Introduction
Spinal cord tumors are common lesions that resemble 5%–15% of all central nervous system tumors. Meningiomas originate from arachnoid cells, and only 10% are found extracranially [1]. Intradural extramedullary spinal tumors account for 80% of all intradural spinal tumors [1]. Spinal meningiomas represent 7.5%–12.7% of all meningiomas; majority of these are present in the thoracic spinal cord, and few are reported in the cervical area. Almost 27% of all whole cervical meningiomas are reported in the upper cervical spine, with only 3% being reported in the foramen magnum area [2,3]. Topographically, they are located either ventral or ventrolateral to the spinal cord in almost 50% of the patients.
These lesions are predominant in women, and the clinical presentation of upper cervical spine meningiomas may be nonspecific. Symptoms range from axial neck pain that is usually intense in the evening and morning to significant neurologic manifestations. Specific presentations related to neural compression include radiculopathy, myelopathy, Brown-Sequard syndrome, and complete cord transection [4].
Standard imaging modalities include contrasted magnetic resonance imaging (MRI), complementary computed tomography (CT)-scan, and plain radiography because these lesions are isointense and are rarely associated with calcifications or bone erosions [5]. Complete microsurgical excision is the gold standard treatment and can be accomplished via different accesses. As these lesions are located ventral or ventrolateral to the spinal cord, their surgical excision, without manipulation of the spinal cord and roots is challenging. Most surgeons operate these lesions via the standard posterior midline approach, while few operate via the lateral approach and rarely via the anterior midline approach [6-9]. Choosing the best access is critical and is mainly based on the spinal level, size, and topographic location of the lesion as depicted on images as well as surgeon experience and preferences.
Ventral and ventrolateral meningiomas require precise preoperative planning for a safe corridor to achieve safe and complete tumor excision [10]. Traditional posterior midline approach requires spinal cord and roots traction, and manipulation for accessing ventrally located lesions that can endanger the patient’s neurology and completeness of tumor excision [6,7,11]. The far-lateral approach that was used in this study is a modification of the transfacetal approach (type A) of the extreme lateral craniocervical approach for ventrally located cervical lesions [12]. The lateral approach has been designed to overcome the drawbacks of the posterior midline approach [11-18]. We consider that this is the procedure of choice in our hands for these tumors. It provides safe access to these tumors without cervical spinal cord manipulation or effect on the vertebral and cervical muscle stability. Moreover, the positioning of patients is more convenient from the anesthetics point of view in some patients.
Here, we present our experience with the far-lateral approach to ventral or ventrolateral upper cervical and foramen magnum meningiomas. We also conducted a review of the literature and compared our results to similar previous reports and the standard posterior approach.
Materials and Methods
We conducted a retrospective descriptive clinical case cohort study with a literature review at the Neurosurgery Department, Suez Canal University Hospital, Ismailia, Egypt. We reviewed our hospital medical records from January 2007 to June 2019 for all patients operated for spinal meningiomas. We were able to trace the medical records of 113 patients who had been operated for spinal meningiomas; 49 of them were cervical patients. In this study, we enrolled only those patients who were operated via the far-lateral approach for either ventral or ventrolateral meningiomas of the upper cervical spine and foramen magnum area.
Only 27 patients met these criteria. Of these, only 23 patients had complete medical records in terms of the preoperative, operative, postoperative, and contact data; the other four were excluded because of insufficient data.
The upper cervical spine in this study involved lesions from the fourth cervical vertebra up to the foramen magnum. The foramen magnum, as described by George et al. [19], is the zone defined anteriorly by the lower one-third of clivus to the upper edge of the axis vertebral body, laterally from the jugular tubercles to the upper edge of the C2 lamina, and posteriorly from the anterior edge of the squamous occipital bone to the spinous process of the axis vertebra. Other lesions from the foramen magnum down to the lower edge of C4 lamina were also studied. Lesions below C4 were excluded because in these lesions, the shoulder will hinder the far-lateral approach. Moreover, we excluded redo tumors, lesions involving the posterior aspect of the Forman magnum, and upper cervical spine, or lesion originating primarily from other areas and invading our areas, as well as all other non-meningioma tumors and those treated with the standard posterior midline approach. Surgical tumor excision has been defined as total when grossly removed, subtotal when some remnant is left attached to either of the nerves or the vertebral artery, and partial when a bulky mass was left [20].
