Introduction
Surgical treatments such as anterior debridement and bone graft, anterior instrumentation, and either single or combined posterior instrumentation1-3 have been introduced as well as other techniques (i.e. percutaneous drainage and irrigation4, percutaneous transpedicular discectomy5 and percutaneous spinal external fixation6. The most effective of the various surgical methods to eradicate infection has not been evaluated. We analyzed patients that underwent anterior debridement and fusion followed by posterior instrumentation.
Materials and Methods
1. Patients
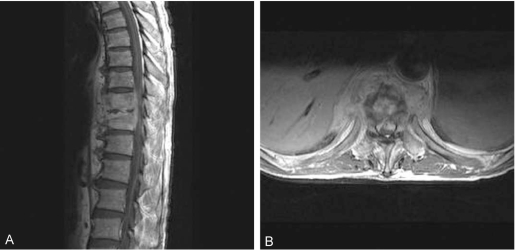
This study included 20 patients with pyogenic spondylitis who underwent anterior debridement and interbody fusion with strut bone graft followed by posterior instrumentation from 1996 to 2005. The mean age of the patients was 59 years (range, 38~80 years) and the mean follow-up period was 25 months (range, 12~42 months). Accompanying diseases were hypertension in four patients, diabetes mellitus in three patients, and other disorders including hyperthyroidism, acute glomerulonephritis, and dementia. Three Lesions were in the thoracic region, 4 legions in the thoracolumbar region and 13 lesions in the lumbosacral region. Neurological deficits were present in 10 cases prior to surgery. The mean time to diagnosis was 5 weeks. The extent of surgery was determined based on diagnosis made by MRI. The indications for surgical debridement included neurological compromise, failed medical treatment, soft tissue extension, extensive vertebral body and disc space destruction, and a progressive deformity1.
2. Methods
A retrospective analysis of the patient medical records and imaging studies were performed along with a telephone survey. The clinical results and the neurological changes were assessed according to the McNab classification (Table 1) and ASIA impairment scale, respectively. The degree of bony union was investigated using the Lenke classification (Table 2). Cobb's method was used for measuring changes in the kyphotic angle when imaging studies showed complete bony union. The duration for normalization of the hematological parameters, i.e. the white blood cell (WBC) count, the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level, were recorded. Culture studies for microorganisms were performed after surgery. The metal failure or screw loosening, and other neurological injuries were also analyzed.
3. Surgical technique and postoperative care
To decide the level of posterior instrumentation preoperatively, if a large part of the vertebral bodies were involved with signal changes as seen on MRI, then instrumentation was performed that extended to one level above and below the involved vertebrae. If only a part of a vertebrae showed signal changes, and pedicle fixation was feasible, then instrumentation was performed on the most proximal and distal affected segments. For the level of anterior fusion, a strut bone graft was performed followed by a corpectomy on all vertebral bodies that showed signal changes on MRI preoperatively. If the lesion was in only one vertebra, a strut bone graft was performed toward just above or below the end plate of the more destructed part.
We performed the procedure under general anesthesia with the patient in the prone position. We dissected subperiostealy using Cobb's elevator down the spinous process and along the laminar to the facet joint. Using an image intensifier, pedicle screws were inserted to both sides of the pedicles at the lesion by use of the intersection technique. Then a rod was inserted to the pedicle screws.
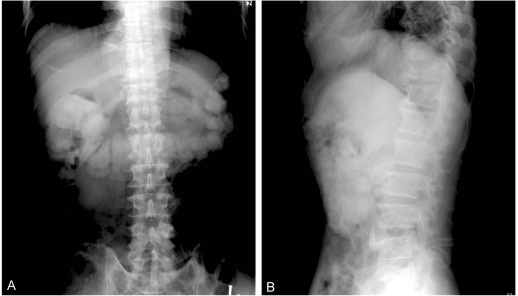
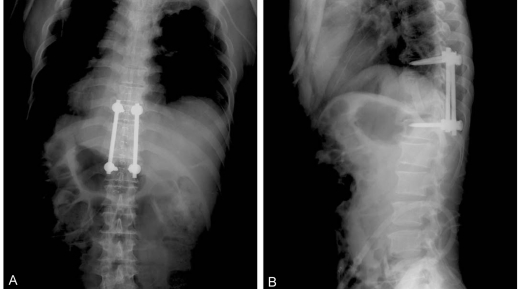
Next, the patient was placed in the semi-lateral position with the right side exposed. The infected lesion was approached with a transthoracic or retroperitoneal approach. Curettage and debridement was performed with a corpectomy. A strut bone graft was performed from the rib or iliac crest. The iliac crest donor site was reconstructed by use of a 1/3 tubular plate7. There was one case where a mesh was inserted. The drain was removed when the amount was below 50 cc. Ambulation was started at the next day with the use of a brace (Figs. 1-3). For two cases out of the total 20 cases, hardware was removed at 2 years postoperatively.
Results
1. Clinical result (Table 3)
For clinical symptom relief, seven patients were grouped as 'excellent,' twelve patients 'good,' and one patient as 'fair.' Half of the 10 patients that had a neurological deficit prior to surgery were improved in motor and sensory function after surgery. With regards to the time to diagnosis, logistic regression analysis showed a significant difference (p=0.05) between patients with or without positive improvement.
