Introduction
Whiplash injury is a prevalent and often destructive injury of the cervical column with an annual incidence of 235 per 100,000 people [1]. Whiplash injury leads to serious neck pain, with side effects remaining for 2 years postinjury in approximately 50% of patients.
Studies have shown that neck injury should be controlled and treated quickly to avoid further injury. Many approaches have been suggested to manage whiplash injury, including anti-inflammatory drugs, manipulation, supervised exercise, and cervical collars.
In many cases, no clinical signs present immediately after injury to the cervical column. Therefore, neck immobilization using cervical collars, even before radiographic evaluation has been completed, is a standard treatment approach for patients suffering from multiple injuries. Using a cervical collar is the first intervention when encountering cervical column injuries.
Cervical collars are generally divided into two groups: soft and rigid collars. Routinely, soft collars are prescribed for whiplash injury; however, some studies have suggested the use of rigid collars [23]. The primary function of cervical collars is to immobilize the cervical spine [4]. Cervical collars are typically used for an extended period of time, and they should immobilize the head and neck movement while allowing for normal daily activities. Rigid collars provide more immobilization in the sagittal and transverse planes compared with soft collars. However, some studies have shown that soft and rigid collars both provide the same range of motion (ROM) in the frontal plane. Another study using a goniometer showed that the cervical column is limited more by rigid collars than by soft ones in all planes. Patient comfort is a critical factor, which encourages caregivers to give preference to soft collars in prescriptions.
Considering that both rigid and soft collars are prevalent in the treatment of whiplash injury, the present study aimed to compare the effects of soft and rigid cervical collars on immobilizing head and neck motion.
Materials and Methods
1. Participants
This semi-experimental study examined 29 healthy people aged 18–26 years without any history of neck surgery or orthopedic problems in the shoulders and spine. All participants signed an informed consent form. To calculate the sample size, considering a confidence level of 99% and power of 80%, we used a similar study to calculate sample size. Table 1 shows demographic information of the participants. This study was approved by the medical ethics committee of University of Social Welfare and Rehabilitation Sciences.
2. Intervention
Soft and rigid cervical collars (Teb Sanat, Tehran, Iran) were tested in this study. The neck environment and length were used to determine the proper size of cervical collar for each participant, according to the manufacturer's instruction. Soft collars are flexible and composed of polyurethane foam rubber. It is easily wrapped around the neck and secured with a Velcro strap for support. Rigid collars are composed of hard polyethylene covered by a soft pad for patient comfort. It also had a Velcro strap in the back part of the neck for ease of removal (Figs. 1, 2).
3. Equipment
In the present study, data collection was performed using a three-dimensional (3D) motion analysis system (VICON) and six infrared cameras. Additionally, eight markers, weighing 4.4 g and thickened 2 cm2, were used and positioned on the seventh cervical vertebrae (one marker) below the jugular notch (one marker) on the right and left acromioclavicular joints (two markers) and at the anterior and posterior of the head (four markers). The markers were used to collect kinematic data [56]. Fig. 1 shows the positions of the markers. All tests were performed in the biomechanics laboratory of the University of Social Welfare and Rehabilitation.
4. Measurements
Measurements were performed in three conditions: no collar, soft collar, and rigid collar. To become familiar with the cervical collars, subjects were asked to wear the collars for 10–20 minutes before testing. They were instructed to perform six different neck motions including flexion, extension, rotation to the left and right, and lateral bending to the left and right using no collar and with collars. They wore the collars while sitting on a chair. Their head was in a neutral position facing anteriorly, focused on a point positioned at the level of the participant's eyes. All were asked to move the neck at a self-selected speed and force. Soft and rigid collars were utilized in a random sequence by each subject. During the test, all data obtained were recorded by a computer connected to the cameras (Figs. 3, 4).
5. Data processing and analysis
Data were analyzed using MATLAB (The Math-Works, Natick, MA, USA). The motion of the cervical region was calculated as a motion of the head relative to the upper body [5].