We reported all relative demographic data, clinical data, surgical technique details, pathological type of tumors, surgical complications and morbidity, and postoperative clinical and radiological outcomes. Our institutional hospital ethical review board (Research Ethics Committee of Suez Canal University Faculty of Medicine) approved the study (IRB approval no., 4122) and waived the need for informed consent from the study subjects.
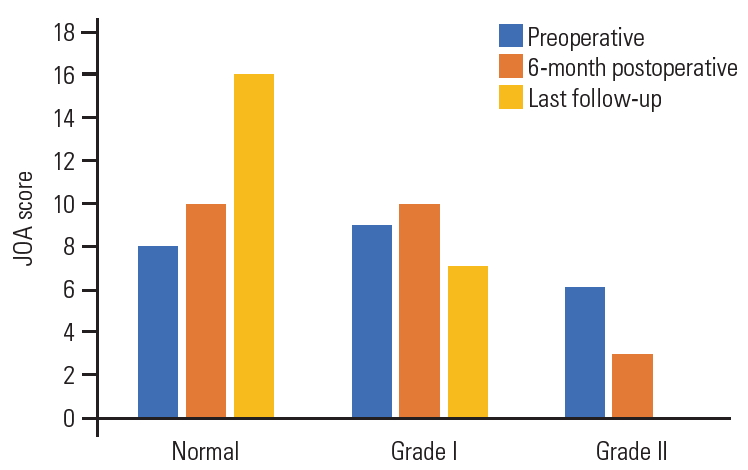
Of the total 23 patients, 17 (74%) were women and 6 (26%) were men, with a mean age of 57.3±15 years (range, 41–66 years). Gait disturbance was the major complaint in our patients and was reported in 15 patients (65%), while radicular pain was reported only in 5 (21.7%), and urinary precipitancy was reported in 2 (8.7%). The mean preoperative duration of the symptoms was 13.4±10 months (range, 5–27 months). As per the 17-points Japanese Orthopedic Association (JOA) scale [21], eight patients (34.8%) were classified into grade 0 (16–17), 9 (39%) into grade I (12–15), and 6 (26%) into grade II (8–13) (Fig. 1). Five patients had hypertension, four had diabetes mellitus, and one had rheumatoid arthritis.
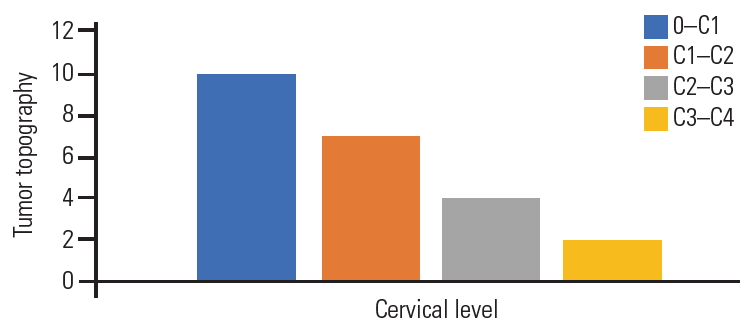
Plain radiography was performed for all patients in the anteroposterior and lateral views; T-1 and T-2 weighted images MRI of the cervical spine with gadolinium enhancement in the sagittal, coronal, and axial views; and six patients were submitted to multiple sclerosis-CT-scan. Seven patients (30.4%) experienced mainly ventral meningiomas to the spinal cord, and 16 (69.6%) had ventrolateral meningiomas. The foramen magnum was involved in 10 patients, C1–2 segment in seven, C2–3 segment in four, and C3–4 segment in two (Fig. 2). Based on the topographic location of the meningiomas, 15 patients were approached from the left side, and only eight were operated from the right side. All the meningiomas were considered large because their cross-sectional area exceeded 50% of the spinal canal as per the measurement on MRI axial images.
1. Operative technique
The patient was placed in the lateral decubitus position under general anesthesia with the head fixed in a Mayfield head clamp. The head was fixed in the dead lateral position with some flexion and contralateral tilt. An incision was marked as per the target segment either straight or lazy “S” one finger-breadth behind the mastoid process. Dissection started between the sternomastoid muscle anteriorly and the trapezius muscle posteriorly and down in the facial plan between the scaleni muscles anteriorly and levator scapulae posteriorly, continuing deeply with finger palpations targeting the tip of the atlas transverse process. In the lower pathology, the fingertip was directed to the lateral mass of the target cervical segment.
