Perioperative Evaluation of Respiratory Muscle Strength after Scoliosis Correction in Patients with Duchenne Muscular Dystrophy
Article information
Abstract
Study Design
Retrospective cohort study.
Purpose
To investigate the effect of spinal correction on respiratory muscle strength in patients with Duchenne muscular dystrophy (DMD).
Overview of Literature
Several studies have reported that scoliosis correction in patients with DMD does not improve pulmonary function. In these studies, pulmonary function was evaluated using the traditional spirometric values of percent vital capacity (%VC) and percent forced vital capacity (%FVC). However, traditional spirometry may not be suitable for patients with DMD because the results can be influenced by patient fatigue or level of understanding. Therefore, we evaluated respiratory function focusing on respiratory muscle strength using maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), and sniff nasal inspiratory pressure (SNIP), in addition to %VC and %FVC.
Methods
We retrospectively reviewed 16 patients with DMD who underwent spinal correction surgery between 2006 and 2011 at Kitasato University Hospital. All patients were males, and the mean age was 13.5 years. Respiratory muscle strength was evaluated using MIP, MEP, and SNIP. Measurements were obtained preoperatively and at 1 and 6 months postoperatively, and %VC and %FVC were obtained preoperatively and within 6 months postoperatively.
Results
The mean preoperative and postoperative %VC values were 54.0% and 51.7%, whereas the mean %FVC values were 53.9% and 53.2%, respectively. The mean MIP, MEP, and SNIP values obtained preoperatively and at 1 and 6 months postoperatively were as follows: MIP, 40.5, 42.7 and 47.2 cm H2O; MEP, 26.0, 28.0, and 29.0 cm H2O; and SNIP, 33.4, 33.0, and 33.0 cm H2O; respectively. The mean MIP and MEP values significantly improved postoperatively. There were no significant differences in SNIP, %VC, or %FVC preand postoperatively.
Conclusions
By focusing on respiratory muscle strength, our results suggest that scoliosis correction in patients with DMD might have a favorable effect on respiratory function.
Introduction
Patients with Duchenne muscular dystrophy (DMD) commonly develop scoliosis after loss of ambulation [1]. Most cases are progressive [23], and operative treatment such as scoliosis correction and fusion is considered for all except mild cases [45678]. Many case-control studies and case series have reported that scoliosis correction has beneficial effects on sitting balance [910], quality of life (QOL) [581112], cosmesis, and self-image [1213]. However, its effect on pulmonary function remains controversial.
Previous studies have reported that scoliosis correction improves respiratory function and prevents further respiratory decline [214]. However, several other studies have demonstrated no obvious benefit in terms of respiratory function [591015161718]. In these studies, respiratory function was evaluated using percent vital capacity (%VC) and percent forced vital capacity (%FVC). These tests are strongly influenced by a patient's level of understanding, motivation, and fatigue and may be difficult for patients with DMD to perform. Alternatively, maximum inspiratory pressure (MIP), maximal expiratory pressure (MEP), and sniff nasal inspiratory pressure (SNIP) have been reported to be useful in evaluating respiratory muscle strength in patients with DMD [19202122]. However, no previous reports have evaluated respiratory function using these methods in patients with DMD following scoliosis correction.
In this study, we evaluated perioperative respiratory muscle strength using MIP, MEP, and SNIP, in addition to conventional evaluation methods, to clarify whether scoliosis correction in patients with DMD can improve respiratory function.
