Introduction
Low back pain (LBP) is experienced in 60%–80% of adults at some point in their lifetime. Andersson [1] estimated the annual worldwide LBP incidence in adults to be 15% and the point prevalence to be 30%. Papageorgiou et al. [2] stated that at least 50% of adults would have experienced an LBP episode. Some studies have demonstrated that LBP is one of the most common cause of visits to a physician [3] and that men and women are equally affected by LBP [4]. The literature shows that 30% of adolescents worldwide experience at least one LBP episode [4]. Various studies found that LBP is a very common problem among adolescents, with an incidence that is the highest in the third decade of life [5]. Some authors proposed that LBP in young adults and children may occur because of growth spurts and increased physical activity [6]. In contrast, Fairbank et al. [7] revealed that students with back pain were more likely to be sports avoiders than their counterparts who were involved in sports. Young adults who experienced LBP at the age of 14 years had an increased incidence 25 years later compared with those who did not experience LBP at age 14 years [8]. Therefore, preventing and avoiding LBP during early adolescence can prevent LBP progression, and thus, can decrease the associated morbidities. However, to prevent LBP, the associated modifiable and non-modifiable risk factors must be identified. Previous studies have demonstrated that high body mass index (BMI) is associated with an increased LBP incidence [9]. In addition, Webb et al. [9] revealed that hereditary plays a vital role in LBP occurrence and that a positive family history has a strong correlation with LBP incidence [10]. Risk factors for LBP are not limited to physical factors; psychosocial factors such as stress, anxiety, depression, and monotony are also potential risk factors for LBP [11121314]. These risk factors can result in the progression from an acute LBP episode to a chronic problem.
Although various studies in the literature have examined the incidence, prevalence, and risk factors for LBP in young adults, there is a paucity of data regarding this topic in young Indian adults. Given this gap in the literature, we conducted a cross-sectional study that aimed to evaluate the prevalence of LBP and the various risk factors for LBP in young adult Indians.
Materials and Methods
A cross-sectional study was employed according to the requirements of regulatory authorities and with the permission from the local Institutional Ethics Committee. A total of 1,532 young adults aged between 18 and 35 years were enrolled. The study was conducted among coaching institutes of Indian Administrative Service aspirants and medical postgraduate aspirants in Delhi from August to November 2014. A detailed questionnaire collected data regarding the subjects' sociodemographic profiles assessed using the modified Kuppuswamy scale; smoking (regular smoking was defined as someone who smoked 100 cigarettes in their lifetime and currently smoked cigarettes daily or some days [nondaily]), alcoholism (regular alcoholism was defined as five drinks for men and four drinks for women and must be consumed on one occasion at least once in a 2-week period), and traveling history; diet; time spent studying per day; place of study; posture while studying (walking, sitting in a chair and forward bending, sitting in a chair with back support, sitting on the floor with back support, and sitting on the floor without back support); frequency of weightlifting; sports activities (strenuous activities included swimming laps, aerobics, calisthenics, running, jogging, basketball, cycling on hills, and racquetball and moderate exercises included brisk walking, golf, volleyball, cycling on level streets, recreational tennis, and softball). Frequency and type of sport, history of LBP, factors that aggravate and relieve LBP, frequency of wearing heels, history of osteoporosis, history of spine problems, whether LBP limits daily, strenuous, or social activities, whether LBP is aggravated by the number of study hours, history of emotional depression, presence of monotony, satisfaction in current employment position, family history of spine problems, or spinal surgery. Anthropometric measurements, including height and weight, were measured, and BMI was calculated. Pain was assigned a score of 0–100. After obtaining ethical permission, all subjects were requested to complete the questionnaire in the presence of an investigator. Informed verbal consent was obtained from all study participants. The data were analyzed using the SPSS ver. 12 (SPSS Inc., Chicago, IL, USA). Percentages and proportions were calculated. The chi-square test was used for categorical variables. Logistic regression analysis was performed using the stepwise, forward entry method, and significant risk factors were examined using significance, standard error, 95% confidence intervals, and Wald test.
