 1B, and 3C deformities (kappa coefficients, 0.88, 0.78, and 0.86, respectively). There was moderate consistency and repeatability with respect to types 2B and 3B deformities (kappa coefficients, 0.50 and 0.63, respectively). Low reliability was observed for deformities of types 2A and 3A. The kappa coefficient for type 2A deformities could not be reported because of only a single case in this category and significant variation among the respondents. The kappa coefficient for type 3A deformities was 0.40 (Table 4). For each type of deformity as classified by the surgeons of the parent institution, the classification proposed by each of the volunteer is also shown in Table 2.
2. Global sagittal balance and coronal deformities
The deformities were classified on the basis of global sagittal and coronal modifiers as M- and M+ and C- and C+. There were five patients who were classified under M+ and C+ categories each and 25 patients each under M- and C-categories. The distribution of the classification of global sagittal and coronal modifiers among the spine surgeons is presented in Table 3. Among those patients whom the parent institution surgeons had classified into C+ and C-categories, 76.8% (43 of 56 responses) and 98.9% (271 of 274 responses) of the respondents also classified in a similar manner, respectively. Among those patients whom the surgeons of the parent institution had classified into M+ and M- categories, 82.5% (47 of 57 responses) and 89.4% (244 of 273 responses) of the respondents also classified under the same category, respectively. Our observations indicated good reproducibility in the interpretation of the global sagittal and coronal modifiers (Table 5).
3. Type of osteotomy or deformity correction required
Based on the recommendations purported by Rajasekaran et al. [9], the type of osteotomy for each deformity was also discussed. The surgeons of the parent institution had recommended type 2 (Ponte) osteotomy in five patients (16.7%), type 3 or 4 (pedicle subtraction/disc-bone osteotomy, PSO/DBO) in seven patients (23.3%), type 5 (vertebral column resection, VCR) in 12 patients (40%), type 6 (multilevel VCRs) in five patients (16.7%), and staged VCR (halo-gravity traction followed by VCR) in one patient (3.3%) (Table 6).
We received a total of 342 responses from the different participating spine surgeons who recommended their preferred surgical interventions for each deformity. The total recommended surgical interventions included 73 (21.3%) Ponte’s osteotomies, 90 (26.3%) PSO/DBOs, 115 (33.6%) VCRs, 49 (14.3%) multilevel VCRs, 12 (3.5%) anterior in-situ fusions with graft, and 2 (0.5%) staged VCRs (halogravity traction followed by VCR). For one patient, one of the surgeons had recommended no surgical deformity correction. For nine deformities, five surgeons had recommended more than one surgical option. One of these deformities was classified as type 1A, one was classified as type 2B, five were classified under type 3B, and two were classified under type 3C.
Among those patients for whom the parent institution surgeons had recommended type 2 (Ponte) osteotomy, type 3 or 4 (PSO/DBO), type 5 (VCR), type 6 (multilevel VCR), anterior in-situ fusion with graft, and two-staged VCR (based on the classification), the evaluators concurred with the standard on 96.3%, 67.5%, 64.1%, 45.5%, and 10% of the cases, respectively. When each respondent’s choices were compared with the standard, the percentage correlation coefficient ranged between 50% and 83.3% and the kappa correlation ranged between 0.3 and 0.77 (Table 7). Among them, the evaluators showed a fair degree of internal consistency in their choice for osteotomy based on Cronbach’s α correlation ranging between 0.973 and 0.977 (Table 7). With respect to the osteotomy choices, there was an excellent inter-rater correlation for the recommendation of type 2 osteotomy (kappa coefficient=0.80). However, for the other procedures, the kappa value was quite low (ranging between 0.3 and 0.52) (Table 8).
Discussion
Unlike scoliosis, kyphotic deformities occur due to a multitude of etiologies and are frequently accompanied by varying degrees of deficiency of the anterior and posterior columns, which determine the prognosis and management decisions [12-14]. In 2018, Rajasekaran et al. [9] proposed a kyphosis classification system based on column deficiency, curve magnitude, and osteotomy requirement. They incorporated the six different types of surgical osteotomies described by Schwab [15] and also added a seventh option of anterior fusion with strut grafts without major correction for patients with buckling collapse. They also demonstrated good correlation with their classification and the complexity of the osteotomy required. However, the results were derived from a single center and no multicenter validation was available. Through the present study, we are providing the results from a multicenter validation on the interobservor correlation for various types with classification and also the correlation with the surgeon’s choice of osteotomy.