Materials and Methods
Approval for this study and for the publication of this manuscript was obtained from the Institutional Review Board of Kitasato University School of Medicine. We retrospectively reviewed the cases of 16 patients with DMD who were surgically treated at Kitasato University Hospital from 2006 to 2011. All patients underwent posterior spinal correction with pedicle screws and sublaminar wiring. The spinal fusion level was between T4 and L5 in all patients. The mean age at the time of surgery was 13.5 years (range, 11–16 years), and the mean body mass index was 20.2 kg/m2 (range, 11.3–24.9 kg/m2). Patient demographic data are summarized in Table 1. The spinal curve was measured using the Cobb angle. Respiratory function was measured using %VC and %FVC, and respiratory muscle strength was measured using MIP, MEP, and SNIP. These parameters were measured by a physical therapist using a RPM01 (CareFusion Co. Ltd., San Diego, CA, USA), with the patients in the sitting position. After ensuring that the bilateral nasal cavities were not obstructed, a mensurative probe was unilaterally inserted into the nasal cavity to measure SNIP. The patients were then instructed to close their mouth and draw in a breath strongly and quickly, starting from the functional residual capacity. The signal from the probe was measured using pressure instrumentation, and the pressure curve was monitored using a personal computer. These series of maneuvers were performed five times in 30-second intervals. To measure MIP, the patients were instructed to strongly draw in a breath at maximal end-tidal volume with the bilateral nasal cavities closed, and the physical therapist measured the intraoral pressure using a mensurative mouthpiece. The MEP values were measured using the same method as MIP, but the patients were instructed to strongly expire from the maximal end of inspiration. These series of maneuvers were performed at least three times in 30-second intervals. Respiratory muscle strength was measured in this manner preoperatively and at 1 and 6 months postoperatively.
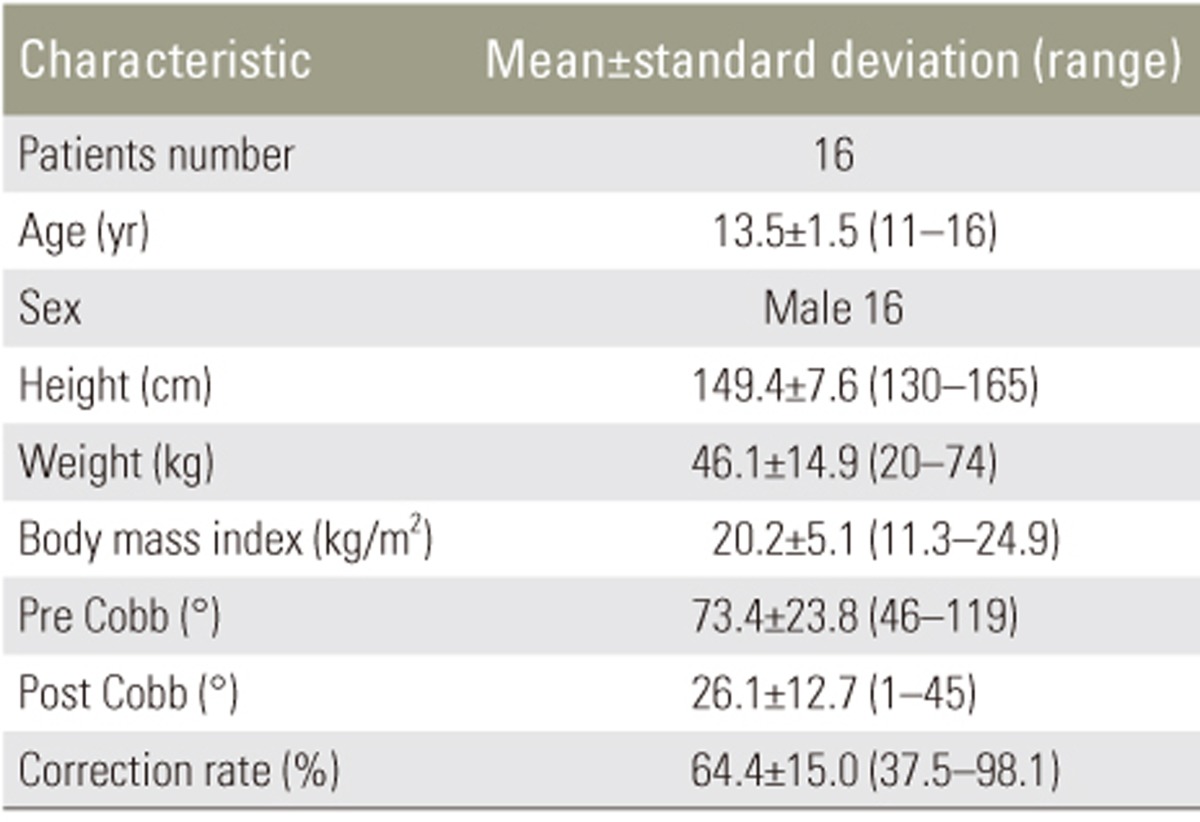
Patients' demographic and radiographic data
The %VC and %FVC values measured by clinical laboratory technicians preoperatively and within 6 months postoperatively were obtained from the clinical records.
