Revisional Percutaneous Full Endoscopic Disc Surgery for Recurrent Herniation of Previous Open Lumbar Discectomy
Article information
Abstract
Study Design
A retrospective study.
Purpose
To determine the feasibility and effectiveness of revisional percutaneous full endoscopic discectomy for recurrent herniation after conventional open disc surgery.
Overview of the Literature
Repeated open discectomy with or without fusion has been the most common procedure for recurrent lumbar disc herniation. Percutaneous endoscopic lumbar discectomy for recurrent herniation has been thought of as an impossible procedure. Despite good results with open revisional surgery, major problems may be caused by injuries to the posterior stabilized structures. Our team did revisional full endoscopic lumbar disc surgery on the basis of our experience doing primary full endoscopic disc surgery.
Methods
Between February 2004 and August 2009 a total of 41 patients in our hospital underwent revisional percutaneous endoscopic lumbar discectomy using a YESS endoscopic system and a micro-osteotome (designed by the authors). Indications for surgery were recurrent disc herniation following conventional open discectomy; with compression of the nerve root revealed by Gadolinium-enhanced magnetic resonance imaging; corresponding radiating pain which was not alleviated after conservative management over 6 weeks. Patients with severe neurologic deficits and isolated back pain were excluded.
Results
The mean follow-up period was 16 months (range, 13 to 42 months). The visual analog scale for pain in the leg and back showed significant post-treatment improvement (p < 0.001). Based on a modified version of MacNab's criteria, 90.2% showed excellent or good outcomes. There was no measurable blood loss. There were two cases of recurrence of and four cases with complications.
Conclusions
Percutaneous full-endoscopic revisional disc surgery without additional structural damage is feasible and effective in terms of there being less chance of fusion and bleeding. This technique can be an alternative to conventional repeated discectomy.
Introduction
Recurrent herniation has been reported in 5-11% of patients after disc excision, and represents a major cause of surgical failure. Recent experience indicates that the outcome of the revision surgery for the treatment of recurred disc herniation is favorable [1-5]. However, the surgical options for the treatment of recurrent lumbar disc herniation are still not standardized. In particular, the advantages of repeated disc excision alone or disc excision with fusion is controversial [6]. Although many authors have recommended a repeated discectomy, that could produce less satisfactory results than the primary operations, and approach-related complications could develop [7]. Scar tissue makes a repeated discectomy more difficult, increasing the risk of dural tear or nerve injury. Further removal of posterior structures, including the facet joint, could increase the risk of segmental instability. In recent years, a number of percutaneous endoscopic procedures for lumbar disc herniation have been developed to allow minimally invasive spine surgery that has clinical outcomes comparable to those of conventional open surgery [8-14]. Percutaneous endoscopic lumbar discectomy (PELD) as revisional surgery for recurrent disc herniation has been thought of as an impossible procedure. Ruetten et al. commented that revision surgery can be conducted using the full endoscopic transforaminal and interlaminar discectomy after percutaneous endoscopic discectomy as the index operation [11,15-17]. However, there have been few previous studies on the outcomes of endoscopic discectomy for recurrent lumbar disc herniation after open discectomy as the index operation [18,19]. The purpose of this study was to determine the feasibility and effects of revisional PELD after open discectomy.
Materials and Methods
1. Patient characteristics
Between February 2004 to August 2009 a total of 41 patients underwent revisional PELD in our hospital. There were 13 female and 28 male patients. Their ages ranged from 25 to 70 years (mean, 42.9 years). All patients presented with clinically significant symptomatic recurrent disc herniation following previous open disc surgery and the herniation was confirmed by gadolinium-enhanced magnetic resonance (MR) imaging [20]. Indications for surgery were (i) intractable pain that had not responded to conservative management over 6 weeks and (ii) recurrent disc herniation with compression of nerve root confirmed by MR imaging. The duration of pain-free intervals after previous open disc surgery ranged from 7 months to 13 years. All operations were performed under general anesthesia. Thirty-two patients (78%) underwent an interlaminar procedure and 9 (22%) had a transforaminal procedure. The number of operations at different spinal levels was: 1 at L2-3, 1 at L3-4, 26 at L4-5, and 13 at L5-S1. Interlaminar approaches were done for all cases at L2-3 and L5-S1, and 18 were done at L4-5. The number of transforaminal approaches were: 1 at L3-4 and 8 at L4-5. The authors took an interlaminar approach when ruptured fragments were located in the lateral recess, and took a transforaminal approach when herniations were located at disc level, or when they were central or somewhat proximal to disc level. In L5-S1 lesions, an interlaminar approach was inevitable because of anatomical features. We excluded patients with cauda equina syndrome, combined spinal stenosis, severe neurologic deficits, instability or isolated back pain.
