Introduction
Pyogenic spondylitis and tuberculous spondylitis are common causes of spinal infection. The current trend is a decrease in spinal infections due to good nutritional and hygienic status, but an increase in the resistant strains of the organism of pyogenic spondylitis [1,2]. Tuberculous spondylitis has been common in developing countries, and the number of patients with the disease has also been increasing recently in developed countries [1,3,4,5]. Tuberculosis of the spine accounts for 1% of all tuberculous infections, and 25% to 60% of all bone and joint infections are caused by tuberculosis [1,6]. It is important to differentiate tuberculous spondylitis from pyogenic spondylitis, because proper treatment for the different types may reduce the rate of disability and functional impairment [1,6,7]. However, it is difficult to differentiate tuberculous spondylitis from pyogenic spondylitis clinically and radiologically [8,9]. The objective of this review is to discuss the symptoms, laboratory findings, magnetic resonance imaging (MRI) evaluations and management of the two spinal infections according to recent literature.
Classification
There are various classification methods for spine infections. The most basic is by the histologic response of the host to the specific organism [10]. Aetiologically spinal infections can be described as pyogenic, granulomatous and parasitic. Most bacteria cause a pyogenic response, whereas Mycobacteria, fungi, Brucella, and syphilis induce granulomatous reactions [11,12]. Other ways of classifying spinal infections are by the primary anatomic location or spread route. Anatomical classifications include vertebral osteomyelitis, discitis, and epidural abscess. Hematogenous, direct inoculation and spread from a contiguous source are also used in the categorization by spread route.
Incidence
Various reports have stated that pyogenic spondylitis is relatively rare and represents 0.15% to 3.9% of all osteomyelitis cases [13,14]. Vertebral osteomyelitis is more common in the lumbar region, followed by thoracic and cervical spine (less than 10%) [13,14,15]. Bone and joint involvement develops in approximately 10% of patients with tuberculosis, and half of these affected patients have tuberculosis of the spine [12,16,17]. In several studies, the thoracic spinal vertebrae have been found as the most common areas of tuberous infection, followed by lumbar and thoracolumbar spine (in descending order by rate). In pyogenic spondylitis, the lumbar spine is the most common area of infection, followed by thoracic and cervical spine (less than 10%) [13,15,17,18].
Aetiology and Bacteriology
While a wide range of organisms have been associated with spondylodiscitis (bacterial, Mycobacterial, fungal, and parasitic), it remains primarily a monomicrobial bacterial infection. Staphylococcus aureus is the predominant pathogen, accounting for half of non-tuberculous cases (range, 20%-84%). Streptococci (viridans type and b-haemolytic streptococci, particularly groups A and B) and enterococci are well known to be causes of spondylodiscitis (5%-20%) [19,20]. The most frequently isolated gram-negative organisms are Escherichia coli, Pseudomonas species, and Proteus species. These are frequently found in association with genitourinary tract infection. In addition the probable sources of infection are those of soft tissue and respiratory tract among others. Most common causes of iatrogenic disc infection are spinal surgery and invasive manipulation [21,22,23]. Tuberculous spondylitis is most commonly caused by Mycobacterium tuberculosis, but any species of Mycobacterium may be responsible [24].
Pathogenesis and Pathology
Infective spondylitis may result from hematogenous spread, direct external inoculation or from contiguous tissues. The hematogenous arterial route is predominant, allowing seeding of infection from distant sites onto the vertebral column. Wiley and Trueta [25] demonstrated that metaphyses and cartilaginous end plates are starting areas for blood-borne infections, showing how bacteria could easily spread hematogenously to the metaphyseal region of adjacent vertebrae [26]. In pyogenic spondylitis, once microorganisms enter in vascular arcades in the metaphysis, the infection spreads. The disc is destroyed by bacterial enzymes in a manner similar to the destruction of cartilage in septic arthritis. Pyogenic infection commonly involves the thoracic and lumbar spines. In contrast to pyogenic infections, tuberculous infection commonly results from venous spread, Batson's paravertebral venous plexus. Tuberculous spondylitis typically involves initial destruction of the anteroinferior part of vertebral bodies and may then spread beneath the anterior spinal ligament, involving the anterosuperior aspect of adjacent inferior vertebra. Further spread may result in adjacent abscesses [27]. Anterior type involvement of the vertebral bodies seems to be due to the extension of an abscess beneath the anterior longitudinal ligaments and the periosteum. However, tuberculous spondylitis does not destroy the disc until very late in the disease.