Results
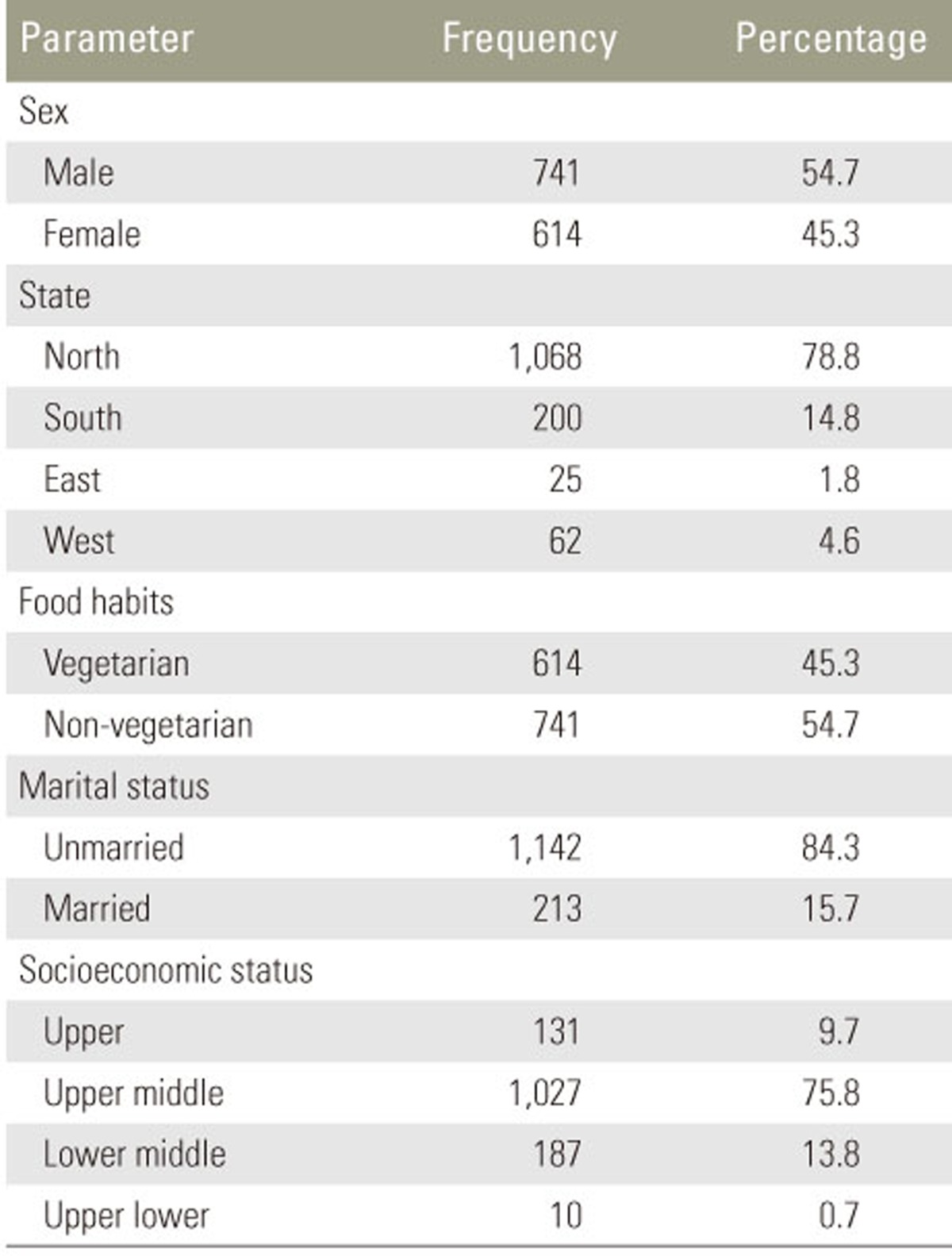
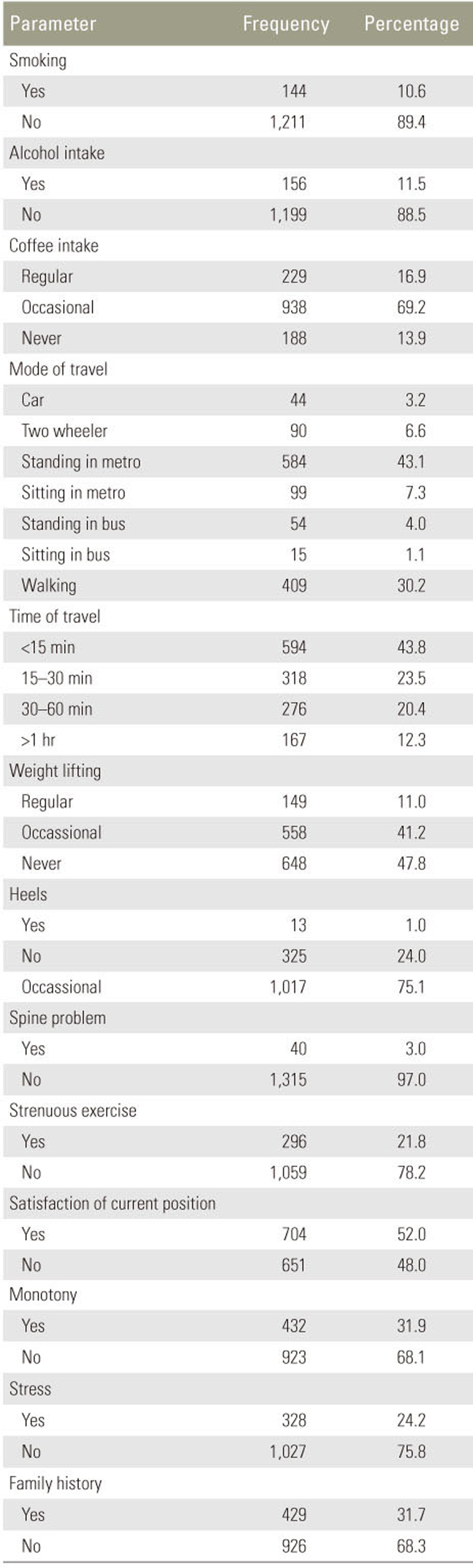
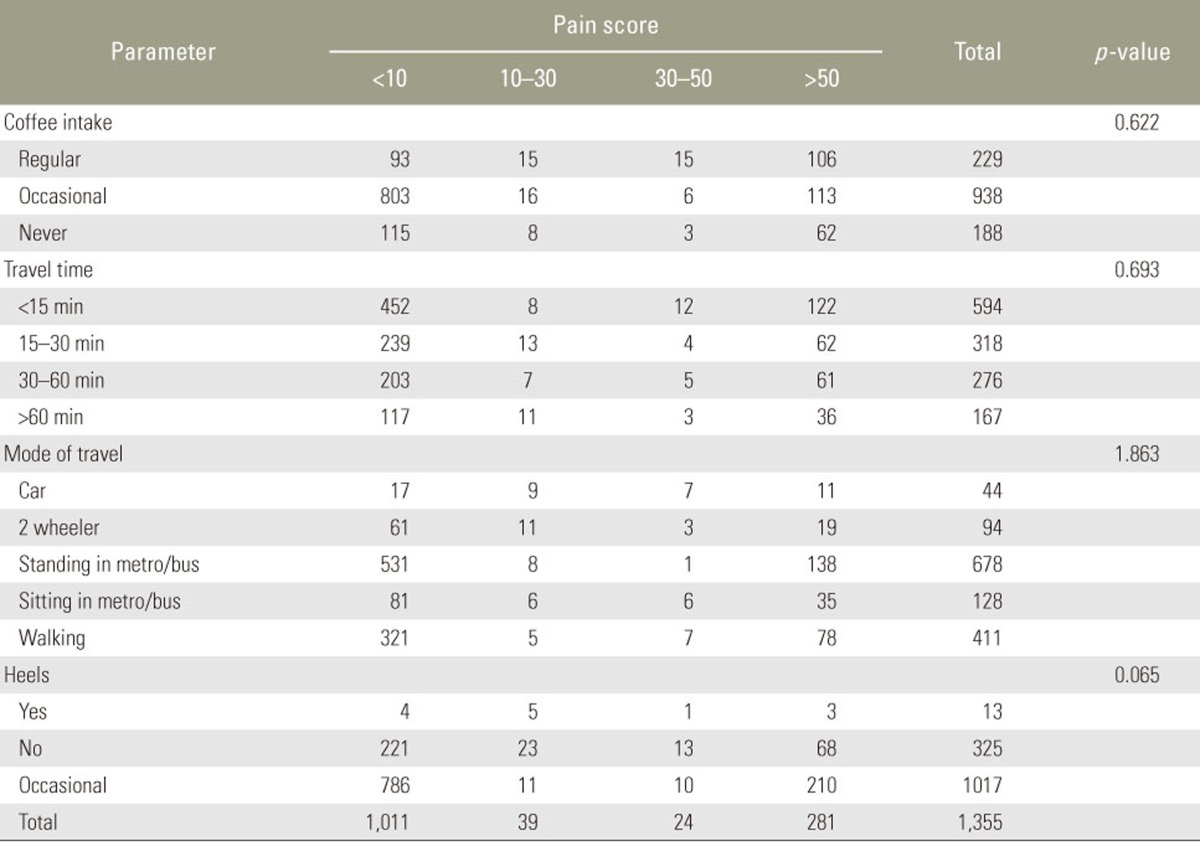
Of the 1,532 subjects, 1,355 (88.4%) submitted completed questionnaires; the remainder were incomplete, and hence, were excluded from the study. Moreover, the response rate was considered to be good. Among the included subjects, 741 (54.7%) were males and 614 (45.3%) were females. Most subjects (90.6%) were aged 20–29 years (mean, 24.49 years; range, 18–35 years). More than half (54.7%) of the study population was non-vegetarian and the rest (45.3%) were vegetarians. The majority (78.8%) belonged to the northern part of the country. Overall, 9.7% of the subjects belonged to the upper scale, 75.8% belonged to the upper middle, 13.8% belonged to the lower middle, and 0.7% belonged to the upper lower scale as per the modified Kuppuswamy scale for the socioeconomic status. Smokers and alcoholics constituted 10.6% and 11.5% of the study population, respectively In terms of coffee intake, 69.2% reported occasional, 16.9% reported regular, and 13.9% reported no coffee consumption. Of the 1,355 subjects, 15.6% were married and 84.6% were unmarried. We found that LBP is precipitated by studying for >5 hours on an average (p<0.05). The LBP prevalence was 42.4% per year and 22.8% per week. Pain was assigned a score of 0–100 and categorized into <10, 10–30, 30–50 and >50. Scores of <10 were considered to be insignificant and scores of >10 were considered to be significant; 94.1% (1,011 of 1,074 subjects) had scores of <10. Approximately one in five (20.6%) patients reported limitations of daily activities that resulted from LBP and 14.4% felt emotionally depressed because of LBP. In total, 52% subjects were satisfied with their current position compared with 48% who were not. Job monotony was reported by 31.9% of our subjects and stress was reported by 24.2% of subjects. The frequencies for other measured variables are depicted in Tables 1 and 2.
