Current Concepts of Anterior Cervical Discectomy and Fusion: A Review of Literature
Article information
Abstract
Anterior cervical discectomy and fusion (ACDF) is a safe and effective procedure for degenerative cervical spinal disease unresponsive to conservative management and its outstanding results have been reported. To increase fusion rates and decrease complications, numerous graft materials, cage, anterior plating and total disc replacement have been developed, and better results were reported from those, but still there are areas that have not been established. Therefore, we are going to analyze the treatment outcome with the various procedure through the literature review and determine the efficacy of ACDF.
Introduction
Anterior cervical discectomy and fusion (ACDF) has been accepted as an effective treatment on a various spinal cervical abnormality such as spondylosis, herniated discs, fractures, neoplastic lesion. It has excellent clinical results and relatively safe so that it has been the one of the most common procedure for degenerative spinal cervical disease and more than 5 milion operations have been conducted in the United States between the period of 1990-1999 [1]. A various trials and experiments have been carried out in the last decades to get better results from the procedure, and it was essential to develop new graft materials and implants for this, but these changes could not always guarantee the better results. The authors identified the historical importance of ACDF in disease of cervical spine and have conducted a literature review on the development of clinical results through the changes in operative techniques and instruments.
Historical Review
Anterior cervical approach which is familiar to the spine surgeon was initially described by Lahey and Warren [2] to expose esophageal diverticula. Smith and Robinson [3] first applied this approach to cervical spine and reported the result of anterior cervical interbody fusion by using a horseshoe-shaped graft harvested from iliac crest in 14 patients suffering from radiculopathy. At that time there was no attempt to remove the structure compressing neural structure and simply disc was removed and autologous bone graft was filled in the hollow space to conduct the fusion. They expected that the inserted graft will indirectly decompress nerve root by recovering the disc height, and it was thought that existing osteophytes would regress wtith stabilization of the involved motion segment. Consequently, 9 patients had excellent and 4 patients had good or fair results. The reason that anterior cervical fusion came to the fore, was that the effort for overcoming the limitation of the current posterior approach. Laminectomy was often not effective when posterior osteophytes compress the nerve root in the intervertebral foramen. Furthermore if the radicular pain was bilateral, bilateral facet excision was necessary to adequately decompress the nerve roots by a posterior approach, often leading to instability. They reported the following benefits of ACDF for the treatment of radiculopathy that this operation: 1) has less morbidity than laminectomy, 2) can remove disc pathology without distrubing spinal canal, 3) allows interbody fusion of the cervical spine at the specific intervertebral level from which symptom arise. In November of the same year, Cloward [4] reported interbody arthrodesis by using dowel type graft. It applied Wiltberger's lumbar interbody dowel fusion technique on cervical spine, and unlike Smith-Robinson technique, it removed not only discs but also all lesions that compressing the neural structure anteriorly under direct visualization, and used a large drill to prepare the area for bone graft. They showed the result that 42 cases out of 47 cases had a complete relief, and 5 cases had a partial relief, and more rapid symptomatic recovery was achieved than in cervical laminectomy. Bailey and Badgley [5] reported the technique with slot or trough type graft. This technique was originally attempted to remove tumor on cervical spine. They did not attempt to decompress neural structure directly or restore the disc height, instead they only conducted fusion with an onlay graft. They recommend 6 weeks of postoperative traction on a Stryker frame followed by immobilization in a brace for 4-6 months. This technique is not used today for single level disease, but this concept led to the development of the grafting technique after the corpectomy. In 1969, Simmons and Bhalla [6] reported anterior fusion by using keystone graft, and in 1981, Bloom and Raney [7] modified Smith-Robinson technique and inserted the horseshoe type graft in the reversed way so that cortical portion headed to disc space, so it could be stronger to resist compressive force. Since then a numerous modifications were introduced by many surgeons, and subsequent excellent results were reported so that anterior approach became the treatment of choice for cervical radiculopathy (Fig. 1).