Prevalence and Clinical Manifestation
Tuberculous spondylitis has been reported to entail a relatively long, insidious progress from the occurrence and diagnosis compared to pyogenic spondylitis [1,28]. Lee et al. [28] described that for pyogenic spondylitis, it took on average 6.4 months for the occurrence of clinical signs, which include non-specific pain, fever and neurological manifestation from the compression on spinal cord and nerve root. For tuberculous spondylitis, it was 11.2 months on average. Hence pyogenic spondylitis takes a shorter duration for the clinical signs. Buchelt et al. [2] reported that the prevalence period of tuberculous spondylitis was significantly longer than that of pyogenic spondylitis. In addition, Colmenero et al. [7] has reported that tuberculous spondylitis has an approximately 6-months prevalence period. As for tuberculous spondylitis, there were almost no clinical sings such as fever, pain or swelling due to infection and entailed a gradual progress of disease. However, pyogenic spondylitis most likely entails severe pain and high fever [1,6]. The results of the most distinctive clinical findings for pyogenic and tuberculous spondylitis are summarized in Table 1 [28,29].
Diagnosis
The definitive diagnosis of spinal spondylitis can only be made from microscopic or bacteriological examination and culture of the infected tissue. However the diagnosis must be considered in combination with corresponding changes in clinical manifestations, radiological findings, blood and tissue cultures and histopathological findings.
1. Laboratory evaluation
The erythrocyte sedimentation rate (ESR) and gram stain and culture are the commonly used laboratory tests in the diagnosis of pyogenic spine infections [30]. C-reactive protein (CRP) has been shown to be helpful in the diagnosis of infection and has supplanted ESR as the laboratory study of choice for assessing the presence of infection [31]. Koo et al. [29] described that the ESR and CRP level were significantly higher in the patients with pyogenic spondylitis than tuberous spondylitis. Polymerase chain reaction has been used to rapidly identify the presence of mycobacterium in formaldehyde solution-fixed, paraffin-embedded tissue specimens [32].
2. Plain radiologic evaluation
The earliest and most common radiographic finding is narrowing of the disc space in pyogenic spondylitis. It is due to the disc destruction by proteolytic enzyme and is followed by irregularity of endplate from the bone destruction. In progression and healing of the disease, osteolytic changes are followed by new bone formation and osteosclerotic changes at the vertebral margins [21,23]. The findings of plain radiographs for tuberous spondylitis may vary depending on the pathologic type and chronicity of the infection. In early tuberous spondylitis, the disc space is preserved more than pyogenic spondylitis from the lack of proteolytic enzyme. Radiographs may show osteoporosis of body and irregularity of endplate, among others.
3. Magnetic resonance imaging
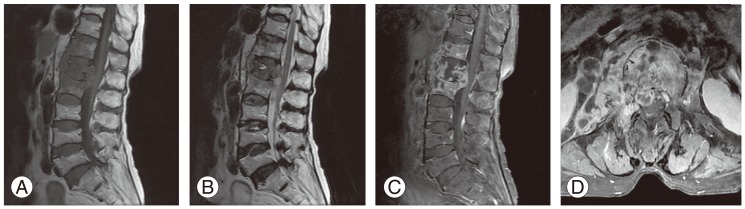
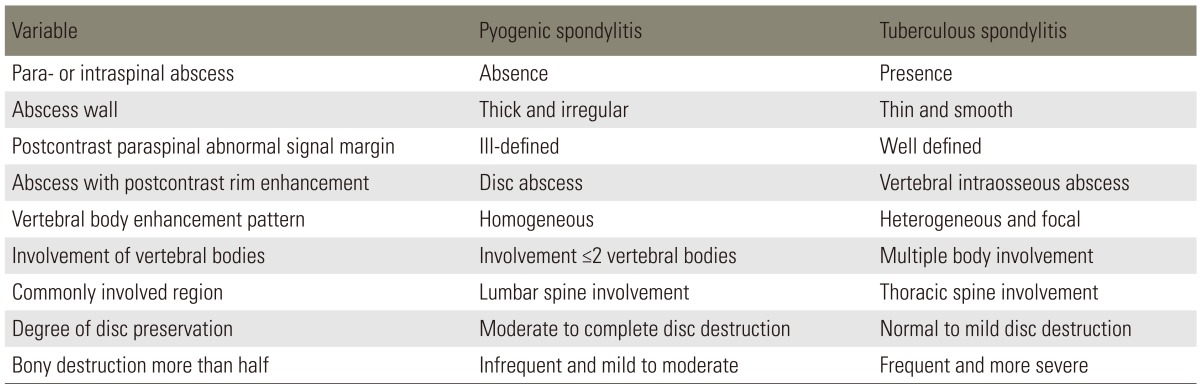
