Comparison of Radiological and Clinical Outcomes between Expandable and Non-expandable Cages Following Cervical Corpectomy: A Systematic Review and Meta-analysis
Article information

Abstract
Anterior cervical corpectomy and fusion is considered the mainstay of surgical treatment in cervical pathology. Expandable and non-expandable cages are preferred over autogenous bone graft because of donor-related morbidity. However, the choice of the cage type remains a debatable topic as studies report conflicting results. Thus, we evaluated the outcomes of expandable and non-expandable cages following cervical corpectomy. Studies were searched in various electronic databases (MEDLINE, PubMed, EMBASE, CINAHL, Scopus, and Cochrane) between 2011 and 2021. Forest plot was made to compare the radiological and clinical outcomes between expandable and non-expandable cages following cervical corpectomy. Altogether, 26 studies (1,170 patients) were included in the meta-analysis. The mean change in segmental angle was significantly greater in the expandable cage group than in the non-expandable cage group (6.7° vs. 3.0°, p<0.001). The mean subsidence rate was lower in the expandable cage group (6% vs. 41%, p<0.001). The mean fusion rate was lower (93% vs. 98%, p=0.06) and the mean displacement rate was significantly higher in the expandable cage group (29% vs. 5%, p<0.05). The mean reoperation rate was higher in the expandable cage group (16% vs. 2%, p>0.05). The improvement in segmental angle is better with expandable cages. Higher subsidence is a major problem with non-expandable cages, but it seems to be beneficial as evidenced by the high fusion rate and minimal effect on clinical outcome in patients with this cage.
Introduction
In various cervical pathologies, anterior cervical corpectomy and fusion is considered the mainstay in surgical treatment. Decompression of neural structures along with immediate fixation of the affected segments can be attained simultaneously [1]. It allows adequate exposure and decompression with improvement in the long-term outcome [2,3]. After cervical corpectomy, the defect is reconstructed with an implant or graft. The most acceptable graft or implant device should provide primary stability with deformity correction, anterior support that is resistant to the axial load, and a good contact surface with adjacent vertebral endplates to enable early fusion [4]. Autogenous bone graft is still used for reconstruction but it has its own donor-related morbidity. Thus, expandable and non-expandable vertebral body replacement (VBR) cages are preferred over autogenous bone graft in many circumstances wherever possible because of their low complication rate [5]. However, the choice of implant device for interbody fusion following cervical corpectomy remains a debatable topic owing to conflicting results. Moreover, implant selection also depends on the surgeons’ preference and pathological type [6]. Contrarily, VBR cages are not completely devoid of complications, as few complications, including non-union, graft displacement, and subsidence, have been consistently reported throughout the literature [7]. One important goal of interbody fusion is to achieve the appropriate cervical alignment because it allows to tolerate the axial load of the head, optimizes forward gaze, and supports head and neck movements [8]. Although a titanium mesh cage (TMC) has its own advantages, it requires the preparation of the implant to have a size that exactly matches the corpectomy defect. Size adjustment made by cutting the cage during placement can cause implant malalignment predisposing to construct failure. Additionally, repeated cage removal to correct malalignment usually damages the vertebral endplate. To overcome the technical disadvantages of non-expandable cages, several expandable cages have been introduced. These cages have a unique merit in terms of in-situ height adjustment and deformity correction [7]. The present study aimed to summarize the advantages and disadvantages of expandable and non-expandable cages (TMC) based on data retrieved from current studies, so that a neurosurgeon can tailor each case and select which cage he prefers. Outcomes including deformity correction and implant fusion, subsidence, displacement, and reoperation rates are compared between the two cage types.
Materials and Methods
The present systematic review was done in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [9]. The studies were selected according to the following inclusion criteria: (1) articles including patients with cervical spondylotic myelopathy, aged ≥18 years with expandable or non-expandable (mesh cage only) cages, or comparison of both cages following cervical corpectomy and anterior fixation; (2) articles including any of the radiological outcomes—deformity (segmental angle [SA]) correction, fusion rate, and subsidence rate, or complications—displacement and reoperation rates; and (3) articles published between 2011 and 2021 and in English language only. The exclusion criteria were (1) studies in which all patients underwent cervical corpectomy due to trauma, tumor, or infection; (2) studies that included posterior fixation cases; (3) articles including peek cages (modular cages) as cervical implant; (4) case reports with <5 cases; and (5) systematic review and opinion papers.
1. Search strategy
Studies were searched in various electronic databases (MEDLINE/PubMed, EMBASE, CINAHL, Scopus, and Cochrane database). The following search strategy was performed: (clinical outcome OR radiography OR subsidence rate OR fusion rate OR SA) AND ((expandable cage OR Prostheses and Implants) OR (non-expandable cage OR mesh cage)) AND (cervical corpectomy OR cervical vertebrae). These terms were searched in the article’s entire text. The reference lists of all original and review articles were examined in search of other relevant articles. The abstracts were screened by two independent authors to identify articles that could potentially meet the inclusion criteria. Any discrepancies were resolved after consulting with a third author.