6. Statistical analysis
SPSS software ver. 16.0 (SPSS Inc., Chicago, IL, USA) was used to analyze data. Normality of the data was assessed using Kolmogorov-Smirnov test. According to the normality of the data, a paired t-test was utilized to analyze the effect of soft and rigid collars on the neck ROM in six different motions. The level of significance was set at α=0.01.
Results
Table 2 provides information on the neck ROM with no collar and with soft and rigid collars. All motions significantly decreased when subjects used soft collars (p<0.01). According to the data, flexion experienced maximum immobilization (39%) and lateral rotation experienced the minimum immobilization (11%) among all six motions when soft collars were used. Similarly, a reduction of the neck ROM was significant in all motions when subjects used rigid collars (p<0.01). Rigid collars caused maximum immobilization in flexion (59%) and minimum immobilization in lateral rotation (18%).
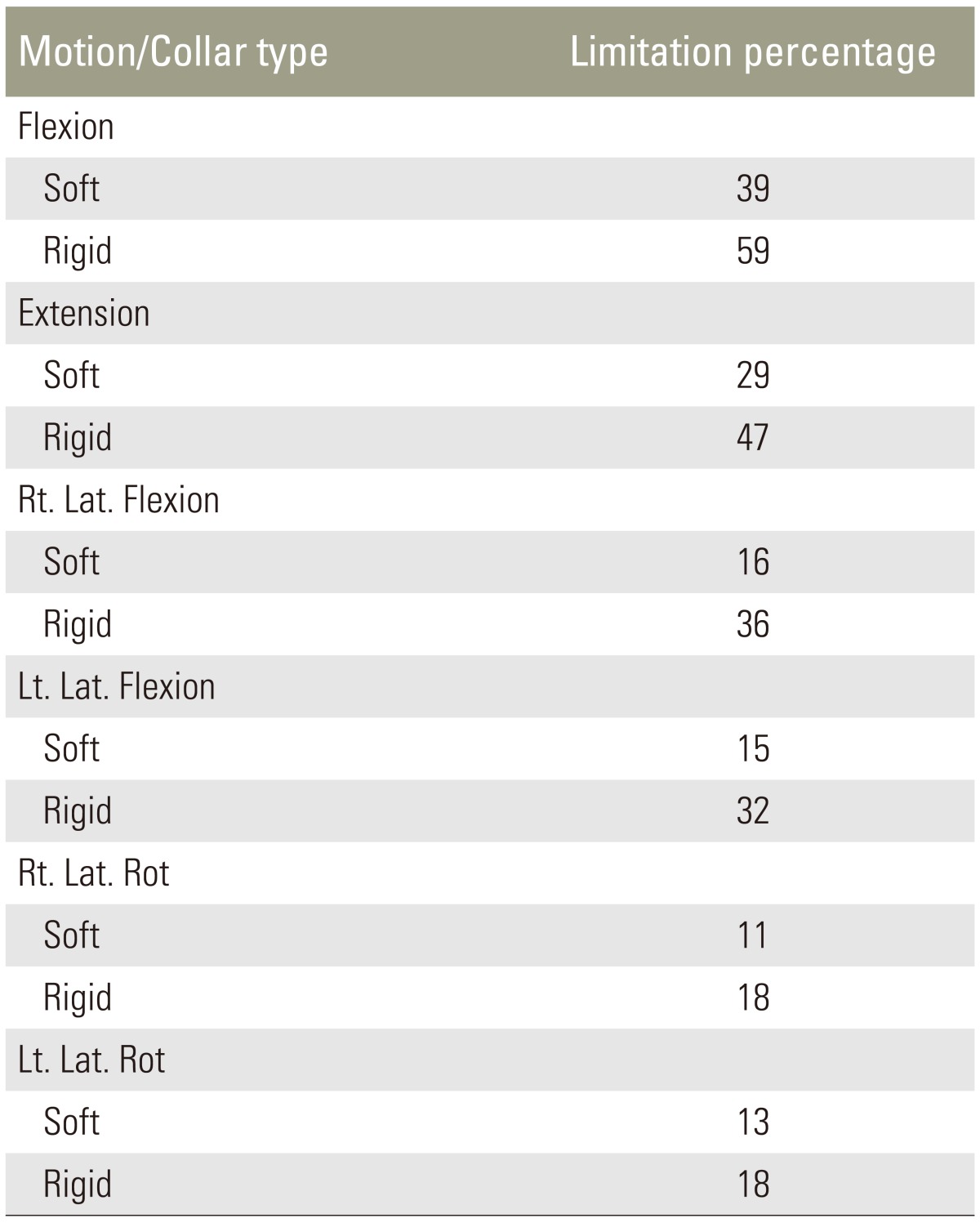
Table 3 shows the percentages of immobilization caused by soft and rigid collars in the six different motions. Rigid collars limited all motion much more than did soft collars. The minimum difference between soft and rigid collars in immobilizing the neck motion was related to the lateral rotation toward the right and left sides (Tables 3, 4, 5).