2. Postoperative outcome evaluation
Postoperative outcomes were evaluated using modified MacNab's criteria, and visual analog scales (VAS) for leg and back pain. All patients were notified of their follow up and we received answers to our questionnaires by telephone. The VAS-derived leg and back scores were checked preoperatively and at the last follow-up. According to the modified MacNab's criteria, excellent or good were both defined as successful outcomes. Statistical analysis was done using a paired t-test, for which p-values less than 0.05 were considered statistically significant.
3. Surgical technique: interlaminar approach
The portal site was determined at the intersection of (i) the medial interpedicular line on a posteroanterior (PA) view and (ii) a line parallel to the lower vertebral upper end plate on a lateral fluoroscopy view (Fig. 1). An 8 mm skin incision was made on the portal site with the patient in the prone position on a radiolucent Wilson frame. An obturator is inserted bluntly. Soft tissue and bony margin of previous laminectomy window can be palpated with blunt obturator tip. Working sleeve is slided over the obdurator and endoscope were sequentially inserted into the working sleeve. The surgeon was able to palpate and discriminate scar tissue and the bony margin of the previous laminectomy window. Scar tissues from the bony margin at the superolateral corner of the previous laminectomy window was removed with an endoscopic punch and radiofrequency (RF) waves. Then, an additional partial laminotomy at the superolateral corner of the previous laminectomy window was done with a 2 mm micro-osteotome (Fig. 2). With the aid of a clear endoscopic view, this can be performed safely and without difficulty. A relatively clear endoscopic operating field can be maintained by controlling bleeding using RF and hydrostatic cold water pressure. A small rent between bone and scar tissue in the superolateral corner was a landmark for the site at which the dissection was begun. Dissection with a sharp freer and an endoscopic curett along the bony margin was continued proximally along the bony margin until the normal epidural fat was found. After identifying the epidural fat, the surgeon dissected the epidural scar tissue cranially, caudally and somewhat medially to detect ruptured disc fragments. Usually recurring fragments were walled-off by hard scar tissue and had not migrated far (Fig. 3).
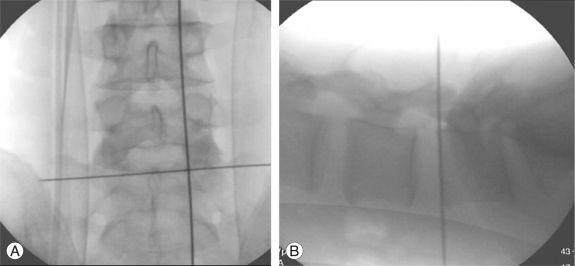
Intraoperative C-arm images posteroanterior view (A) and lateral view (B) with interlaminar access.

Photograph showing endoscopic instruments of the authors' design (A), and a microosteotome (upper) and chisel (lower) (B).
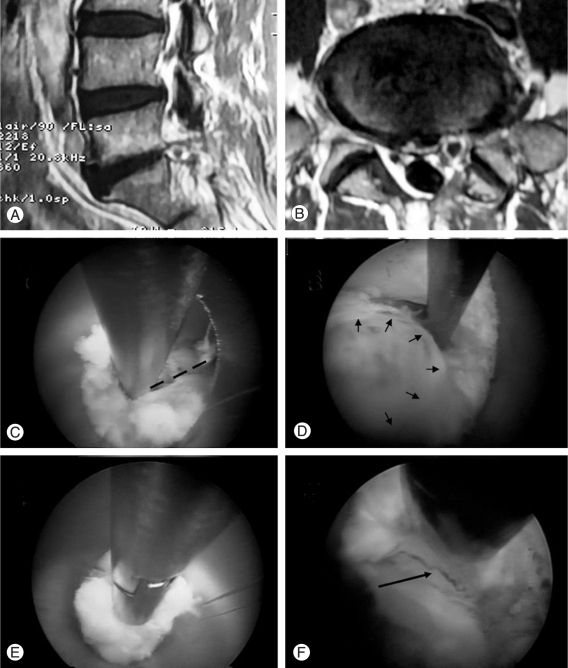
Interlaminar case. (A, B) On magnetic resonance imaging, a ruptured disc at L5-S1 in the left paramedian is seen on sagittal and axial views. (C) Partial laminotomy (dotted line) at the superolateral corner of the previous window with a micro-osteotome is seen. (D) Ruptured fragment are walled-off by epidural scar tissue. (E) Walled off disc fragment are removed with an interlaminar approach. (F) After decompression, traversing the spinal nerve (arrow) can be seen.