2. Data collection and analysis
The whole text of the articles was read and reviewed by two independent authors to include articles meeting the eligibility criteria. If any published data were insufficient for evaluation, the authors were contacted and requested to provide additional data. After identifying all eligible articles, they were reviewed using a systematic review process. An integrated table including information on the study design, sample size, average age, indications, corpectomy level, cage type used, follow-up period, outcome measures, and results was constructed. A meta-analysis was conducted for the following five outcomes: change in SA, subsidence rate, fusion rate, displacement rate, and reoperation rate. Baseline variables, including age, sex, and follow-up duration, was compared between the expandable and non-expandable cage groups for each outcome. For these outcome variables, age and sex were not statistically significant between the two groups, indicating that these two variables were similar at baseline. Whereas, the non-expandable cage group had a significantly longer follow-up duration than the expandable cage group (p<0.05) (Table 1). Categorical values for each outcome were reported as proportions and continuous data as mean difference. Higgins I2 represented the heterogeneity within the studies. DerSimonian–Laird random-effects model was used when heterogeneity was present, otherwise a fixed-effects model was used. For continuous variables, a fixed-effect model was used due to statistical code limitation, despite heterogeneity; p-value <0.05 was considered significant.

Baseline comparison between expandable and non-expandable cage groups
3. Assessment of risk of bias and level of evidence
Two authors independently assessed the risk of bias using the National Institutes of Health quality assessment tool for evaluating study quality, which was based on a set of questionnaire. Authors could select “yes,” “no,” or “cannot determine/not reported/not applicable” in response to each question. Authors judged each study to be of “good,” “fair,” or “poor” quality [10]. In case of disparities, a concord was drawn up after discussing with an independent third author. Table 2 provides the quality scores of each study, appraising the risk of bias [1–5,7,11–30]. Nine, 14, and three studies were of good, fair, poor quality, respectively. Overall, the risk of bias is low.

National Institutes of Health quality assessment of studies
Results
The PRISMA flowchart shown in Fig. 1 gives an overview of the article selection process. After the initial search, 1,476 studies were identified. Eleven additional studies were identified after searching their reference list and from other sources. After removing 30 duplicate articles, 1,457 remained for title and abstract screening. Studies not meeting the eligibility criteria were excluded from the full-text review, i.e., review articles, editorials, articles with insufficient details and without an English translation. Altogether, 71 full-text articles were reviewed for eligibility; of these, only 26 were eligible articles from which further data were retrieved and the results summarized.
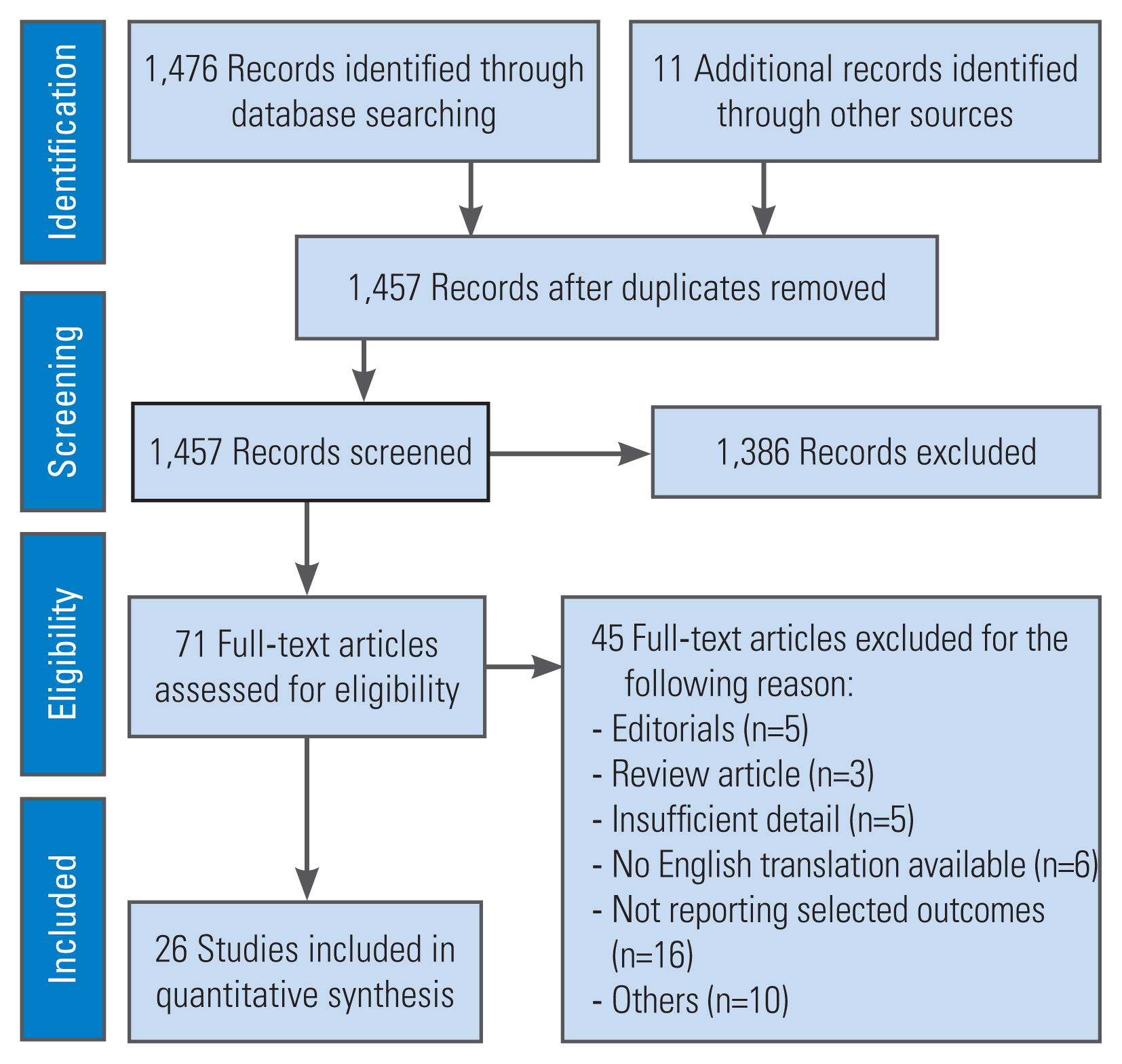
The flowchart of literature search and selection.