Results indicated that the following factors were associated with LBP in young adults: marital status, previous history of spine problems, strenuous exercise, satisfaction in current employment position, monotony, stress, number of daily study hours, and family history of spine problems (Tables 3, 4). Satisfaction with current employment position, monotony, stress, and family history of spine problems were identified as significant predictors of LBP using logistic regression (Table 5). In contrast, age, sex, smoking, alcoholism, coffee intake, mode and duration of travel, diet, frequency of weightlifting, wearing heels, studying posture, and frequency and type of sports activities were not associated with LBP.
Discussion
Various studies [123] reported that LBP is one of the most common causes of hospital visits and that it is the leading cause of activity limitations and work absences in many parts of the world. LBP poses a significant economic threat to the individual, family, workplace, and society. Initially considered to be a problem confined to developed countries, studies have now revealed an increasing prevalence in developing countries [1516]. Although LBP can manifest at any age, LBP prevalence is the highest in the third decade of life [17]. LBP occurrence at an early age can cause disease progression, resulting in chronic LBP that has the potential to decrease an individual's quality of life [8]. Being a common health issue that affects all age groups, LBP and its risk factors have been evaluated by various authors internationally. However, data pertaining to the prevalence and risk factors for LBP in Indian subjects is scarce, particularly in young adults. This study, which included 1355 young adults, was unique as it not only examined LBP prevalence in young adults in Delhi, India, but also analyzed its potential risk factors. Recommendations are provided herein to prevent the modifiable risk factors with which one can expect a reduction in LBP incidence and prevalence.
According to Hestbaek et al. [18], the annual LBP prevalence in young adults is 32.4% compared with 42.4% annually, as observed in the current study. This study demonstrated that there is no sex predilection for LBP occurrence, which is consistent with several studies [19]. Furthermore, our results differ from those of Linton et al. [20] and Thomas et al. [21], which demonstrated a higher incidence in females and who also develop chronic backache compared with males. A meta-analysis by Hoy et al. [22] also showed an increased prevalence in females. Shiri et al. [23] conducted a meta-analysis and found that smokers have a higher prevalence and LBP incidence than non-smokers and that the pain is stronger in adolescents than in adults. Our study results were contrasting, revealing no significant difference in LBP occurrence in smokers and alcoholics compared with non-smokers and non-alcoholics. Similar to the results of Currie et al. [24], our analysis did not demonstrate an association between coffee intake and LBP. Although few studies suggested that BMI is a weak factor in LBP occurrence, a study by Webb et al. [9] showed that higher BMI is associated with an increased LBP incidence. The results obtained in our study showed that BMI did not have a significant impact in LBP development. With regard to the marital status, an increased LBP incidence in married participants was contemplated compared with unmarried subjects.