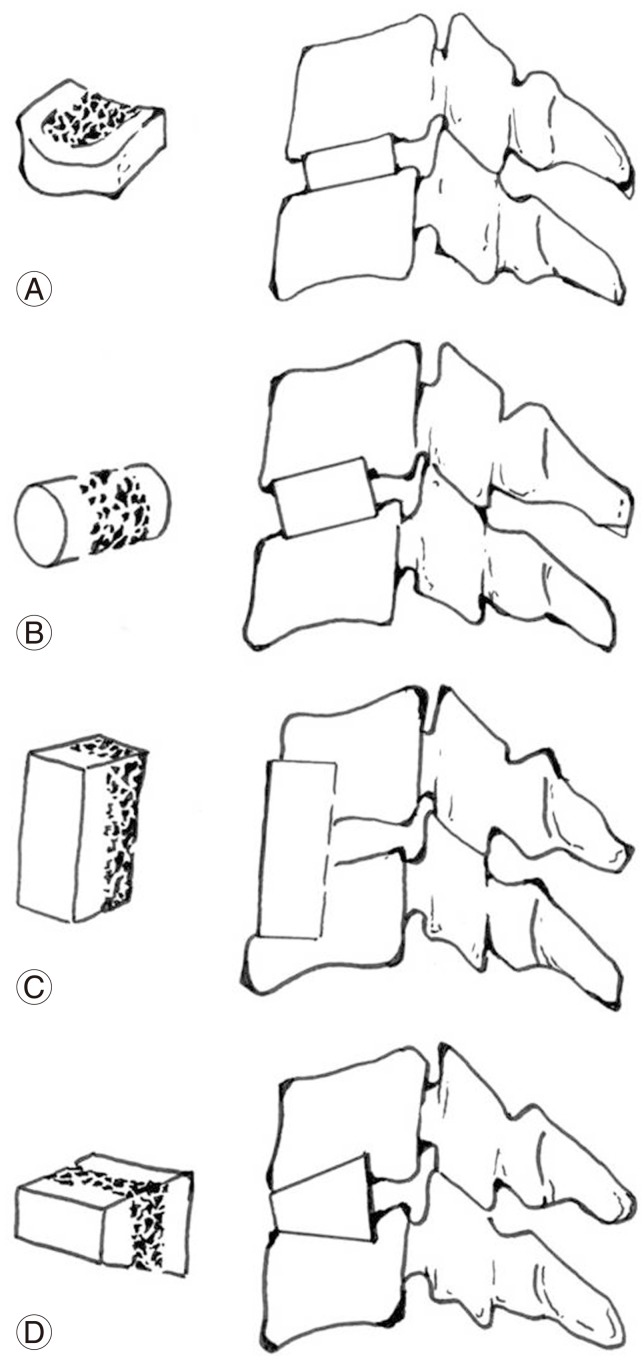
Autogenous bone graft techniques. (A) Smith-Robinson graft (horseshoe). (B) Cloward graft (dowel). (C) Bailey-Badgley graft (onlay strut). (D) Simmons-Bhalla graft (keystone).
Autograft versus Allograft
The history of modification in ACDF is the effort to obtain stable fusion. The ideal graft should have all potentials of osteogenesis, osteoinduction and osteoconduction, and currently the only graft that fulfills all of three properties is autologous bone graft. So far the fusion using autobone graft has been a gold standard with a high fusion rate. Smith and Robinson's [3] horseshoe type tricortical iliac bone graft was found to be much more resistant to compressive forces than the other graft shapes and has been used as the most popular technique in autobone graft [8]. The height of the graft should be a minimum of 7 mm and at least 2 mm higher than the original disc height. The graft should be countersunk into disc space and location which sligthtly posterior to the anterior surface of the adjacent vertebral body is the best position [9,10].
Despite of excellent clinical outcome from ACDF with autograft, there were continuous modifications in surgical technique. One of the most important reasons is a fatal complication of donor site morbidity. The donor site complication due to the use of host bone led to the morbidity rate of 20% or higher [11], and it is presented as pain in the donor site, seroma, hematoma, infection, hip fracture, and meralgia paresthetica. To resolve those problems the use of allogenic bone graft and synthetic devices were suggested, and there was development various new surgical techniques and synthetic materials.