1. Study characteristics
Altogether, 21 retrospective and five prospective studies assessed the postoperative outcomes with a follow-up duration ranging from 6 to 96 months. Only two studies had both expandable and non-expandable cage groups for comparison. The remaining 10 studies only had an expandable cage group and 14 studies only had a non-expandable cage (mesh cage) group without any comparison group. The indication for cervical corpectomy in all studies was cervical spondylotic myelopathy. The anterior approach was used without posterior fixation. Traditional mesh and expandable cages were used with an anterior plating system. An autologous bone graft was filled in all cases. Conventional X-rays were used in all studies to assess the radiological outcome and the criteria used to define the radiological outcomes were uniform. The regional angulation (Cobb’s angle) was measured as an angle between the cranial endplate above and the caudal endplate below the affected segment. Fusion was considered to be achieved by the absence of lucency at the cage endcaps and vertebral endplates, or the absence of instability on dynamic X-rays. Subsidence was defined as cage intrusion (>2 mm) into the adjacent vertebral endplates, as seen on radiographs. A summary of studies is presented in Table 3 [1–5,7,11–30].

Summary of studies
2. Change in segmental angle
Altogether, six studies including 199 patients used expandable cages and the other seven studies with 287 patients used non-expandable cages (mesh cage) as the implant device for reconstruction following cervical corpectomy. In the expandable cage group, 141 single-level, 52 two-level, and 6 three-level corpectomies were performed. In the non-expandable cage group, 274 single-level and 13 two-level corpectomies were conducted. The mean age of patients with an expandable cage was 60 years, and they were followed up to a mean duration of 19 months. Whereas, in the non-expandable cage group, these were 62.9 years and 38 months, respectively. The mean change in SA during the last follow-up visit following expandable cage placement was 6.7°, which was significantly greater than that of non-expandable cage placement (3.0°) (p<0.001) (Fig. 2).
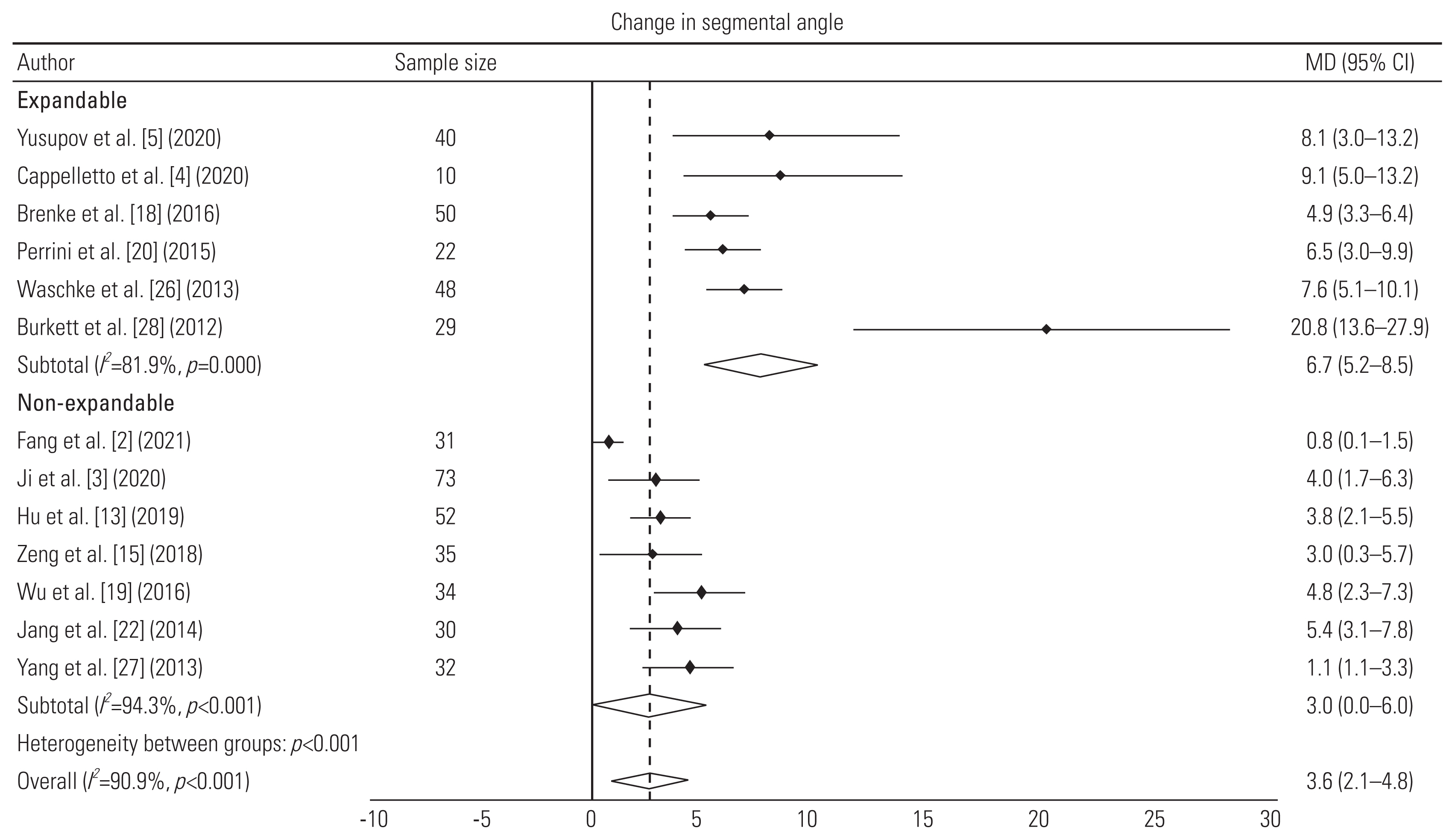
Forest plot showing the comparison of change in segmental angle between the expandable and non-expandable cage groups. MD, mean difference; CI, confidence interval.