1. Deformity classification
As previously mentioned, the rationale behind the current classification is that the greater the loss of column integrity, the more complex is the kyphotic deformity. In type 1 deformity, the columns are intact; in type 2 deformity, the integrity of one column is violated; and in type 3 deformities, the integrities of both columns are lost. In the present study, there was an excellent consistency among the surgeons in the reporting of type 1A, 1B, and 3C deformities. There was moderate consistency and repeatability with regard to types 2B and 3B deformities. However, for types 2A and 3A deformities, we observed a lower inter-rater accuracy.
Most of these variations were secondary to the discrepancies in distinguishing between single- and two-column deficiencies. Although the surgeons of the parent institution had classified only two deformities under type 2 category and 20 deformities under type 3A or 3B category, a significant proportion of these type 3 deformities were classified by the other respondents under type 2 category. This variation was caused due to surgeons concentrating primarily on the anterior column in their radiological assessment and failing to notice posterior column failure either by facet subluxation or by frank dislocation. However, the differentiation between types 2 and 3 deformities is clinically very important as it has important biomechanical implications and changes the management protocol. In general, among type 2 deformities, type 2A deformity involves the loss of integrity of only the anterior column [3,4]. When such deformities are caused secondary to the partial loss of vertebrae, the kyphosis is gradual. However, when there is a complete loss of one or more vertebrae, angular kyphosis ensues [16]. Type 2B deformities result from posterior soft tissue (tension band) or posterior bony loss (e.g., laminectomy) [17,18]. Type 3 deformities, involving the loss of both columns, have a poor prognosis for curve progression, instability, and buckling collapse [19]. Whenever there is a type 3 curve of magnitude >60°, there is a relatively greater risk for progression, instability, and buckling collapse [2]. In type 2A deformities, although the deficiency of the anterior column is structural, the progression of the deformity can lead to functional failure of the posterior column (predominantly involving facet subluxation or dislocation). Such deformities must be promptly recognized as “impending type 3A deformities,” as described in our original article [9]. We do believe that in any patient with kyphosis >60° magnitude and positive “spine at risk” signs (described by Rajasekaran [20] for the prediction of progression of pediatric kyphosis), the loss of posterior column should be strongly suspected (Fig. 6).
2. Intactness of posterior column
The classification is based on the integrity and extent of loss of columns; hence, the accurate identification of the column loss is important. We found that there was no discrepancy in the assessment at the two ends of the spectrum—where there is no column loss (types 1A and 1B) or where there was a severe loss of both columns (type 3C). The major emphasis of the current classification is the identification of the intactness or deficiency of posterior column based on radiological findings.
The biomechanics of the spine, especially in children, is determined by the “Euler’s laws of slender column” [21]. Evaluation of impairment of the posterior column is of utmost significance in understanding the evolution of type 3 kyphotic deformities. Although the loss of anterior column is always structural, the failure of the posterior column in several instances is consequent to a functional failure involving facet subluxation. Pathologies such as tuberculosis, congenital vertebral anomalies, achondroplasia, and posttraumatic kyphosis can present with perched, subluxed, or dislocated facets, which leads to confusion between type 2A and type 3A deformities. In biomechanical terms, failure of both columns is termed as “death of the column” following which precipitous collapse and increase in deformity are predicted. Although surgeons are quite adept at identifying the structural loss of the anterior column, there is often a lack of recognition to identify a posterior column failure or facet dislocation [22,23]. This was the reason for the low interobserver agreement value and the more frequent classification under type 2 category in cases that were actually type 3. Figs. 7 and 8 demonstrate two such cases that were classified originally as types 3A and 3B, respectively (according to the standard recommendation). However, the classification of the deformity in these two patients by the participant spine surgeons varied significantly due to the inconsistencies in the recognition of the posterior column discontinuity. Although the imaging shown in Fig. 7 (type 3A) was classified under types 3A, 2A, and 3B by 18%, 73%, and 9% of the respondents, respectively, the type 3B deformity shown in Fig. 8 was classified as types 3B and 2A by 63.6% and 36.4% of the respondents, respectively.