Iliac bone or fibula is used in allograft usally and fibula allograft has been reported to be more effective in maintaining the disc height [12,13]. Although allograft has advantages over autograft in terms of donor site morbidity and surgical time, it is expensive and outcomes of fusion rate, maintenance of disc height and lordosis are worse than autograft. Also the issue with disease transmission cannot be neglected [14]. However when it is used with the addition of cervical plate fixation, the fusion rates become comparable with autograft and has been reported that the patient was able to return to work faster [15,16]. Demineralized bone matrix (DBM) is an allograft with a varying degree of osteoinduction, and it cannot support the disc space on its own, so that it require being used with mineralized allograft or synthetic cage [17].
Bovine bone or calf bone was used as animal allograft (Xenograft). Despite of some favorable datas [18,19], its use has declined due to problems like poor biocompatibility and increased re-operation rates [20,21].
Other Bone Graft Substitutes
A various synthetic materials have been introduced which can substitute autograft (Fig. 2). The use of cage has advantages of shorter operation time, maintenance of intervertebral disc height and lordotic angle and when it is used with cancellous autobone that is packed into the cage, it can reduce the donor site complications and obtain comparable fusion rate to autogenous tricortical iliac bone [22,23]. On the other hand, some reports indicated that the cage itself appeared to have stress shielding onto inserted bone graft so that it reduced the fusion rate, and caused delay in fusion, nonunion and kyphosis due to the cage migration, subsidence and loss of lordosis [24]. Although cortical allograft can be manufactured as a cage, the materials generally used for cage are plastic and metal. Polyetheretherketone cage which is a kind of plastic cage is popularized due to its physical property that has similar rigidity to the normal bone, and it is feasible in radiological fusion analysis [22,25,26]. Usually it is made in a box type which cancellous autobone, DBM or ceramics can be packed. Stainless steel, Ti (titanium), Ta (tantalum) are used for metal cage, and mainly Ti is used. Titanium cage is generally packed with autogenous bone from iliac crest, and there are provided as a variety of form such as mesh type, thread type, box type, etc, and it showed low donor site morbidity, high fusion rates [27,28], but in case of mesh cage, the combination with anterior cervical plate was recommended due to the risk of subsidence [27]. The cage with carbon fiber showed satisfactory results [29], but this device is currently not available in the United States.

Synthetic cages with various design and material. (A) PEEK (Solis, adapted from http://www.stryker.com/emea/Products/Spine/Cervical/SolisPEEK/index.htm, with permission of Stryker). (B) Metal thread (BAK/C, adapted from http://www.zimmer.com/, with permission of Zimmer Inc.). (C) Metal mesh (Ti Surgical mesh, adapted from http://www.synthes.com/, with permission of Depuy Synthes). (D) Tricalcium phosphate (Cervios ChronOs, adapted from http://www.synthes.com/, with permission of Depuy Synthes).
Ceramics are attractive graft option as they avoid donor site morbidity, demonstrate biocompatibility, present no risk of infection or disease transmission. And their supply is virtually limitless and it can be manufactured into a various sizes and shapes. Hydroxyapatite or tricalcium phosphate are most widely investigated for use in the cervical spine. Although threre were problems like slippage or fracture in the beginning, but with continuous development ceramics are now showing relatively favorable clinical outcomes and fusion rates [30,31,32]. On the other hand, the use of biocompatible osteoconductive polymer or polymethylmethacrylate showed poor outcomes [33,34].
Bone morphogenic proteins (BMPs) was first introduced by Urist [35] and was suggested as an innovative material to increase the fusion rate, and the outcome of use in lumbar spine was promising [36,37]. However, in cervical spine, the serious complications such as serious postoperative edema, dysphagia, and ectopic bone formation were reported [38,39] and eventually Food and Drug Administration announced the warning of using BMP in anterior cervical spinal surgery [40]. Currently the use of BMP in cervical spine is an off label, and additional studies are warranted for adequate dosage and delivery method in the future.