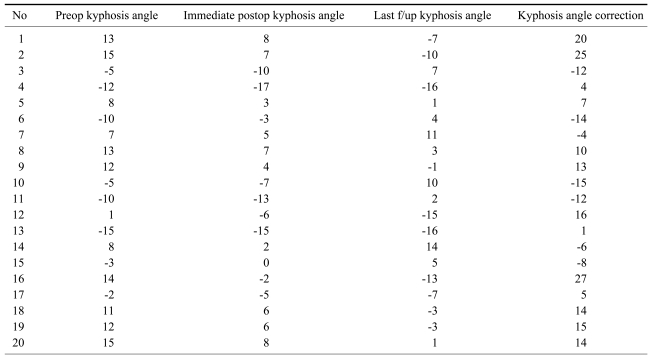
2. Imaging studies (Table 4)
To obtain complete bony unions as seen on the plain radiographs, an average of 4 months was required. Fifteen cases of grade 1 and 5 cases of grade 2 were identified by Lenke's classification. The kyphotic angle was measured for all but one case involving the upper thoracic vertebrae. The average correction angle was 5 degrees after surgery.
3. Laboratory results
Before surgery, WBC counts in 9 patients were 10000/┬ĄL or more and the average was 9700/┬ĄL. All patients showed normalization of the WBC counts within 4 months after surgery. For the ESR, with a normal range of 0~10 mm/hr in men and 0~20 mm/hr in women, became normalized in 9 patients after 3 months on average. The other 11 patients showed a decrease in the ESR from 65.8 mm/hr preoperatively to 44.2 mm/hr postoperatively on average. The preoperatively checked CRP level was 6.0 mg/dL on average. The average duration for the CRP level to become normalized was 1.9 months. In two patients, the CRP level remained above 10 mg/dL (11.4 and 8.5 mg/dL, respectively). In 14 cases, culture studies showed the presence of S. aureus in half of the cases and coagulase (-) staphylococci in the other half of the cases.
4. Other complications
There was one case of incomplete bony union, which was later corrected by a subsequent revision operation. A complete bony union was finally achieved, as seen on follow-up X-rays. Two cases of sensory disturbance in the femoral area were reported but the patients complained of minimum interference in daily activities.
Discussion
In 1911, Albee8 proposed posterior instrumentation with auto transplantation of the tibia for treatment of tuberculous spondylitis, which marked progression of surgical treatment9. Since Hodgson and Stock10 proposed anterior fusion (instrumentation) with anterior debridement and auto transplantation in 1960, its use has gained wide popularity although posterior instrumentation was added to the procedure for fast rehabilitation. Wang11 has stated that physiologically the anterior and middle spinal column could bear 70~80% of the axial gravitational pressure and the posterior column could bear the remaining 20~30%. On that basis, Wang advocated the use of the anterior fusion method with an anterior approach, arguing that present day posterior instrumentation alone without anterior instrumentation could not bear a pressure of 1,300 N, physiologically exerted to the anterior column.
Also suggested was a method of posterior approach where laminectomy and resection of granulation tissue protruded into epidural space are performed and then are supplemented by posterior fusion with preceding bone transplantation on the co-resected disc area12. However, this method is useful with only one body infection; in our study this situation was found in only two cases among the 20 patients. We think this method is a somewhat limited technique.
One of the new minimally invasive surgical treatments is percutaneous transpedicular discectomy. This method allows both definitive diagnosis and treatment at the same time and could be used for cases in the early stage where there is no instability, bone destruction or other neurological symptoms5.
Another method is percutaneous drainage and irrigation4, which was suggested by Hanaoka and colleagues. This is reserved as a second line treatment for patients with a poor general condition, evidence of an abscess on MRI, and advanced bone destruction.
Some surgeons perform posterior instrumentation 1~2 weeks after anterior fusion. In contrast, we performed anterior debridement and fusion immediately followed by posterior spinal instrumentation13.
Sensory disturbance in one patient, who was reported as 'fair' according to McNab's classification for the clinical result, was found in the femoral area where the bone graft was harvested, implying no correlation with symptoms of pyogenic spondyiltis. One other patient who reported such a sensory disturbance complained only of minimal interruption in daily life during the one-year postoperative period. A preoperative neurological deficit could not be assessed in two patients due to dementia in both cases but could be found in 10 other patients. Of these 10 cases, half of the patients showed improvement postoperatively. As reported in the result, there was significant correlation the time until diagnosis with neurological improvement. For this reason, we believe that early decompression is important. For blood chemistry, the ESR and CRP level decreased significantly within 3.3 and 1.9 months respectively. Two patients showed persistently high CRP levels postoperatively but the high levels could be attributed to the fact that one patient developed a bed sore after admission to the hospital and the other patient developed cellulitis in the right foot. A culture for microorganisms is known to yield positive results in 60~80% of cases in general14, which was confirmed in this study, yielding 14 positive results (7 cases of S. aureus infection and 7 cases of coagulase (-) staphylococci infection) out of 20 cases. S. govender said that the frequent organism is S. aureus, Streptococcus, and coagulase (-) staphylococci are assumed to cause subclinical infections that probably account for a low ESR and a decreased CRP level15.