Introduction
Scheuermann's kyphosis (SK) is a thoracic hyperkyphosis first described by Holger Werfel Scheuermann in 1921 [1]. Radiographically, this deformity presents as an anterior wedging of three consecutive vertebrae by more than 5 degrees, with endplate irregularities, loss of disc space, and the presence of Schmorl nodes [2].
According to the literature, operative treatment should be considered for patients with a kyphotic deformity of over 70–75 degrees, significant pain that has not responded to conservative management, and/or respiratory problems due to severe kyphosis [3]. The correction of kyphosis with instrumentation can be performed using posterior-only or combined anterior-posterior procedures [4]. With the use of all-pedicle screw constructs in spine surgery, the posterior-only approach has become a favorable option for the definitive treatment of SK [5]. In a nationwide study involving 2,796 patients, a trend toward posterior-only fusion with lower complication rates was reported [6].
The purpose of this study was to evaluate the clinical and radiological results of the posterior-only approach with pedicle screws in patients with SK.
Materials and Methods
Local ethical committee approval was obtained for this retrospective study. We retrospectively reviewed and analyzed the data of patients who underwent posterior-only correction for SK between January 2005 and May 2013. Patients with a definitive diagnosis of SK and a minimum follow-up of 24 months were included. Indications for surgery were a thoracic kyphosis angle of over 70 degrees with persistent pain despite conservative management and/or cosmetic concerns. Patients with tumors, inflammatory diseases, traumatic spine pathologies, and neurological deficits, as well as those who had spinal surgery, were excluded.
Standing anterior-posterior and lateral radiographs were taken preoperatively, shortly after surgery, and at the last control. Radiographs for all patients were evaluated by the same senior surgeon through our center's radiograph archiving system (PACS INFINITT, INFINITT Healthcare Co., Hangzhou, China). Thoracic kyphosis (T5–T12), lumbar lordosis (LL) (L1–S1), and thoracolumbar junction (T10–L2) angles were measured using the Cobb angle method preoperatively, postoperatively, and at the last control. Sagittal balance (displacement in mm, normally passing the C7 plumb line from the posterior-superior endplate of S1), thoracic length (length in mm, between the anterior-superior endplate of T1 and the anterior-inferior endplate of T12), thoracic diameter (length in mm, between the thoracic apex vertebrae and the thoracic length line), Voutsinas index (ratio of thoracic diameter to thoracic length×100, TD/TL×100), the sacral slope (SS) angle, and the pelvic tilt (PT) angle were also measured preoperatively, postoperatively, and at the last control.
Junctional kyphosis, which can occur in proximal or distal segments, is a common radiographic finding after SK surgery because of the abrupt transition between fixed and mobile spinal segments. The proximal junction kyphosis (PJK) angle (Cobb angle between the caudal endplate of the highest instrumented vertebrae and the cephalic endplate of the vertebrae two rows above) and distal junction kyphosis (DJK) angle (Cobb angle between the cephalic endplate of the lowest instrumented vertebrae and the caudal endplate of the vertebrae two rows below) were measured postoperatively and at the last control. Proximal or distal junctional kyphosis was considered to be present if the PJK or DJK angles were higher than 10 degrees. The Scoliosis Research Society 22 (SRS-22) questionnaire translated to our native language was completed by all patients.