1. Cervical plating
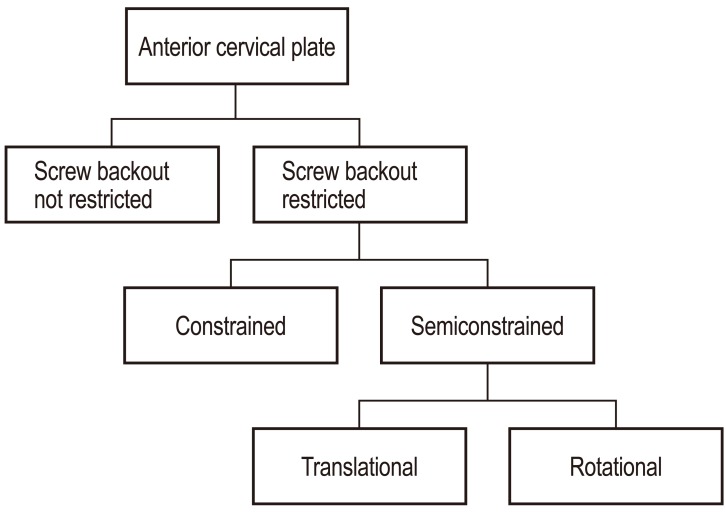
Anterior cervical plate was developed in early 1980 and it was first developed for use in cervical spinal trauma like fracture or dislocation. With successes in trauma, anterior plate fixation has spread to use in degenerative cervical spinal diseases. There are theoretical benefits with additional fixation with anterior plating such as initial stability, early mobilization and minimizing external bracing, prevention of bone graft callapse or extrusion, improved bone fusion and maintenance of sagittal alignment. Although anterior plating in long cervical fusion (two or more levels) with high pseudoarthrosis rate can be justified [16,23,41], the routine use in single-level fusion is still controversial due to the additional cost and possibility of complications with the use of plate [42,43]. Currently the wide array of anterior cervical fixation devices were developed and available. Cervical Spine Study Group [44] has classified them based to the biomechanical characteristics (Fig. 3). The earlier cervical plates had catastrophic issues such as screw backout and esophagus damage, but with the technical advance in implant design including locking mechanism, the complications have been decreased. Also use of locking screw eliminate the nessecity of bicortical fixation and have decreased the possibility of spinal cord damage. Since then the concept of dynamization was introduced and many dynamic plate designs were developed. Compared to the existing static (constrained) plate, dynamic plate has an advantage of early bone fusion because it prevents the stress shielding and transfer axial loading onto bone graft sufficiently through settling [45]. Also metal failure such as screw loosening or breakage due to nonunion and subsidence of bone graft can be reduced. According to the dynamization method, dynamic plate types are classifies as; rotational plate, translational plate with slotted screw holes, translational plate with plate telescope (Fig. 4).

Dynamic plate. (A) Rotationally dynamic plate (Atlantis Vision, adapted from http://www.medtronic.com/, with permission of Medtronic). (B) Translational plate with slotted screw holes (ABC-2, adapted from http://www.aesculapimplantsystems.com/, with permission of Aesculap AG). (C) Translational plate with plate telescope (Atlantis translational, adapted from http://www.medtronic.com/, with permission of Medtronic).
The complications related to the use of plates are rarely reported. Those are loosening of screw or plate, breakage and malpositioning, etc. [46]. There is a controversy that use of plate increases the prevalence of dysphagia which is a relatively common complication of anterior cervical fusion [47], but often cases of esophagus injury have been reported [48]. Adjacent-level ossification (ALO) is an interesting phenomenon occurs in instrumented ACDF but the clinical significance is not clear. It was reported that the placement of plate at least 5 mm away from the adjacent disc helps to reduce the prevalence of ALO [49].
