Introduction
Routine lumbar axial and sagittal magnetic resonance imaging (MRI) have failed to clearly demonstrate nerve root anomalies and entrapment in the extraforaminal area [1-3], which deterred the diagnosis of conditions such as extraforaminal lumbar disk herniation and foraminal stenosis [3,4]. Nerve root anomalies are of clinical importance for predicting the risk of injury during spinal surgery [5,6], particularly during minimally invasive spinal surgeries such as percutaneous endoscopic procedures and transforaminal lumbar interbody fusion. Furthermore, diagnosis of nerve root entrapment is crucial for optimal treatment [7].
We suggest that oblique lumbar MRI can clearly demonstrate the pedicle, nerve root, ganglion, and radiological anatomy of the foraminal and extraforaminal regions. Here, we present a technical oblique lumbar MRI method and assess its efficacy in diagnosing nerve root anomalies and entrapment lesions.
Materials and Methods
Since 2013, a total of 162 patients underwent initial routine axial and sagittal MRI at the Leon Wiltse Memorial Hospital. Upon suspicion of lumbar nerve root entrapment or anomalous lesions, oblique unilateral or bilateral lumbar MRI was performed. We retrospectively analyzed the oblique MRI data. This study was approved by the Institutional Review Board of the Leon Wiltse Memorial Hospital (IRB approval no., #2015-05) and conforms to the tenets of the Declaration of Helsinki.
1. Indications of oblique lumbar magnetic resonance imaging
Oblique lumbar MRI was additionally performed in patients suspected of having the following diseases or diagnoses upon routine axial and sagittal MRI: (1) foraminal stenosis, (2) nerve root anomalies (furcal and conjoined nerve roots), (3) extraforaminal disc herniations, and (4) nerve root entrapment by various pathologic lesions of foraminal and extraforaminal regions.
2. Procedure of oblique lumbar magnetic resonance imaging
Oblique lumbar MRI was performed with a 1.5-T MRI system (Signa Excite; GE Healthcare, Milwaukee, WI, USA) using a T2-weighted sequence (repetition time, 2,750 ms; echo time, 113 ms; slice thickness, 2 mm; flip angle, 90; field of view, 240├Ś240).
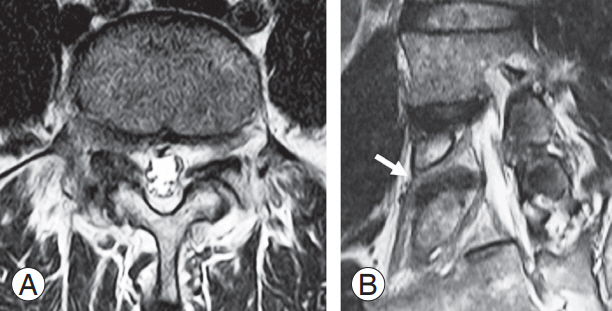
Oblique lumbar MRI was modified for the coronal images. The sagittal line of the oblique image was parallel to the line connecting the posterior margin of the upper end plate to the lower end plate of the affected levelŌĆÖs functional segmental unit (Fig. 1A) [4]. For example, in the case of an L4ŌĆō5 lesion, the sagittal line was a line connecting the posterior margin of the upper end plate of L4 to the lower end plate of L5. The axial angle of the oblique image was parallel to the foramen (Fig. 1B) [4]. In our experience, the axial angle optimally ranges from 17┬░ to 23┬░.
3. Analysis of oblique magnetic resonance images
Two different clinicians assessed the oblique lumbar MR images. In cases of unilateral pathologic lesions, oblique MRI findings of the symptomatic side were compared with those of the asymptomatic side. If the patients presented with unilateral lateralizing symptoms or signs, such as unilateral radiating pain or weakness of the legs, oblique MRI findings of the symptomatic side were compared with those of the asymptomatic side. The exiting nerve root entrapment caused by foraminal stenosis or extraforaminal herniated disc particles in the symptomatic side was compared with that of the asymptomatic contralateral side. Furthermore, the abnormal findings below and above the nerve roots were compared.
Data are presented as mean┬▒standard deviation. FisherŌĆÖs exact test and interobserver agreement (weighted kappa value) were used for statistical analysis using the R software (https://www.r-project.org/).