3. Subsidence rate
Seven (223 patients) and 13 (652 patients) studies used expandable and non-expandable cages following cervical corpectomy. Altogether, 154 single-level, 54 two-level and 9 three-level corpectomies were performed in the expandable cage group. In the non-expandable cage group, 650 single-level and 49 two-level corpectomies were done. In the expandable cage group, the patients’ mean age and follow-up duration were 60.9 years and 22 months, respectively. In the non-expandable cage group, these were 62.4 years and 39 months, respectively. The mean subsidence rate in expandable cage group was 6%, which was significantly lower than that of the non-expandable cage group at 41% (p<0.001) (Fig. 3).

Forest plot showing the comparison of cage subsidence between the expandable and non-expandable cage groups. ES, estimate; CI, confidence interval.
4. Fusion rate
In the expandable cage group, six studies had a total of 161 patients and, in non-expandable cage group, 13 studies had a total of 532 patients. Altogether, 92 single-level, 37 two-level, and 6 three-level corpectomies were performed in the expandable cage group, whereas, in the non-expandable cage group, 447 single-level and 46 two-level corpectomies were performed. In the expandable cage group, the patients’ mean age and follow-up duration were 58.9 years and 18 months, respectively. In the non-expandable cage group, these were 62.3 years and 32 months, respectively. The mean implant fusion rate at the last follow-up visit in the expandable cage group was 93%, which was lower than that of the non-expandable cage group (98%), but the difference was not statistically significant (p=0.06) (Fig. 4).
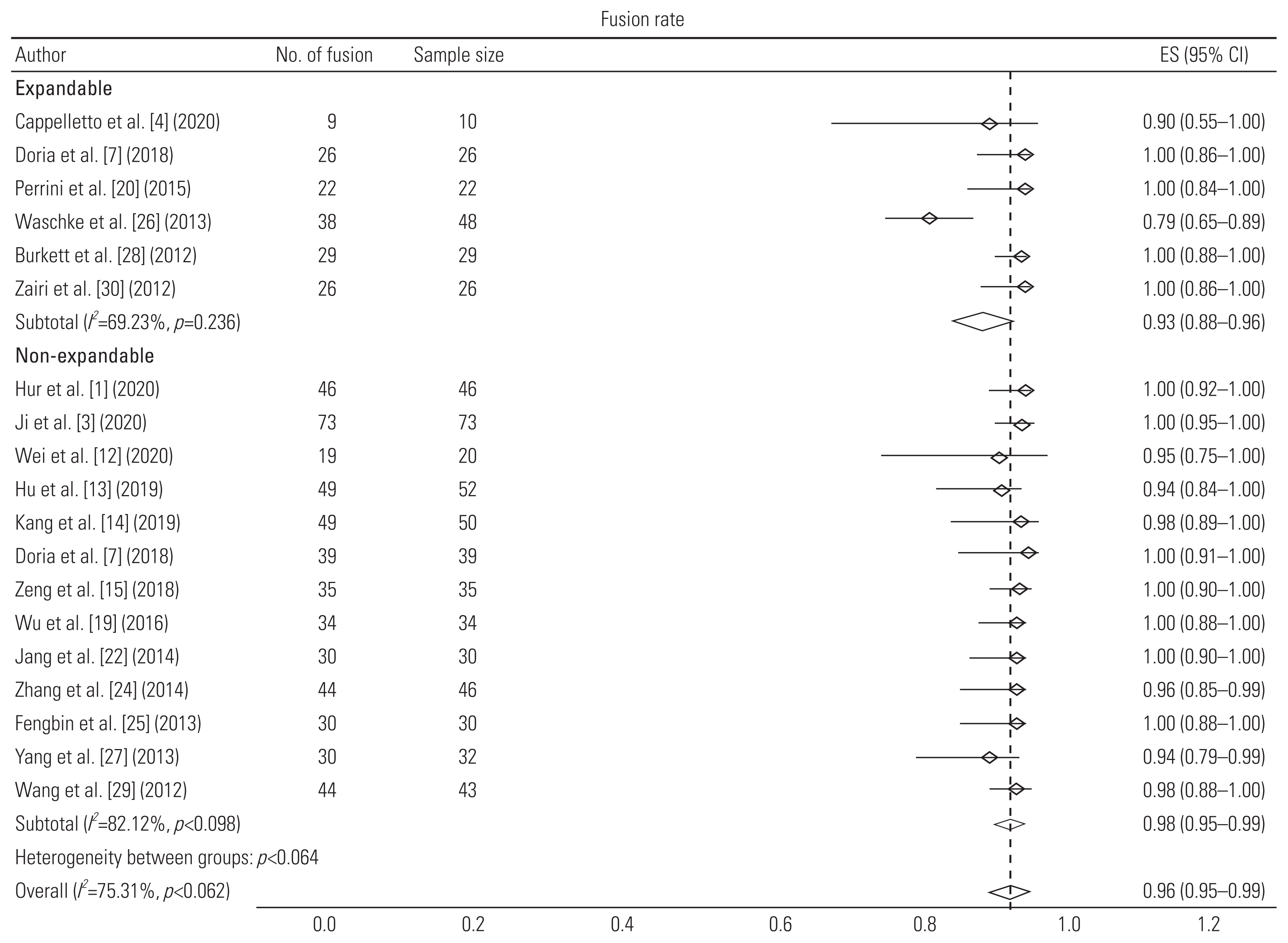
Forest plot showing the comparison of fusion rate of cages between the expandable and non-expandable cage groups. ES, estimate; CI, confidence interval.
5. Displacement rate
Seven studies with an expandable cage group had a total of 279 patients, whereas eight studies with a non-expandable cage group had a total of 308 patients. In the expandable cage group, 136 single-level, 83 two-level, and 14 three-level corpectomies were performed, whereas in the non-expandable cage group, 283 single-level and 25 two-level corpectomies were done. The expandable cage group was older than the non-expandable cage group (57.2 years with mean follow-up duration of 18 months versus 60.1 years with mean follow-up duration of 29 months, respectively). The mean displacement rate at the last follow-up visit of the expandable cage group was 29%, which was significantly higher than that of the non-expandable cage group (5%) (p<0.05) (Fig. 5).
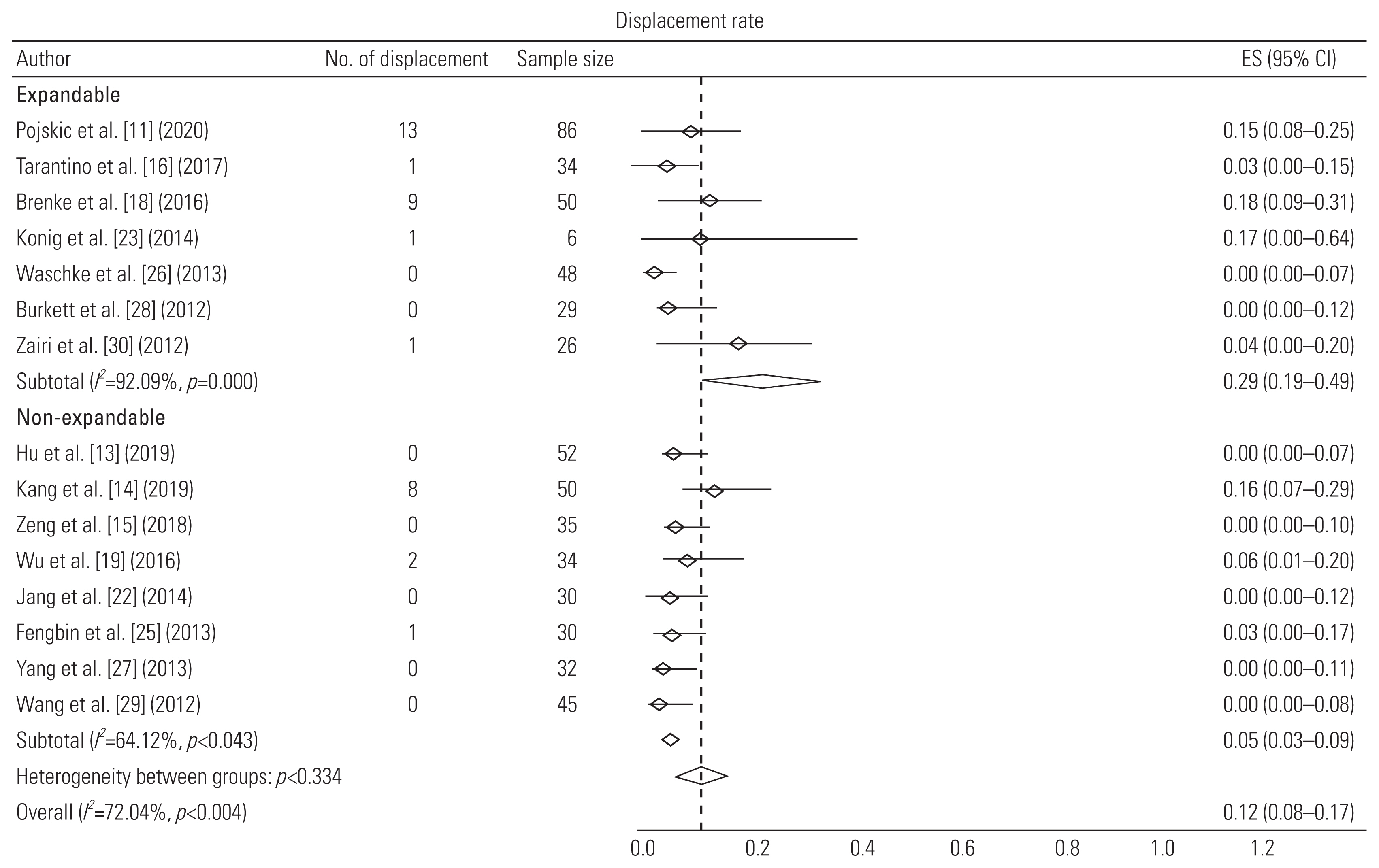
Forest plot showing the comparison of displacement rate of cages between the expandable and non-expandable cage groups. ES, estimate; CI, confidence interval.