4. Surgical technique: transforaminal approach
With the patient in the prone position on the radiolucent Wilson frame, the portal site was determined according to the level and location of the herniation. In case of a central herniation at L4-5, a portal site is farther from the midline - about 12-15 cm. A 6 inch- long, 18 gauge needle was targeted from portal site with a 15-20° angle from the coronal plane, anteromedially towards the anatomical center of the disc. In case of a central herniation at L1-2, a portal site was closer from the midline - about 6-8 cm - with needle insertion at a 45-60° angle from the coronal plane to protect retroperitoneal abdominal organs. A high angular transforaminal approach of upper lumbar vertebra can facilitate access to the midline of the anterior spinal canal because of the large neural foramen, more medially positioned isthmus, and the anatomically large triangular working zone. The ideal position of the needle tip was not beyond the medial interpedicular line on a PA view and the posterior vertebral body line on a lateral view of the C-arm intensifier (Fig. 4). The 18 gauge needle was targeted parallel to the end plate of the vertebra. A guide wire was inserted in the disc through a needle channel. After removing the needle, a bluntly tapered tissue dilating obdurator was slipped over the guide wire until its tip was firmly engaged in the annular window, and then, an endoscope was inserted into the working sleeve. Then, the triangular working zone and the annulus fibrosus were observed, while making the annulus fibrosus window as medial as possible and pushing the working sleeve into the disc space. Decompression was continued under a direct clear visual field and constant saline irrigation. In recurrent herniation, ruptured fragments were walled-off by epidural scar tissue (Fig. 5).
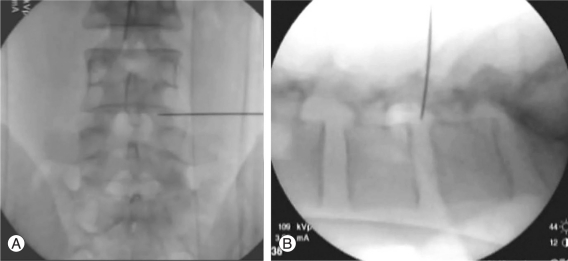
Intraoperative C-arm images posteroanterior view (A) and lateral view (B) with transforaminal access.

Transforaminal case. (A, B) On magnetic resonance imaging, recurrent herniation of L4-5 with peridural scar formation is seen on sagittal and axial views. (C) Walled-off disc fragments are removed with a transforaminal approach. (D) After decompression, dura of cauda equina and scar tissue (arrow) can be seen.
Results
1. Patients characteristics
All 41 patients were included in the follow-up. The mean follow-up period was 16 months (range, 13 to 42 months).
2. Operative techniques
The mean operation time was 37 minutes (range, 25 to 96 minutes). There was no measurable blood loss perioperatively. To find the normal epidural fat, osseous resection was required in all interlaminar cases and in 2 transforaminal cases.
3. Perioperative complications
There were no serious neurologic deficits or complications, such as nerve root injury or cauda equina syndrome. But there were two cases of injury to the thecal sac with cerebrospinal fluid (CSF) leakage. Since the CSF leakage was minimal, the patients were managed by increasing hydration instead of doing open repair. Two patients complained of transient postoperative dysthesia in the leg. The patients were treated with oral gabapentin and improved after 2 months.
4. Recurrences
In two patients (4.8%), recurrences were seen within 3 weeks after the operation. The patients were operated on again with the same technique. Recurring fragments were mixed with desiccated degenerative disc and cartilage materials. The operation times were just 15 and 23 minutes for the 1st and 2nd operations, respectively. The 2nd was finished easily due to the previous laminectomy and little migration.
5. Clinical outcomes
The mean preoperative VAS for leg pain was 8.74 1.50 (range, 5-10) and for back pain was 4.96 ± 2.54 (range, 1-10). At the last follow up, the mean postoperative VAS for leg pain was 2.88 ± 1.01 (range, 1-6) and for back pain was 3.25 ± 1.48 (range, 1-6). There was no significant operation-related worsening of leg and back pain. Indeed, the VAS for the leg and back were significantly reduced (p < 0.001). Based on the modified MacNab's criteria, the surgical outcomes were rated as follows: excellent in 18, good in 19, fair in 2 and poor in 2. Therefore, 90.2% showed excellent or good outcomes.