Differences between preoperative and postoperative data were analyzed using paired t-test with the SPSS Statistics ver. 19 software package (IBM, Tokyo, Japan). Data are shown as mean±standard deviation. A p-value of <0.05 was considered statistically significant.
Results
The mean preoperative Cobb angle was 73.4°±21.6° (range, 46°–119°), which was corrected to 24.9°±11.2° (range, 1°–45°) postoperatively. The mean correction rate was 67.1%±15.7% (range, 50.0%–98.1%). Radiographic data are summarized in Table 1. The mean MIP values obtained preoperatively and at 1 and 6 months postoperatively were 40.5±13.8, 42.7±16.5, and 47.2±14.5 cm H2O, respectively, showing significant improvement at 6 months postoperatively (Fig. 1). The mean MEP values obtained preoperatively and at 1 and 6 months postoperatively were 26.0±8.5, 28.3±11.5, and 29.3±11.8 cm H2O, respectively, showing slight but not significant improvement at 1 and 6 months postoperatively (Fig. 2). The mean SNIP values obtained preoperatively and at 1 and 6 months postoperatively were 33.4±13.1, 33.2±12.7, and 32.7±12.7 cm H2O, respectively, showing no improvement postoperatively (Fig. 3). The mean pre- and postoperative %VC values were 49.2%±16.2% and 50.1%±18.6%, respectively, and the mean %FVC values were 53.9%±12.8% and 53.3%±12.3%, respectively; %VC tended to increase and %FVC showed no improvement (Figs. 4, 5).
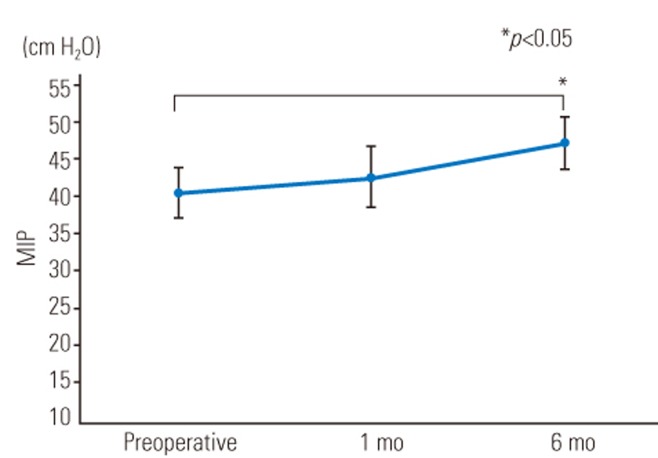
Mean maximum inspiratory pressure (in cm H2O) preoperatively and at 1 and 6 months postoperatively. The error bars in the graph indicate standard error. MIP, maximal inspiratory pressure.
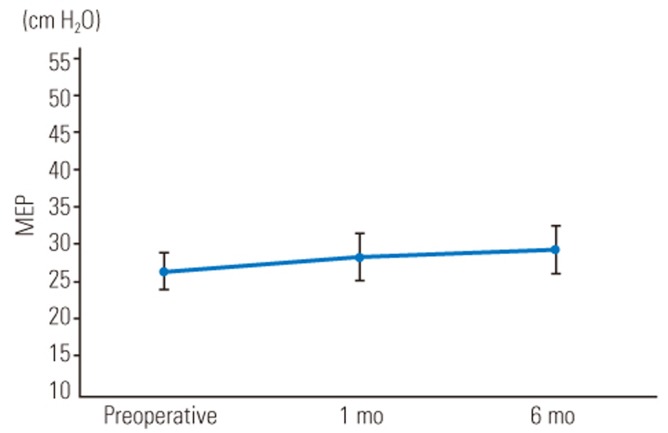
Mean maximum expiratory pressure (in cm H2O) preoperatively and at 1 and 6 months postoperatively. The error bars in the graph indicate standard error. MEP, maximal expiratory pressure.