6. Reoperation rate
Altogether, 367 patients were present in 11 studies examining expandable cages and 517 patients were present in nine studies using non-expandable cages. In the expandable cage group, 206, 172, and 15 patients underwent single-, two-, and three-level corpectomies, respectively. In the non-expandable cage group, 468 and 49 patients underwent single-level and two-level corpectomies, respectively. The expandable cage group had a mean age of 59.5 years with a mean follow-up duration of 21 months. In the non-expandable cage group, these were 60.9 years and 36 months, respectively. The mean reoperation rate at the last follow-up was higher in the expandable cage group was than in the non-expandable cage group (16% versus 2%), but the difference was not statistically significant (p>0.05) (Fig. 6).
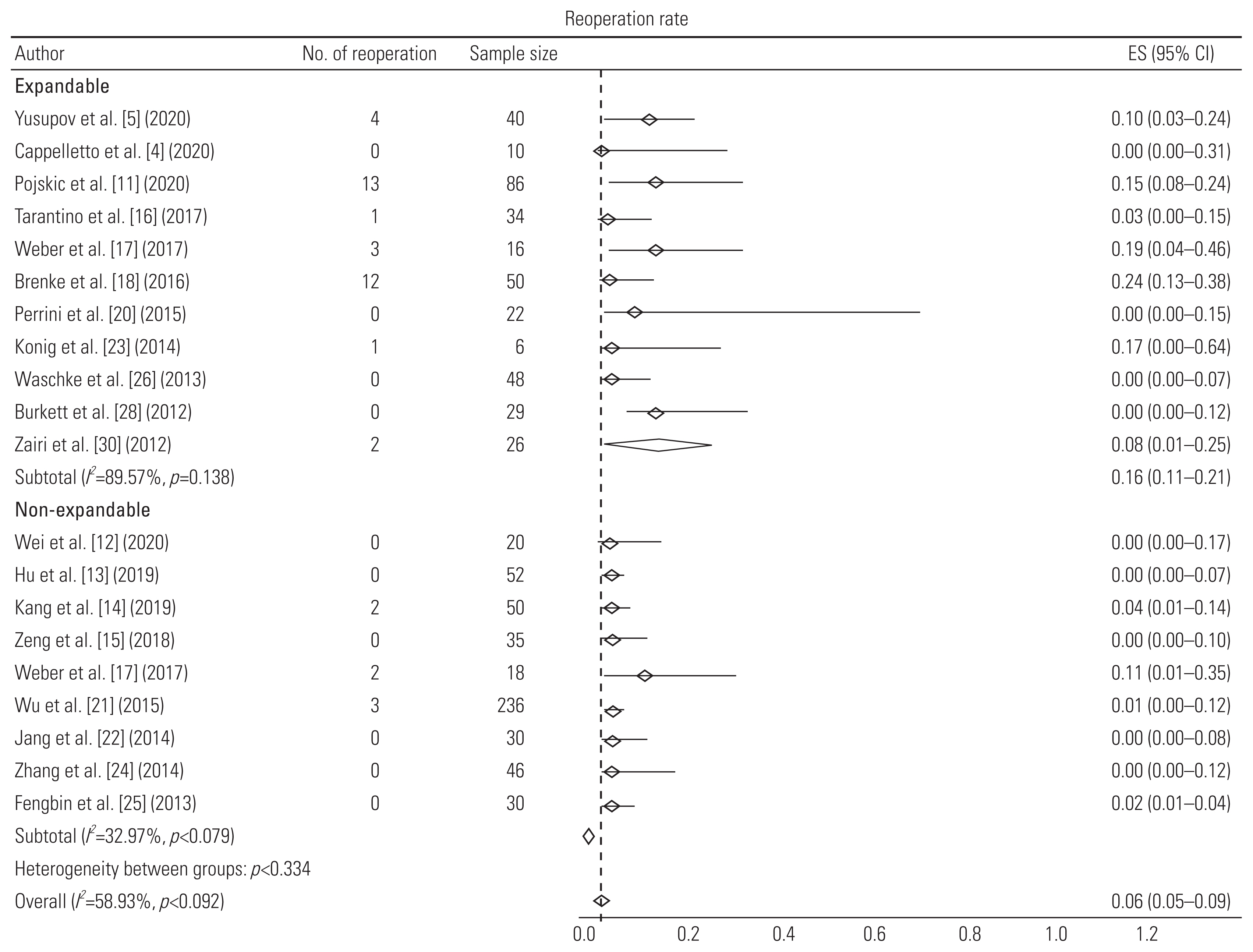
Forest plot showing the comparison of reoperation rate between the expandable and non-expandable cage groups. ES, estimate; CI, confidence interval.