Discussion
The present study aimed to evaluate the effect of soft and rigid collars on head and neck immobilization. This study was performed using 3D motion capture to assess the head and neck ROM. This method is non-invasive and more reliable than other tests. This study was performed on young healthy participants without motion limitations.
For the neck ROM in subjects who were not using any cervical collar, 51° of flexion, 61° of extension, 41.5° of lateral flexion to the right, 41.3° of lateral flexion to the left, and 64.2° of lateral rotation to the right and the left were observed. Due to the variety of methods used to measure ROM, it is difficult to compare our results with those of other studies. However, our results were similar to those reported by some previous studies [3789].
The results of this study indicated that soft and rigid collars both limited head and neck ROM. This result is similar to those of previous studies [310].
Rigid collars, compared with soft ones, contributed to significantly more immobilization in all directions including flexion/extension, lateral flexion to the right/lateral flexion to the left, and rotation to the right/rotation to the left. These differences may be due to the different materials of soft and rigid collars. This result is consistent with those of other studies [310].
This study indicated that different cervical collars have different effects on neck motion. The immobilization on flexion (soft 39% and rigid 59%) was greater than that on extension (soft 29% and rigid 46.4%), which could be due to the fact that the extensors of the neck are more powerful compared with the flexors in people aged 18–25 years. Our results are similar to that of previous studies [4911].
The results of the present study showed that flexion and extension of the neck were more immobilized when compared with lateral flexion and rotation while subjects were using cervical collars. It can be due to the absence of a counter to limit lateral flexion and rotation. This result was similar to those of previous studies [37910].
For whiplash injury to be treated, cervical collars should be used for an extended period of time [12]. Thus, immobilization should create minimum discomfort to the patient in daily activities [13]. Daily tasks typically require 30%–50% of the neck ROM [141516].
Considering that 30%–50% of the neck ROM is required to perform daily activities, soft collars did not sufficiently limit the neck ROM. Neck immobilization by rigid collars was sufficient only in the flexion/extension. This finding was similar to those of previous studies [1017].
Flexion and extension are the most repetitive motions in the neck which could be limited by rigid collars by 59% and 47%, respectively [14]. However, soft collars limited flexion and extensions by 39% and 29%, respectively.
One limitation of the present study was the lack of recruitment of subjects in different age groups. Few studies have been conducted on people in different age group, and most studies have evaluated subjects of age 20–30 years. Since elderly people generally require cervical collars after whiplash injury, a study on older subjects should be conducted. Furthermore, this study examined healthy subjects; future studies should be performed on injured subjects. As the neck motions were separately examined in the current study, investigating neck motion concurrent with daily activities while using cervical collars should be a focus of further research. A lack of long-term effects of cervical collars was another limitation of the present study.
Conclusions
The data in this study showed that both soft and rigid collars limited head and neck motions. However, subjects experienced more immobilization in flexion/extension than in lateral flexion and rotation. Finally, rigid collars resulted in more immobilization in all directions compared with soft collars.