1. Surgical technique
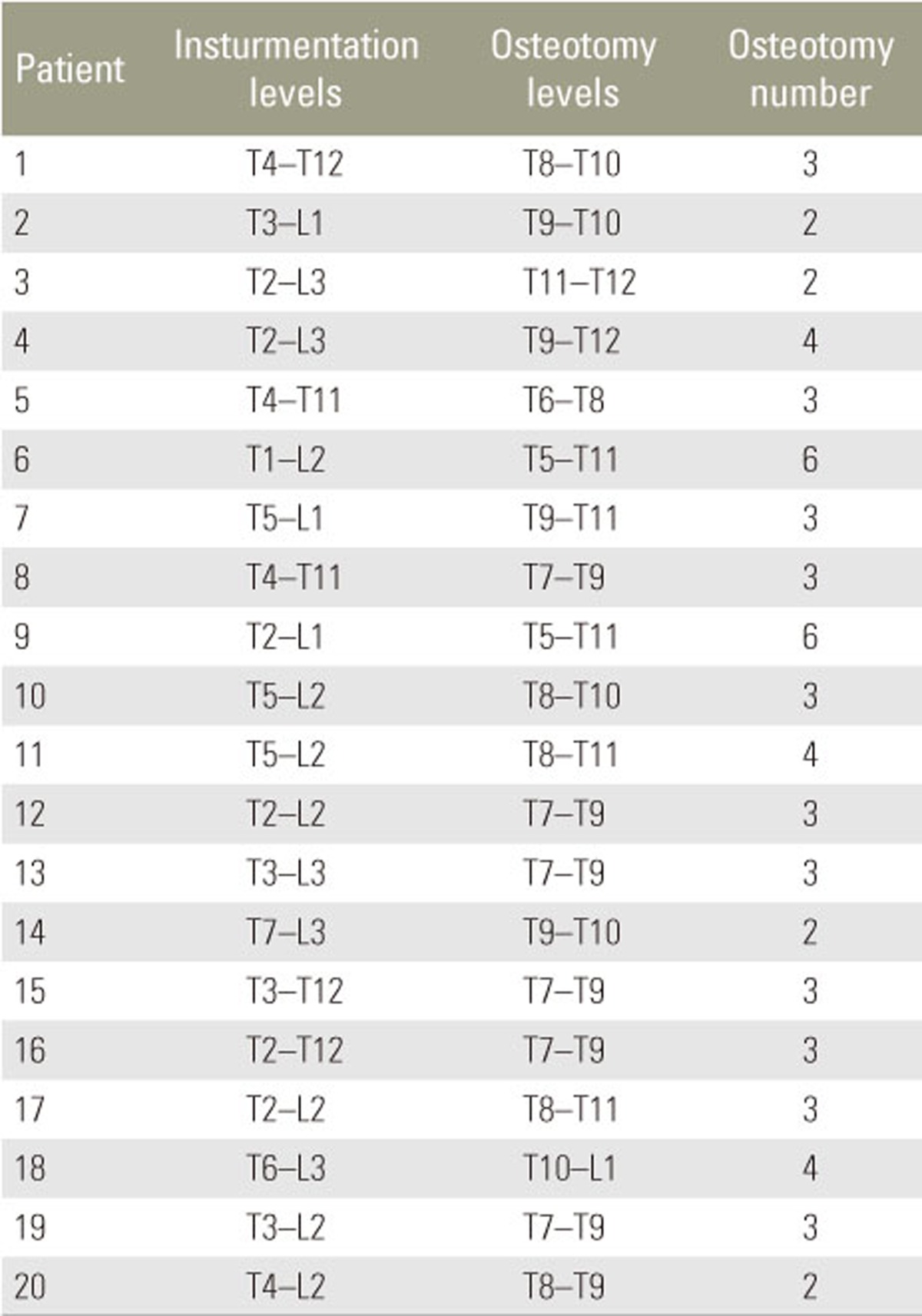
All surgeries were performed by two senior surgeons at our center's spine clinic using the same techniques. Patients were placed prone on the operating table (radiolucent table) under general anesthesia. A standard posterior midline incision was used, and paraspinal muscles were subperiosteally elevated to the tips of the transverse processes. Monoaxial titanium pedicle screws were bilaterally used for all levels and were placed using the free-hand technique. Proximal fusion was performed at the first kyphotic vertebrae to prevent PJK, and fusion was performed toward the first lordotic vertebrae distally. Apical Ponte osteotomies were routinely performed in all patients to enable deformity correction. Two 6.0 mm titanium rods were used for deformity correction after the above procedures, and the nuts were tightened. Allografts were used for nine patients, and posterior elements were decorticated and used as autologous grafts along the fusion levels for all patients.
On the first postoperative day, patients were ambulated under the guidance of an orthopedic surgeon. Patients were discharged with instructions to limit compelling activities and were contacted for follow-ups at the 2nd, 4th, 8th, 12th, and 24th weeks after surgery and annually afterwards.