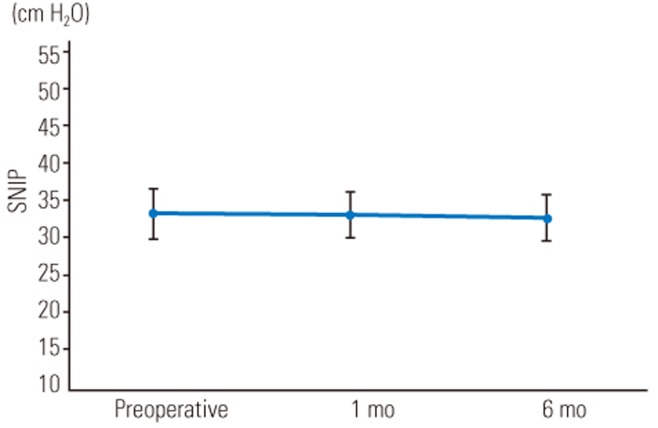
Mean sniff nasal inspiratory pressure (in cm H2O) preoperatively and at 1 and 6 months postoperatively. The error bars in the graph indicate standard error. SNIP, sniff nasal inspiratory pressure
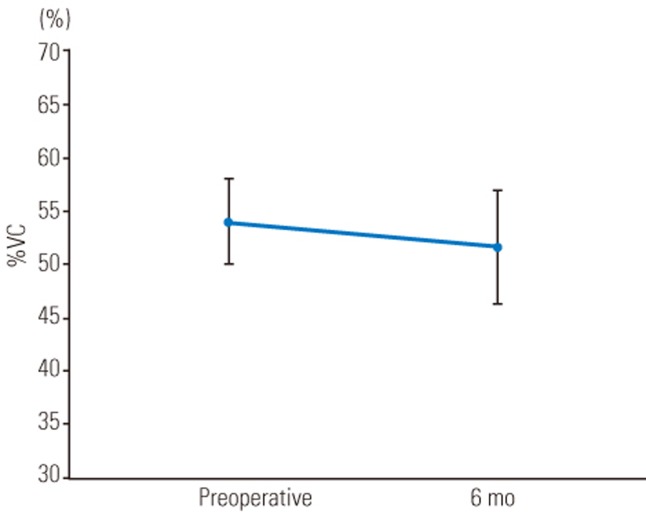
Mean %VC values preoperatively and at 6 months postoperatively. The error bars in the graph indicate standard error. %VC, percent vital capacity.

Mean %FVC values preoperatively and at 6 months postoperatively. The error bars in the graph indicate standard error. %FVC, percent forced vital capacity.
Discussion
We evaluated the effect of scoliosis correction on patients with DMD using respiratory muscle strength tests. Although there was no specific difference in the preoperative and postoperative %VC and %FVC values, we observed small improvements in MEP at 1 and 6 months postoperatively and a significant improvement in MIP 6 months postoperatively. Our results suggest that scoliosis correction improves postoperative respiratory muscle strength in patients with DMD.
Currently, spinal correction and fusion surgery is the mainstay of scoliosis treatment in patients with DMD. The advantages of surgery include increased comfort and sitting tolerance [101223], increased upper extremity function [2324], easier nursing care by parents [12], increased QOL [81112], cosmetic improvement, and higher self-image [1213].
However, the effect of scoliosis correction on pulmonary function remains controversial. Progressive deterioration of respiratory function occurs during the natural course of DMD because of weakening of the respiratory muscles. In addition, deterioration of respiratory function appears to be related to progression of scoliosis [425262728]. After the onset of spinal deformity, scoliosis can rapidly progress and compromise respiratory function [28]. Several groups have thus investigated the effect of scoliosis correction on respiratory function. Several studies have reported the stabilization of VC, FVC, and peak expiratory flow rate or slowing of the rate of %FVC decline in surgically treated patients [214]. In contrast, many studies have reported that scoliosis correction does not improve respiratory function in patients with DMD [5691015161718]. In these studies, respiratory function was evaluated using traditional spirometric values such as VC, forced expiratory volume in 1 second, and peak expiratory flow. These values evaluate respiratory function as a whole, including thoracic compliance and respiratory muscle strength. Furthermore, the results of these tests are easily affected by patient fatigue, motivation, and level of understanding. Thus, traditional spirometry might not be suitable for evaluating the effect of scoliosis correction on respiratory function in patients with neuromuscular diseases such as DMD.