Discussion
Various grafts are available for vertebral body reconstruction after cervical corpectomy (bone autograft, TMCs, and expandable, modular, and polymethylmethacrylate cages). Each graft is distinguished by its own properties conferred by biomechanics and interaction with vertebral endplate surface. Hence, the choice of an appropriate cage is of critical consideration [7]. In this article, we present current evidence on the outcomes of expandable and non-expandable cages following cervical corpectomy.
1. Segmental angle
The change in SA was calculated as a difference between the SA prior to surgery and that post-surgery at the last follow-up visit. In this study, the mean change in SA at the last follow-up visit following expandable cage placement was significantly greater than that of the non-expandable cage (6.7° versus 3.0°, p<0.01). This greater mean difference suggests that the expandable cage is better than the non-expandable cage in deformity correction and cervical lordosis correction. Failure in restoring cervical lordosis can lead to an uneven distribution of axial load over the adjacent vertebral endplates and strain over the neck paraspinal muscles. Expandable cages reportedly improve cervical lordosis but no large comparative studies have been conducted yet to evaluate this [7]. Additionally, expandable cage placement is very smooth and avoids any major damage to the vertebral endplates, in contrast to TMC placement it allows cage expansion in situ and ensues an optimal fit into the corpectomy defect, leading to the correction of kyphosis and restoration of vertebral height and sagittal alignment in single stage. They have wide footprints, which disseminates axial load evenly [7,31].
2. Subsidence rate: complication or a protective phenomenon?
It is an instinctive thought that subsidence should be lower in the cervical spine because of less axial loading, contrary to the dorsal and lumbar spine. Whereas, biomechanical studies have reported that the cervical spine is in fact more susceptible to subsidence than any other region. Subsidence depends on the following several factors: (1) surgical preparation of the vertebral bodies, (2) bone density, (3) modulus of elasticity of the material in the implant (the closer the modulus to the bone, the lesser the probability of subsidence), (4) footprint type and implant diameter (there is a lower chance of subsidence when the contact area is greater), and (5) proportion of distraction on the adjacent vertebrae [28]. In this study, the mean subsidence rate was significantly lower in the expandable cage group (6% versus 41%, p<0.01). Moreover, the expandable cage group had mild degree of subsidence of 2–3 mm, whereas, in the non-expandable cage group, almost all patients had severe subsidence of ≥3 mm at the last follow-up visit. Despite the expandable cage group having more older patients (60.9 years versus 62.4 years, respectively), they seemed to have a lesser number and degree of subsidence. As opposed to TMC, subsidence occurs minimally with expandable cage because of its greater diameter and dull-edged footplates. Hence, using an implant with the largest diameter possible is preferred. Additionally, the endplates’ integrity may further prevent the risk of future subsidence of the cage [31,32]. One study demonstrated that the ratio of footplate-to-vertebral endplate diameter of <0.5 significantly leads to a higher subsidence. Therefore, they recommended that an implant with a footplate with a diameter of more than half of the maximum diameter of the adjacent vertebral endplate should be implanted [32]. The need for cage removal due to intra-operative misalignment, which is more frequent in TMC, usually follows with severe damage to the vertebral endplate integrity [7]. Furthermore, the sharp footprints of TMC weaken the adjacent vertebral endplate and, if the bone density is poor, it will lead to severe subsidence. The subsidence in TMC was reportedly greater on the posterior part than on the anterior part of the implant, which could be due to several elements. The TMC is usually placed in the vertebral body’s anterior part after corpectomy. The cage’s anterior rim contacts the strong cortical surface, whereas its posterior rim fits into the weaker cancellous portion of the vertebral body, which is already damaged by extensive drilling of the surface.
Due to inherent cervical lordosis, the center of gravity is over the cage’s posterior part, causing more pressure on the posterior rim of the cage. Thus, a “tension band effect” is created and majority of the axial load is transmitted from the anterior part of the cage to the posterior part due to the fixed plate with a relatively mobile posterior part. This evolves into a “piston-type action” that increases the risk of subsidence at the posterior rim of TMC [22,25].
Since subsidence is most evident at the posterior rim of the TMC, it may assist in maintaining the cervical lordosis. Despite the fact that there was an increased subsidence, both the SA and cervical sagittal angle (CSA) improved postoperatively and at the last follow-up. These results propounded a theory that posterior subsidence may actually have a favorable effect on maintaining cervical alignment [22]. Previous studies suggested that subsidence can cause a decrease in restored intervertebral height and recompression of the nerve root or spinal cord, leading to poor clinical outcomes. However, the reported incidence of TMC subsidence usually did not lead to a detrimental impact on successful fusion and clinical outcomes postoperatively [3,33,34]. Contrarily, our study found that the visual analog scale and Japanese Orthopaedic Association scale scores improved immediately postoperatively and in the long-term follow-up, despite the TMC group having significant subsidence. Furthermore, the subsidence may encourage fusion by developing a greater surface contact between the cage and vertebral endplate. Thus, despite the fact that subsidence occurred in majority of patients with TMC, fusion was achieved [22].