2. Statistical analysis
SPSS ver. 17.0 for Windows (IBM, Chicago, IL, USA) was used for statistical analysis. Variance analysis (repeated analysis of variance) and post hoc Bonferroni analysis were performed to evaluate quantitative values such as preoperative, postoperative, and last control measurements. Categorical data were evaluated with Fisher's test, and p-values lower than 0.05 were considered statistically significant.
Results
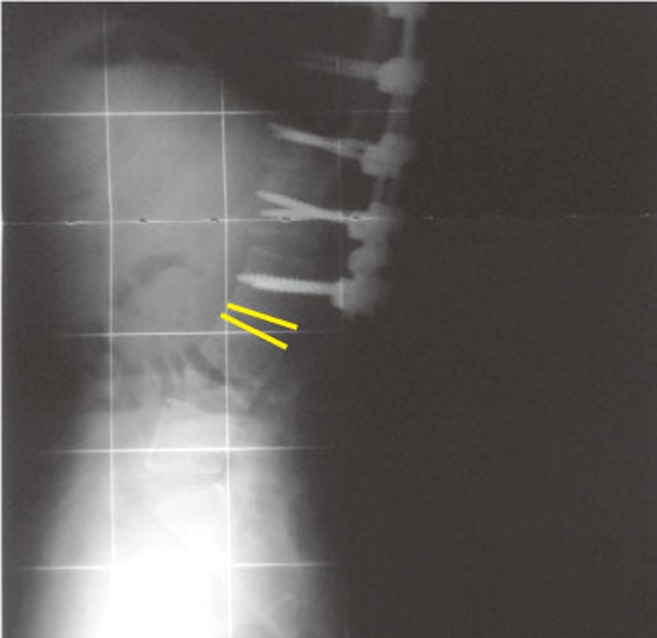
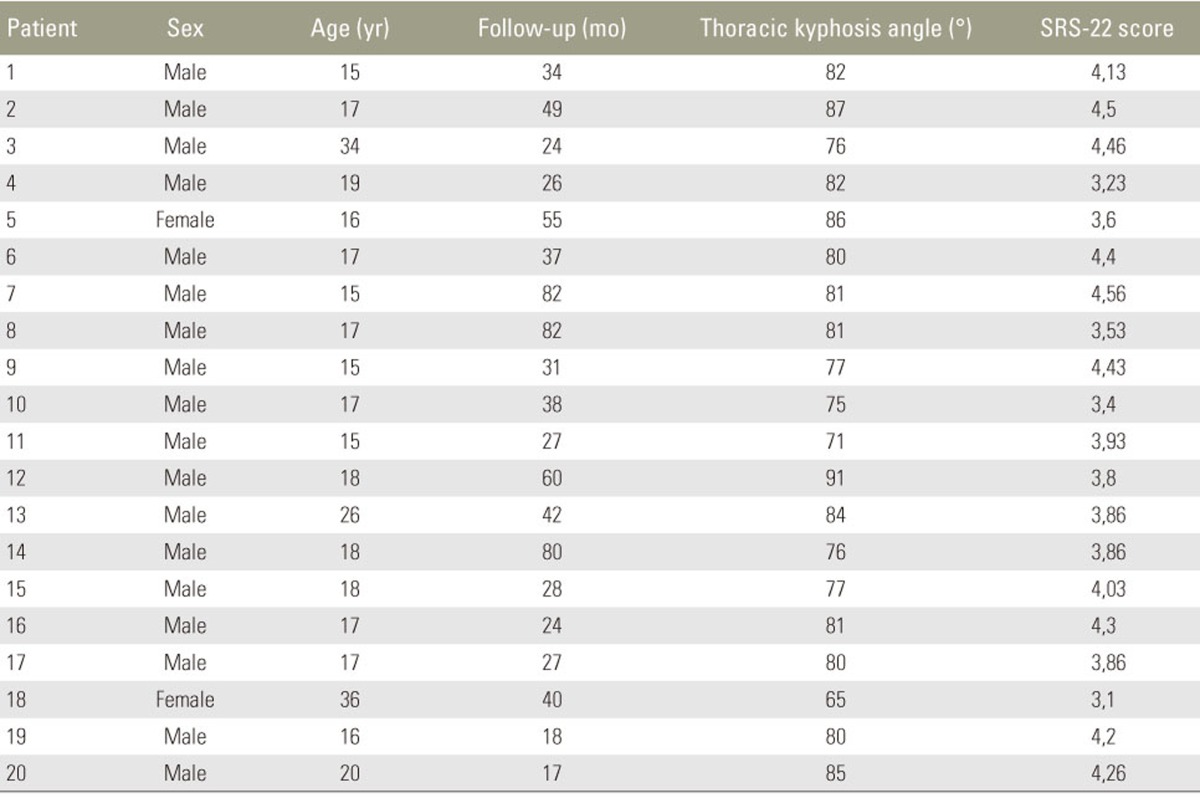
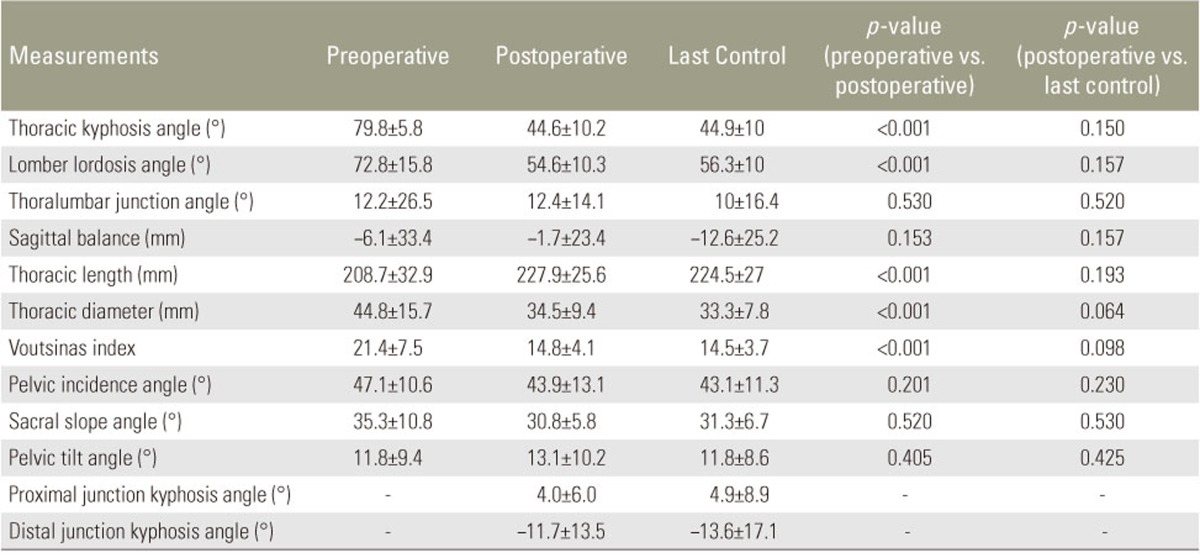
Forty-five patients underwent surgery for the treatment of SK between 2005 and 2013. After applying the exclusion criterion, 20 patients (18 males and 2 females) with a mean age of 19 years (range, 15 to 36 years) were included. Our follow-up rate was 44%, and the mean follow-up length was 41 months (range, 24 to 82 months). The demographic data of the patients are shown in Table 1, and the operative data are shown in Table 2. The mean preoperative thoracic kyphosis angle was 79.8±5.8 degrees (range, 65 to 91 degrees), and the mean postoperative thoracic kyphosis angle was 44.6±10.2 degrees (range, 20 to 58 degrees). The mean last control thoracic kyphosis angle was 44.9±10 degrees (range, 29 to 60 degrees) (Figs. 1, 2). The degree of correction was statistically significant when preoperative values were compared with early postoperative and last control values (p<0.05). There was no statistically significant difference between the early postoperative and last control values (p>0.05). Other values and the p values for preoperative, postoperative, and last control differences are shown in Table 3.
The mean SRS-22 score, which was evaluated from 1 to 5 points (1, worst; 5, best) for each component, was 3.9±0.4 points (range, 3.1 to 4.6 points) (Table 1). The best mean score was obtained from the “self-image” component and the worst was obtained from the “mental health” component. The most remarkable result from the questionnaire was that almost all patients answered “definitely yes” to the question “Would you have the same management again if you had the same condition?”