Measurements of respiratory muscle strength, such as MIP, MEP, and SNIP, have been used to evaluate respiratory function in diseases such as chronic obstructive pulmonary disease and neuromuscular disease [19]. Nava et al. [20] used MIP, SNIP, and combined maneuvers (adding MEP after MIP) to differentiate between the respiratory muscle strength of the rib cage, abdomen, and respiratory muscles. Stefanutti et al. [22] demonstrated the feasibility and usefulness of SNIP in a large group of children and adults with various neuromuscular and skeletal disorders. Furthermore, Nicot et al. [21] reported that in 39% of young patients with neuromuscular disease, FVC could not be measured and that SNIP was a more valuable tool for the assessment of respiratory muscle strength in this patient population. These studies suggest that MIP, MEP, and SNIP are suitable tests of respiratory function in children with neuromuscular diseases. In our study, almost all patients were able to perform respiratory muscle strength tests (MIP, MEP, and SNIP) without difficulty (in three patients, MEP could not be measured because of an air leak; the size of the mouthpiece did not fit the patient's mouth).
In the present study, respiratory muscle strength was measured using MIP, MEP, and SNIP and respiratory function was measured using conventional perioperative tests (%VC and %FVC) in patients with DMD who underwent scoliosis correction. Our data are consistent with the findings of previous studies. We observed no significant postoperative improvement in either %VC or %FVC, which supports the view that scoliosis correction does not play a role in the improvement of respiratory function. On the other hand, both MIP and MEP improved postoperatively. Although the exact mechanism has not been fully elucidated, we believe that the deterioration of sitting balance, development of thoracic cavity deformity, and decrement of thoracic cavity compliance due to spinal deformity may negatively influence rib movement and weaken respiratory muscles, including the internal/external intercostal muscles, abdominal rectus muscle, abdominal internal/external oblique muscles, and diaphragm. We speculate that spinal correction improves sitting balance and thoracic deformity, thereby positively influencing respiratory muscle movement. Respiratory muscle strength measurements are capable of detecting these improvements in respiratory muscle movement more sensitively and specifically than conventional pulmonary function tests in patients with neuromuscular scoliosis. Because of these reasons, the respiratory muscle strength values and conventional pulmonary function test results changed differently after spinal correction.
Although MIP and SNIP are both influenced by inspiratory muscle strength, MIP significantly improved postoperatively but SNIP did not. Previous reports have suggested that the agreement between these two tests is relatively poor [20]. Stefanutti et al. [22] pointed out that because of differences in the type of effort and the pattern of muscle activation required by the two maneuvers, the values obtained from MIP and SNIP maneuvers probably reflect different aspects of inspiratory muscle function. It has also been reported that MIP and MEP entirely reflect the strength of the inspiratory and expiratory muscles, respectively, whereas SNIP mainly reflects the contractile strength of the diaphragm [20]. Therefore, the results of this study support the speculation that in the short term, spinal correction can influence inspiratory/expiratory muscle strength rather than diaphragm strength.
It is reported that preoperative respiratory muscle training contributes to pulmonary function improvement [23]. Based on our results, respiratory muscle training particularly focusing on inspiratory and expiratory muscles could produce a positive effect on pulmonary function and possibly reduce perioperative respiratory complications and effectively maintain pulmonary function.
This was a short-term study with a relatively small number of patients. Hence, it remains uncertain whether our findings will be applicable to a larger population. Adequately designed studies with a larger number of patients may help answer this question. Nonetheless, the results of this study may be useful in designing perioperative respiratory rehabilitation programs that slow down the natural deterioration of respiratory function in patients with DMD.
Conclusions
We evaluated postoperative improvements in respiratory muscle strength using MIP, MEP, and SNIP in patients with DMD who underwent spinal correction surgery. The mean MIP and MEP values improved postoperatively. Therefore, our results suggest that respiratory muscle strength improves after scoliosis correction in patients with DMD.
Acknowledgments
This work was supported in part by an Intramural Research Grant (26-6) for Neurological and Psychiatric Disorders from the National Center of Neurology and Psychiatry.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.