Results
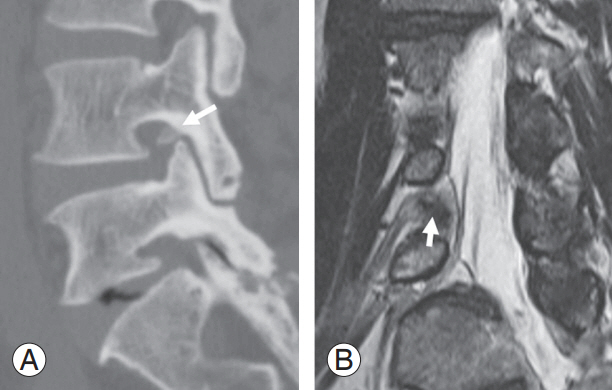
In total, 162 patients (60 males and 102 females; mean age, 59.8┬▒17.8 years) were enrolled in our study (see Table 1 for patient characteristics). Of these, 118 (72.8%) displayed the following abnormal findings: extraforaminal disc herniation in 29 cases (Fig. 1), nerve root entrapment due to foraminal stenosis in 82 (Fig. 2), conjoined nerve root in six (L5 and S1 in four cases, S1 and S2 in two cases) (Table 1, Fig. 3), and foraminal bony cyst in 1 (Fig. 4).
Oblique lumbar MRI clearly demonstrated the pedicles, dorsal root ganglia, and lumbar nerve roots of the foraminal and extraforaminal regions; however, clear images could not be obtained for four patients with degenerative scoliosis and spondylosis. Forty-six patients presented with lateralizing unilateral symptoms such as unilateral radicular pain or weakness. In 43 of the 46 patients (93.5%), unilateral nerve root entrapment due to unilateral foraminal stenosis, herniated disc, or extraforaminal bony cyst were clearly observed when compared with the asymptomatic contralateral side (p<0.05). Interobserver agreement was observed to be excellent for oblique MRI (overall kappa value=0.88) (Table 2).
Discussion
A centrally herniated lumbar disc of the spinal canal can be easily diagnosed using routine axial and sagittal MRI or computed tomography. However, it may be challenging to precisely detect foraminal and extraforaminal lesions, and thus, lead to overlooks on routine axial and sagittal lumbar MRI [3,4,8]. Recently, attempts have been made to use three-dimensional (3D) MRI and 3D MR rendering imaging to evaluate lumbosacral foraminal and extraforaminal lesions [2,3,8,9]. Coronal 3D MRI images have accurately demonstrated the foraminal and extraforaminal regions of the lumbosacral nerve roots and have precisely diagnosed foraminal stenosis and extraforaminal disc herniation [2,3]. Furthermore, diffusion-tensor imaging can help visualize nerve fiber tracts, foraminal stenosis, and extraforaminal disc herniation [8].
The exiting lumbosacral spinal nerve root passes obliquely through the intervertebral foramen in an inferior-ventral direction [10-12]. Therefore, axial, sagittal, and coronal MRI may not precisely demonstrate the spinal nerve root in the extraforaminal region. Conventional foraminal MRI is taken at a right angle to the foramen; thus, foraminal MRI comprises oblique sagittal images. In contrast, our oblique MRI was taken parallel to the foramen and close to the oblique coronal plane. Oblique lumbar MRI was based on the radiological anatomy of the spinal nerve roots. Our findings suggest that oblique MR images can demonstrate foraminal and extraforaminal regions.
In T2-weighted images, the degenerative disc signal was lower than the nerve root signal. Therefore, we performed oblique T2-weighted MRI to detect extraforaminal nerve root compression caused by extraforaminal disc herniation [4]. Because oblique MRI helped compare the abnormal findings between the regions above and below the nerve roots on the symptomatic side as well as the contralateral asymptomatic side, root entrapment or anomalous lesions could be easily detected. Oblique MRI data were easily interpreted with good interobserver agreement. Oblique MRI did not require any additional programs or intravenous injections and could be performed using the 1.5-T MRI scanner.
Despite the advantages of oblique lumbar MRI, the foraminal and extraforaminal radiological anatomy of patients with spinal deformities cannot be demonstrated clearly. Furthermore, it is difficult to determine the axial and sagittal angles of oblique MRI; these angles should be changed in accordance with level due to spinal deformity [4]. Therefore, oblique MRI may not provide adequate information regarding the foraminal and extraforaminal region in cases with scoliosis or hyper-lordosis. Thus, coronal 3D MRI may be more suitable than the presently used oblique MRI for patients with spinal deformities.
Axial and sagittal MRI may not precisely demonstrate anomalous root lesions; hence, spinal nerve root anomalies may be underdiagnosed [5,6]. Although the incidence of nerve root anomalies is very low, anomalous nerve root lesions can interfere with spinal operations. Incomplete decompression or root injury can occur during lumbar spine surgery in cases with unsuspected root anomalies. Here, conjoined nerve roots were clearly detected using oblique lumbar MRI (Fig. 3). Moreover, we detected furcal nerve roots using this technique in a previous study [4]. We suggest that additional oblique MRI can help diagnose nerve root anomalies and provide guidance with respect to their surgical treatment.