MRI has been reported to be beneficial for early diagnosis and differential diagnosis of the spondylitis and is being extensively used for diagnosis [1,7,33,34,35]. The typical MRI findings of acute vertebral myelitis are low signal intensity in the T1-weighted images and high signal intensity in the T2-weighted images, due to edema of bone marrow in the infected area. However the value of differential diagnosis is low, as there is no specific difference in the contagious causes. In the chronic progress with delayed diagnosis, high signal intensity is sometimes shown in the T1-weighted images [3,34,36,37]. In addition low signal intensity is shown in both T1 and T2-weighted images, if vertebral body has progressed to a collapse and has irregular endplate sclerosis. Hence contrast enhancement images of the gadolinium are specifically required [3,37]. As the MRI is generalized, specific opinions that are beneficial to differential diagnosis of tuberculous spondylitis are being reported by various authors (Figs. 1, 2). Representative opinions deal with abscess in the vertebral body showing contrast enhancement in the peripheral rim, erosion of vertebral body surface, paraspinal abscess with relatively clear border that shows contract peripheral enhancement, extension of anterior longitudinal ligament of the inflammatory tissue and relatively preserved disk [8,34,38,39]. As for tuberculous spondylitis, it typically starts from the anterior cancellous bone in the vertebral body followed by vertebral body starting to be destructed, extending beneath anterior longitudinal ligament and creating an abscess near the vertebral body [1,3,40]. Many of the studies dealing with tuberculous spondylitis have reported that abscess involves uniquely multiple vertebral bodies, especially in gadolinium-enhanced MRIs [34,35,41]. Chang et al. [41] has reported that aforementioned form of contrast enhancement is completely shown in tuberculous spondylitis. Destruction of vertebral bodies in tuberculous spondylitis entails more of such contrast enhancement. It is assumed that abscess is formed more and also available to be used for beneficial indices when performing a differential diagnosis. Epidural extension and epidural abscess formation have been reported to be observed more in tuberculous spondylitis [35,41]. As for paraspinal abscess formed in tuberculous spondylitis, contrast enhancement is known to be more easily performed in the rim of abscess, with the importance of a differential diagnosis [4,41]. In other words, paraspinal abscess is frequently found in pyogenic spondylitis; but well-defined paraspinal abnormal signal, thin and smooth abscess wall and presence of paraspinal or intraspinal abscess are more suggestive of tuberculous spondylitis than of pyogenic spondylitis. On the other hand, if the wall of abscess is relatively thick entailing irregular contrast enhancement, it has been reported to be implying pyogenic spondylitis [30,34,42]. Chang et al. [41] has reported that cases with grade 3 or above and destructed more than 50% of vertebral body height were observed in 82% of all cases in tuberculous spondylitis. Such was observed in 30% of the cases in pyogenic spondylitis. It was concluded that vertebral body was damaged more severely in tuberculous spondylitis than in pyogenic spondylitis. On the other hand, it has been reported that disc is damaged more frequently in pyogenic spondylitis [41,42]. Lack of proteolytic enzymes in Mycobacterium as compared with agents of pyogenic infection has been proposed as the cause of the relatively preserved intervertebral disc, found totally sequestered within the involved vertebrae [1,3,12]. Chang et al. [41] has reported that 57% of a disc was preserved in tuberculous spondylitis, while only 3% was preserved in pyogenic spondylitis. A summary of data regarding the radiologic findings is in Table 2 [4,41].