Zero-P system (Synthes GmbH Switzerland, Oberdorf, Switzerland) has the design that fixes the existing stand alone cage onto vertebral body with screws, it shows comparable clinical outcomes and fusion rates relative to using anterior cervical plating, and is reported that it also reduced the prevalence of dysphagia or degenerative change of adjacent segment (Fig. 5) [50].

Image of Zero-P implant (adapted from http://www.synthes.com/, with permission of Depuy Synthes.).
Resorbable plate was developed with the benefit of easy observation of fusion progression on imaging assessment after the surgery due to absence of opacity that metallic plate has. And it was anticipated that it may reduce hardware failure or stress shielding. Although some reports showed favorable results relative to the metal plate [51,52], it should be used with caution as the complications such as early failure, back-out, nonunion and kyphotic deformity.
2. Cervical disc arthroplasty
Since it have been suggested the fused segmentation from anterior fusion increases the load at adjacent segment and it may cause the adjacent segment degeneration, total disc replacement (TDR) that can preserve index level motion was proposed as a new alternative in cervical radiculopathy treatment [53,54] (Fig. 6). The efficacy of total disk arthroplasty has been recognized in stability, clinical outcome and maintenance of index level motion [55,56,57,58], but in the recovery or maintenance of sagittal balance, it showed the similar results to ACDF [59,60]. And complication like heterotopic ossification, prosthetic migration, segmental kyphosis, device failure, wear problem are remained to be resolved in TDR [61,62]. Many studies were conducted on the occurrence of adjacent segment disease (ASD) after TDR, and there were reports that it showed better results compared to ACDF, optimistic outcomes are not guaranteed [63].

Cervical artificial disc. (A) Bryan (adapted from http://www.BryanDisc.com/, with permission of Medtronic). (B) Prestige ST (adapted from http://www.PrestigeDisc.com/, with permission of Medtronic). (C) Mobi-C (adapted from http://www.ldr.com/, with permission of LDR spine). (D) Prodisc-C (adapted from http://www.synthes.com/, with permission of Depuy Synthes).
ASD is a complication with a lot of controversy. It has not been determined if such ASD is the result of the natural progression of degenerative disc disease or biomechanical change after fusion surgery [64]. Also there have been no clear evidence that the increased stress or strain of adjacent segment from the fusion which is indicated as the cause of ASD increases the incidence of reoperation. Even in short-term studies comparing ACDF and TDR have failed to show any significant difference in the prevalence of adjacent segment pathology following surgery [65,66,67]. Existing studies comparing ACDF and TDR have been limited by small sample sizes and by the lack of long term follow-up.
Also the hybrid technique involving arthrodesis and TDR has a biomechanical advantage over two-level fusion in terms of reducing adjacent level hypermobility, but longer follow-up studies are needed to assess the clinical effect [68].
Summary
The aim of ACDF is to obtain sufficient decompression and successful fusion. There was a lot of effort to increase fusion rate and decrease donor site morbidity, and although there was controversy about the use of a various synthetic graft materials and anterior cervical plate, but currently those have been established as a accepted treatment regime for ACDF. The use of cervical plate in ACDF increases fusion rate and has a theoretical advantage of reducing ASD by maintaining cervical lordosis, on the other hand there is a report that it increases stress of adjacent segment and it rather accelerates the adjacent segment degenerative change. TDR is also introduced for reducing ASD, but from the med-long term follow-up of ACDF and TDR, it have failed to identify any significant difference in the prevalence of ASD between them. Eventually the focus on TDR to overcome the limitation of fusion surgery could not show superiority in comparison to ACDF, hence it can be an alternative to fusion surgery, but it will be hard to substitute ACDF.
Conclusions
ACDF showed excellent results for decades in terms of efficacy and safety, and it is an procedure with expectation of better results together with the development of surgical techniques and instruments. However, longer-term follow-up of prospective, randomized multi-center studies are needed to answer the questions about complication or on-going issues like ASD. There is a tendency of expanding indication of ACDF due to its excellent treatment outcomes, but should not neglect the value of conservative treatment in degenerative cerv ical spinal diseases.
Notes
No potential conflict of interest relevant to this article was reported.