Static muscle load and flexion of the lumbar spine have been postulated as risk factors for LBP development; thus, prolonged sitting or sitting in an abnormal posture can aggravate LBP [25]. We found that posture while studying had no effect on LBP occurrence; however, the number of daily hours spent studying had a significant association with LBP. We ascertained that LBP is precipitated by studying for >5 hours on an average (p<0.05). We analyzed the mode and time of travel to the institutes and detected that there was no significant correlation between these variables and LBP. Further analysis aimed to examine the association between LBP and posture while traveling (standing vs. sitting), but results revealed no significant correlation between these parameters.
The role of psychosocial factors in LBP development has been emphasized in various studies. Nuwayhid et al. [11] showed that there was no correlation between LBP and job dissatisfaction, whereas other authors [12] demonstrated a significant impact of job dissatisfaction on LBP. Moreover, dissatisfaction with one's job or position can lead to the progression of acute LBP to chronic LBP [26]. In our study, LBP prevalence was significantly higher in the dissatisfied group (p<0.05). A systemic review by Hoogendoorn et al. [13], which evaluated psychosocial factors in the workplace, showed that job monotony increases the LBP prevalence. Similarly, the 31.9% of our subjects who reported job monotony had an increased LBP incidence (p<0.01). Atkinson et al. [14] postulated that stress can precipitate LBP and can cause chronic LBP. Stress had a statistically significant correlation with LBP. Previous research revealed LBP recurrence, which can eventually become chronic [26]. In this study, 3% of subjects had at least one LBP recurrence in the past year, and this recurrence was associated with LBP (p<0.01). In their study of 3,042 factory workers, Matsui et al. [27] concluded that LBP is prevalent in subjects with a positive family history in parents or siblings. Similar to this, our study also showed a statistically significant correlation between a positive family history and LBP (p<0.01). Although studies [628] have demonstrated an increased association of sports and athletic activities with LBP, our study did not show an association between LBP and any type of sport or duration of sports activities. Similarly, our study did not find a significant correlation between LBP and frequency of wearing heels or weightlifting. Some studies [2930] demonstrated that socioeconomic status has an inverse association with LBP; however, we did not find any significant association between these two factors.
This study identified family history as a non-modifiable risk factor, and the number of study hours, marital status, previous history of spine problems, strenuous exercise, job satisfaction, monotony, and stress as modifiable risk factors for LBP in a young Indian population. Satisfaction of one's current position, family history of spine problems, stress, and monotony appeared to be the major contributing factors for LBP development in young Indian adults, as indicated by logistic regression analysis. Lifestyle modifications such as adequate rest, relaxation [14], and recreation can reduce and modify stress and monotony, thereby preventing LBP development. The health and economic status of young adults play a vital role in developing countries such as India. LBP occurrence in the early stages of life increases the risk for chronic, reoccurring LBP, which has the potential to reduce the efficiency of the young population, which in turn may affect productivity.
The limitations of our study included the fact that it was conducted in young adults who were preparing for their entrance examinations. At the time of the study, these individuals often studied for long periods of time, which could be a major contributing factor to LBP occurrence. Thus, these subjects would have likely experienced high stress levels and monotony, which may have exacerbated LBP. Our study did not include sedentary lifestyle as a risk factor for LBP. Although the study sample included subjects from various parts of the country, the majority was from north India, which could be a limitation. Because this study was questionnaire based, the students were not asked to provide details regarding smoking and alcoholism, which could explain why our results contrasted those of other studies. Finally, as this was a cross-sectional study, we could not assess LBP progression in these subjects, except for in a very small number of subjects who returned to our clinic for evaluation of the problem.
Conclusions
This study, conducted among a young adult Indian population, revealed that Indian youth are prone to developing LBP, which aligns with published Western literature. The study also identified various modifiable and non-modifiable risk factors for LBP in young adults. Identification of these risk factors at an early stage will prevent the progression of acute LBP to chronic LBP. As chronic LBP has the potential to curb individual quality of life and increase economic burden, creating awareness about the modifiable risk factors in young adult populations may lead to lifestyle modifications, thereby improving their quality of life and increasing productivity.