Treatment
The aim of treatment is to eradicate the infection, restore and preserve the structure and function of the spine and alleviate pain.
1. Conservative management
Conservative management consists of antimicrobial therapy and non-pharmacological treatments, including physiotherapy and immobilization. Immobilization through bed rest is for pain control and prevention of deformity or neurologic deterioration. Length of time for bed rest, type of orthosis and duration of its use depend on location of the infection, degree of bone destruction and deformity and response to treatment. While initial antimicrobial therapy is almost always administered parenterally, its duration varies considerably. In several studies, the mean parenteral treatment duration is at least from 4 to 6 weeks, followed by oral conversion treatment [11,12,20,43,44]. At present, it is recommended that parenteral antibiotic therapy be used in maximal dosage for 6 weeks and followed with an oral course of antibiotics until a resolution of the disease. Criteria for discontinuation of antimicrobial treatment include symptom resolution or improvement and the normalization of ESR or CRP [20,45].
In tuberculous spondylitis, multiple drugs are used because of the potential for resistance to a single agent. Selection of rational combinations of drugs is based on the mechanism of action and toxicity of the agents. A 6-month three-drug regimen including isoniazid, rifampin and pyrazinamide is used for most cases of drug-sensitive infection [24,46].
2. Surgical management
A surgical treatment is required in the following: to acquire bacteriological or histological verification; if there is severe pain; if clinically important abscess is formed; if there is no response after injecting an appropriate antibiotic; if spine is deformed or such needs to be prevented due to a severe damage to the bone; or if there is neurological paralysis [38,47,48,49,50]. An operation may be performed to drain abscesses, to debride sequestered bone and disc, to decompress the spinal cord or to stabilize the spine for the prevention or correction of deformity. There is a broad range of options for the surgical management of spinal infections, which include anterior or posterior approach, single-stage or two-stage surgery and with or without instrumentation. Chen et al. [48] has described a tendency toward a decrease in the incidence of infection recurrence and revision surgery with combined approach as compared with other approaches. Single-stage surgery has advantages including lower complication rate, shorter hospital stay and early mobilization. The two-stage surgery has shorter operation time, less blood loss and increased safety for patients with poorer general health [51,52]. The efficacy of the two-staged operation did not differ between the patients with pyogenic and tuberculous spondylitis [53].
In most cases, the spine should be approached anteriorly, as it allows direct access to the infected tissues and adequate debridement. The use of titanium mesh cages may provide better anterior column support, because their structural integrity is not affected by degradative enzymes present in an infection environment. Interestingly bacteria show lower propensity of adherence to titanium compared with stainless steel [54,55,56,57]. The addition of posterior instrumentation provides even better deformity correction and faster rate of fusion and does not appear to increase the risk of infection [54]. Single-stage anterior and posterior surgery has been shown to be safe and effective using titanium implants [55,56]. Recent advances in minimally invasive spine (MIS) techniques offer alternative methods of surgical treatment. Korovessis et al. [58] showed in a small number of patients that anterior debridement and reconstruction with titanium mesh cages followed by posterior MIS screw fixation led to decreased blood loss and shortened operative time.
In tuberculous spondylitis, most authors agree that anterior radical debridement and strut graft fusion is superior. The spine is approached anteriorly so that the affected area may be dealt with most directly. Oga et al. [59] evaluated the adherence properties of M. tuberculosis and S. epidermidis to stainless steel. The Staphylococcus heavily colonized the rods and was covered with a thick biofilm, whereas only a few biofilm-covered colonies of M. tuberculosis were seen. These findings have prompted the use of anterior instrumentation at the time of initial anterior debridement. Some authors recommend that a posterior fusion should be performed in addition to an anterior fusion in order to eliminate the risk of increased deformity [60,61,62]. Anterior grafts may not provide stable fixation, especially in cases where the graft spans more than two-disc spaces [63].
Conclusions
Pyogenic spondylitis and tuberculous spondylitis entail various types of clinical behavior, and a differential diagnosis is less likely to be conducted. It would be feasible for clinical and radiologic indices to be beneficially utilized on the differential diagnosis, before a culture examination or pathologic examination is performed or in uncertain situations.