The following complications occurred: one patient had rod failure two years after surgery and revision surgery was performed, three patients had PJK (15%), and three patients had DJK (15%) (Fig. 3).
Discussion
The posterior-only approach was the first operative technique introduced for the correction of kyphotic deformity in SK and was first performed by Bradford in 1975 [7]. Bradford et al. [8] reported loss of correction in 16 of 22 patients and emphasized that the correction of kyphosis at all lengths contributed to this complication. Different methods have been introduced over the years, and combined anterior-posterior fusion has been recommended for many years for rigid and large deformities. Today, debates continue regarding additional anterior release or posterior-only fusion for the surgical management of SK [4].
In this study, we achieved an average of 35 degrees of correction without loss of correction. Many studies have compared the posterior-only approach with anterior-posterior correction. In these studies, the authors reported similar results for the correction of deformity followed by loss of correction during the follow-up period, with higher complication rates reported for combined anterior-posterior groups [5910]. Consequently, the popularity of posterior-only fusion has increased in recent years. Papagelopoulos et al. [11] reported the results of posterior- only fusion using a segmental compression device in 13 patients. In the study, the thoracic kyphosis angle decreased from 68.5 to 40 degrees and the average loss of correction was 4.4 degrees after 4.5 years of follow-up. Ponte reported the results of posterior-only fusion (with Ponte osteotomies and pedicle screws) in 17 patients. In the study, the best results were achieved with the combined anterior-posterior technique [12]. Behrbalk et al. [13] also achieved satisfactory results in 21 patients in whom posterior-only fusion and Ponte osteotomies were performed. In the present study, we performed Ponte osteotomies for all patients and achieved satisfactory results for up to 91 degrees of thoracic kyphosis without additional anterior release.
In SK, thoracic hyperkyphosis is commonly associated with LL, which is reduced by the surgical correction of hyperkyphosis [14]. The preoperative and postoperative sagittal profiles and spinopelvic parameters of patients with SK have been compared in a few studies. Jansen et al. [15] reported a strong correlation between the correction of kyphosis and spontaneous decrease in the LL after fusion. Jansen also reported a correlation between LL and the SS. In the present study, we achieved a significant decrease in LL after the correction of thoracic kyphosis, and there were no significant changes in the SS, PT, and pelvic incidence (PI=SS+PT) after posterior fusion. In a recent study with 20 patients, sagittal spinopelvic parameters were evaluated after the posterior-only correction of SK and no significant changes were reported in the SS and PT, as well as in the PI as expected [16]. These results can be explained by the irreversible contracture of pelvic ligaments through the years because of kyphotic deformity.
The Voutsinas index is a measure that provides information about the morphology of kyphotic curves based on the Cobb method because the length and width of the curvature are taken into consideration [17]. In a study in which combined anterior-posterior fusion was performed in 15 patients, the authors achieved significant correction in the Voutsinas index, with no significant changes after 4 years of follow-up [18]. In our study, we also achieved significant correction and normalization in the Voutsinas index after posterior-only fusion, with no significant changes at the last control.
In a review, the overall complication rate after posterioronly fusion was reported to be 14.8% and did not significantly differ when compared with that after combined anterior-posterior fusion (16.9%) [19]. PJK and DJK are common well-known complications after SK surgery [20]. The most common risk factor for PJK is inadequate identification of the proximal end vertebrae, and overcorrection of kyphosis is another risk factor [2122]. In our study, 15% of the patients had asymptomatic PJK. The average correction of kyphosis for these patients was 33.4 degrees, and the cause of PJK was mostly likely the selection of the wrong proximal kyphotic vertebrae. Proper selection of the distal fusion level is important to prevent DJK after SK surgery [23]. Yanik et al. [24] reported their results for posterior-only fusion in 54 patients after investigating the occurrence of DJK in relation to the distal fusion level. They concluded that fusion to the first lordotic vertebrae is sufficient for distal fusion.
The main limitation of this study was the small patient population due to the low follow-up rate. The retrospective design of the study was another limitation. Prospective randomized studies with larger populations are needed in the future.