Discussion
The optimal surgical approach (simple discectomy with or without fusion of the affected segment) for recurrent disc herniation remains a subject of controversy [6]. In 1981, Lehmann and LaRocca [21] treated 36 patients with chronic back and low leg pain following previous lumbar surgery by spinal canal exploration and spinal fusion. By contrast, in the studies of Cinotti et al. [22], Jönsson and Strömqvist [23], and of Suk et al. [5], the clinical outcome was good only with repeated decompression [1]. The open repeated discectomy has been considered the treatment of choice for recurrent lumbar disc herniation [7,24].
Revisional spinal surgery is more challenging than primary surgery due to the following problems. First, epidural or perineural scar tissue could disturb the dissection in the posterior approach, increasing the risk of dural tear or nerve injury [7]. Ebeling et al. [25] reported a complication rate of 13% after repeated discectomy, dural tears or infections being the most common problems. PELD provides an approach through unscarred virgin tissue, especially in the transforaminal approach [7,11,15-18,26-31]. However, when it comes to the interlaminar approach, our team overcame this problem with a feasible solution. We dissected with a sharp freer, an endoscopic curett, and the authors' specially designed micro-osteotome. We did this proximally along the bony margin until finding the normal epidural fat. After finding the epidural fat, we dissected epidural scar tissue cranially, caudally and somewhat medially to detect ruptured disc fragments, and we were able to do so without any problems. Four cases in our study had complications. Two had a dural tear, and the others had postoperative dysthesia. Fortunately, the dysthesia was very mild, and both of the patients recovered and returned to work.
Second, an extended muscle splitting dissection and laminectomy with further facetectomy could cause segmental instability and postoperative low back pain [3,7,32]. PELD does not damage the posterior paraspinal structures (laminae, facets, ligaments, and muscles) when using the transforaminal approach. It makes a resection for neglectable minimal laminectomy with micro-osteotome feasible when using the interlaminar approach and can preserve spinal stability through both approaches [33-38]. Tissue traumatization and complications of PELD are low compared to conventional procedures. We preferred a full-endoscopic interlaminar approach to a transforaminal approach because herniation was located within the spinal canal in all cases. Ruetten et al. reported that resection of intradiscal nucleus materials is frequently constrained because of the divergent level between the interlaminar window and the intervertebral space, which may be partly responsible for the 6.0% recurrence rate when using the interlaminar approach [15-17]. However, the authors overcame the divergence between the interlaminar window and the intervertebral space by widening of the narrow interlaminar window with an author-designed micro-osteotome. Furthermore, the authors selected the transforaminal approach for cases of herniation that were technically inoperable with an interlaminar approach, cases such as foraminal or extraforaminal disc herniation and proximally migrated herniation [39]. Eventually, the authors chose interlaminar or transforaminal approaches, taking into consideration the level and location of herniation because of the different anatomic features at each level.
In the present study, the authors found that full-endoscopic interlaminar and transforaminal operation are possible as revision surgery for recurrent disc herniation. The goal of surgical treatment of recurrent disc herniation is sufficient decompression without neural injury and secondary postoperation trauma. Ruetten et al reported that a full-endoscopic operation achieves results similar to those of microscopic open discectomy [11,15-17]. In our study, there was no significant operation-related deterioration. Therefore, clinical results were good for open revisional surgery as well. The minimally invasive procedure as a new surgical technique was applied in the treatment of recurrent herniation after an open primary discectomy.
In our opinion, there are many advantages over the conventional open disc surgery: excellent visualization of anatomical structures, good illumination and expanded field of vision, reduced anatomical trauma, reduced bleeding, and high patient satisfaction. Moreover, even if the operation time is relatively long, there were no complications associated with epidural edema, which was responsible for the epidural scarring. However, disadvantages must be considered as well. Epidural scarring makes a revisional endoscopic operation more difficult to do as the revisional open surgery. Also, a steep learning curve is required to perform it successfully without complications.
Conclusions
The present study shows that predictably sufficient decompression under visual control is possible using full-endoscopic interlaminar and transforaminal techniques as revisional operations for recurrent disc herniation after conventional open discectomy. The authors have therefore concluded that full-endoscopic interlaminar and transforaminal approaches are possible and are an effective alternative to conventional revisional discectomy.
Notes
Portion of this work were presented in abstract form at the APOA (Asian Pacific Orthopaedic Association), Jeju, Korea, June 7, 2008.