We consider this issue not as a problem of the classification but as an important clinical value of the classification itself, as it will now help surgeons focus on the status of the facet and accurately classify patients belonging to type 3. This will benefit patients through early and appropriate intervention and prevent progression under observation.
3. Global sagittal balance and coronal modifiers
The global sagittal balance is an important parameter to be considered in the management of kyphotic deformities. As the ultimate goal of managing these deformities is to optimally restore the anatomical sagittal profile of the patient, the significance of including this radiological parameter into any kyphosis classification system cannot be understated [24,25]. We included a deviation of >5 cm in both directions (positive or negative sagittal imbalance) under sagittal imbalance (M+ global sagittal modifier). Another parameter, which is of utmost importance in assessing any sagittal spinal deformity, is the associated coronal deformity [26,27]. We included a cut-off value of 20° to include patients with significant coronal deformity (C+). These two parameters are components of the Scoliosis Research Society–Schwab adult spinal deformity classification. Knowledge of these two parameters not only helps in providing greater uniformity to kyphosis nomenclature but also helps in evaluating the overall balance of the spinal column and devising appropriate management strategies for these deformities. As mentioned earlier, there was good consensus among the assessors in describing these modifiers.
We observed a significant correlation among the respondents regarding the classification of global sagittal and coronal modifiers in these patients. The surgeons of the parent institution had classified five patients each under M+ (global sagittal modifier) and C+ (coronal modifier) categories, respectively. Overall, there was good (82.5% and 77%, respectively) repeatability in classifying the “global sagittal” and “coronal” modifiers.
4. Type of osteotomy or deformity correction required
Based on our classification, we made recommendations for the osteotomy and the correction technique for each kyphotic deformity type. In type 1 curves, the deformity correction typically involves Schwab type 2 (if disc spaces are open) or type 3/4 (if disc spaces are fused) osteotomies. In type 2 deformities, the osteotomy is proposed based on the magnitude of the deformity. In type 2A deformities of <30° magnitude, Schwab type 2 osteotomies may be recommended, and in type 2A deformities of >30° magnitude and type 2B deformities, type 3 or 4 osteotomies may be required. In type 3A or 3B deformities, Schwab type 4, 5, or 6 osteotomies are necessary. When buckling collapse (type 3C) develops, staged deformity correction procedures or in-situ fusions generally offer the safest outcome. The rationale underlying these recommendations is the progressive degrees of curve complexity and the need for more complex corrective measures with each deformity type.
The surgeons of the parent institution had recommended Schwab type 5 (VCR) osteotomy in 40% (12 patients), types 3 or 4 (PSO/DBO) osteotomy in 23.3% (seven patients), types 2 (Ponte) and 6 (multilevel VCRs) osteotomies in 16.7% (five patients) each, and multistaged osteotomy in one patient. Among the total 342 responses from the participating spine surgeons, 33.6% (115) of the recommended procedures were type 5 (VCR) osteotomies, 26.3% (90) were types 3 or 4 (PSO/DBO) osteotomies, 21.3% (73) were type 2 (Ponte) osteotomies, 14.3% (49) were type 6 (multilevel VCRs), and 3.5% included anterior in-situ fusions. The consensus among the evaluators was excellent for deformities requiring type 2 osteotomies. However, a wide variation was detected among the surgeons regarding the choice of PSO and vertebrectomy. This can be explained by their institutional preferences and surgeons’ experience. Similarly, the anterior strut grafting without major correction procedure is a valuable option in very severe cases where any form of correction will be dangerous. However, this is not very frequently performed and hence several surgeons opt for the other alternative of vertebrectomy.
5. Limitations
The major limitation of this study was the relatively smaller number of cases, with the significantly smaller number of patients belonging to types 2A and 2B. No formal power analysis was performed to select the number of patients under each subgroup. Further studies may be planned in future to validate the kyphosis classification system, considering these drawbacks. All the entries by the respondents were made on the online “SurveyMonkey” software program in a blinded manner. Any stratification of the experience of spine surgeons and its correlation with their understanding of the classification was out of scope of this study.
Conclusions
Based on our results, there was excellent accuracy in the assessment of the deformities at the two ends of the spectrum, namely types 1A, 1B (with no column deficiency), and 3C (severe loss of both columns). However, surgeons classified more severe type 3 deformities as type 2, frequently not identifying facet subluxation or dislocation. Following this classification will prevent this error and help the surgeon to intervene appropriately.