3. Fusion rate
In this review, the mean fusion rate in the expandable cage group was 93%, which was lower than that of the non-expandable cage group (98%) at the last follow-up visits, although the difference was not statistically significant (p=0.06). The mean age of patients in the expandable and non-expandable cage groups were almost comparable (58.9 years versus 62.3 years). The lower mean fusion rate in the expandable cage group could be due to the difference in the follow-up period (18 months versus 32 months). As discussed above, even with high subsidence in the TMC group, the fusion rate was much higher compared to that of the expandable cage group. The lower fusion rate of the expandable cages can be explained by their restricted surface area for fusion provided by the large footprint and smaller quantity of bone graft that can be inserted in its tiny cavity [3]. The other factor could be that, after distracting these cages, bone filled in its cavity gets spilled out and resorbed, thereby not fulfilling its purpose. Thus, the use of β-tricalcium phosphate reportedly promotes bone ingrowth to attain cage fusion [35].
4. Displacement rate
Graft displacement is among the most dreaded complications of multilevel cervical corpectomy. The displacement risk is proportional to the corpectomy level. The graft displacement is low with one-level corpectomy and, up to some extent, with two-level corpectomy with or without plating. Whereas, graft displacement risk is significantly higher in ≥3 level corpectomy. Theoretically, the rate of graft displacement may be decreased by placing a plate over the graft [36]. Plate fixation increases graft stability by reducing the range of motion and decreases the probability of pseudo-arthrosis [6]. In the present review, the mean displacement rate at the last follow-up visit in expandable cage was 29%, which was significantly higher than that of non-expandable cage fixation (5%) (p<0.05). One important factor for this result could be the corpectomy level. In the expandable cage group, 42.5% of patients underwent implant placement after multilevel corpectomy, including two and three levels; this rate was higher than that of the non-expandable cage group (14.5%) and that’s too only two-level corpectomy. This could be the possible major factor predicting the large number of displacement in the expandable cage group because in both groups all patients had anterior plating. In one recent study, expandable cages were not considered ideal implants for multilevel corpectomy. One feasible reason mentioned was the limited cage and bone interface when the expandable cage is placed over long segments [23]. The insertion of expandable cage requires a precise adjustment of the implant height in situ according to the size of corpectomy with a firm contact between footplates and vertebral endplates to prevent cage migration. To achieve this firm and secure fit into the defect, some over-distraction is required. Thus, inadequate distraction in view of the misjudgment of the cage height can result in weak compressive forces over endplates and may lead to cage migration [6]. Contrary to the dull edges of footprints of the expandable cage, the sharp footprints of TMC usually subside into the vertebral endplate during fixation providing a firmer placement than expandable cages.
5. Reoperation rate
In this review, the mean reoperation rate in the expandable cage group was 16%, which was higher than that of the non-expandable cage group (2%) at the last follow-up visit. However, the difference was not statistically significant (p>0.05). The mean ages of the expandable and non-expandable cage groups were 59.5 and 60.9 years, respectively. In both groups, implant-related factors (displacement and malalignment) were the major causes of revision surgeries. Other less common causes were epidural hematoma, pseudoarthrosis, infection, and delayed union. One of the subsidence prevention features of expandable cage is the limited footprint surface area, which leads to less fusion due to the inadequate graft–host bone contact and in turn increases the implant failure risk [37]. Noteworthy, despite the long mean follow-up period in the non-expandable cage group, no patient underwent revision surgery for severe subsidence.
6. Limitations
This systematic review gives a comprehensive insight to the use of expandable and non-expandable cervical implants and their complications. However, this study has a few limitations. First, the follow-up duration was different between the two treatment groups. Secondly, only change in SA was evaluated in this review, as only few of the published studies report the effect on CSA (C2–C7 Cobb’s angle). Lastly, the effect of cages on the adjacent segment disease is not reported in any of these included studies. Therefore, randomized studies with a large sample size, taking into the account the abovementioned factors, and an adequate follow-up period are warranted.
Conclusions
For expandable cages, the degree of improvement in SA is better with less frequent subsidence even in older patients but they have a low fusion rate and high displacement and reoperation rates. Therefore, expandable cages should be used in patients where severe subsidence need to be considered, such as those with vertebral osteomyelitis, cervical vertebrae malignant lesion, and osteoporosis. Additionally, expandable cages are not the optimal choice for multilevel corpectomy. For non-expandable TMCs, the major drawback is its high subsidence rate but it seems to be a protective phenomenon as evidenced by the high fusion rate and minimal effect on clinical outcome. To tackle high subsidence, mesh cages with end caps or cement augmentation need to be considered.
Acknowledgments
We acknowledge all our professors and consultants from the Department of Neurosurgery for the guidance and assistance.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Conceptualization: DKP; data curation: AKD, AG; formal analysis: AKD, RK; funding acquisition: AKD, AG; methodology: DKP; project administration: not applicable; visualization: DKP, RK; writing–original draft: AKD; Writing–review & editing: AKD, DKP, AG, RK; and final approval of the manuscript: all authors.