C1 transverse process was palpated just inferior to the mastoid tip; thereafter, the muscles attachments to it were resected. The ipsilateral lamina of the cervical spine was palpated, and a Cobb muscle elevator was used to remove the deep cervical muscle attachments subperiosteally and gently from the lamina to protect the vertebral artery from injury [22]. Exposure of the hemi-laminae according to the target level was conducted. Using high-speed drill and Kerrison rongeur, laminotomy was performed and extended from the fact joints anteriorly to the base of the corresponding spinous process posteriorly, using the retro-facet approach. In a similar manner, and in the foramen magnum meningiomas, a suboccipital craniotomy could be performed. After full dural exposure, a vertical dural incision as per the target level was performed, and dural edges were stitched to the ipsilateral muscles. Dentate ligaments were sharply incised to allow tumor access and relax the spinal cord.
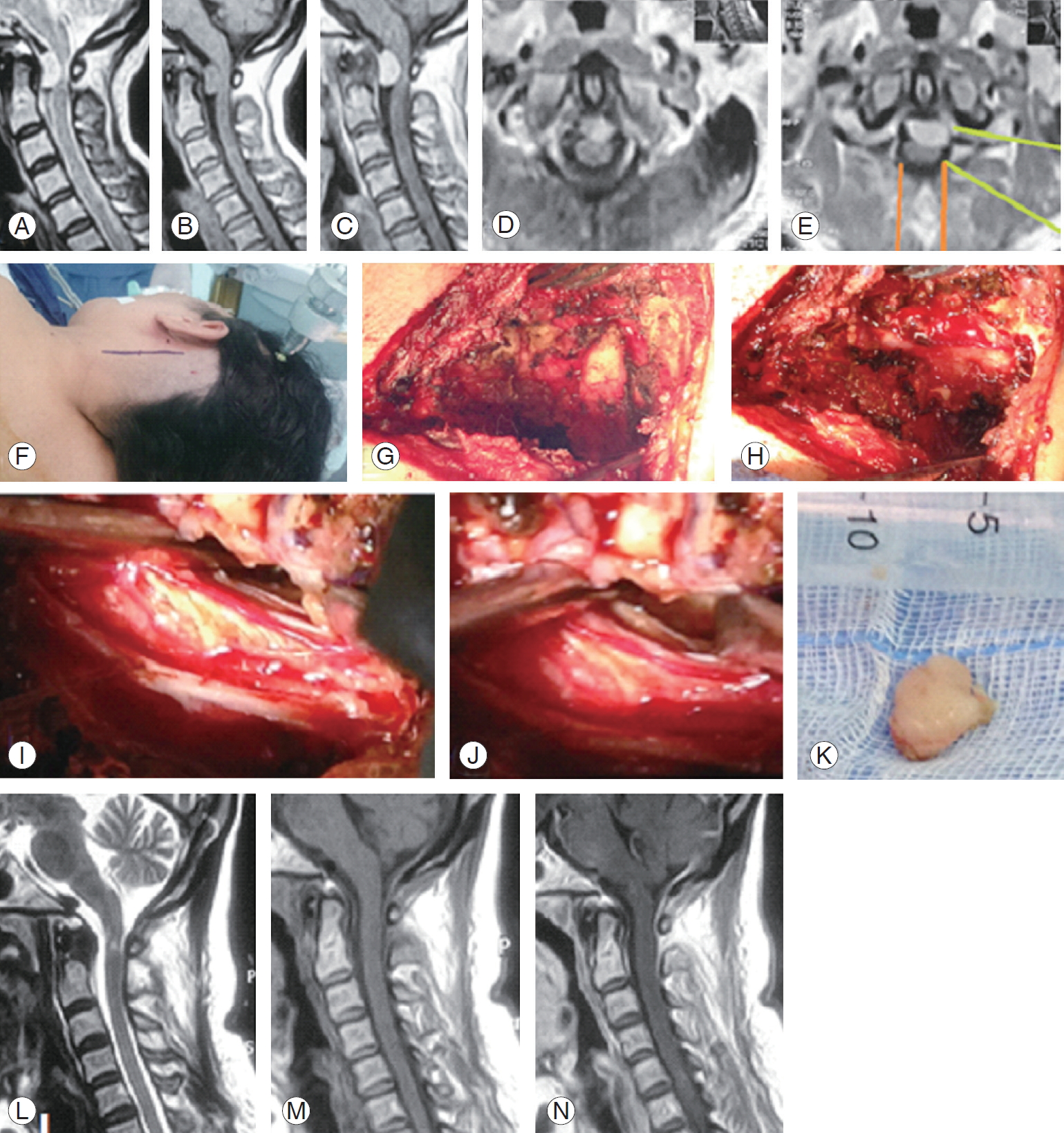
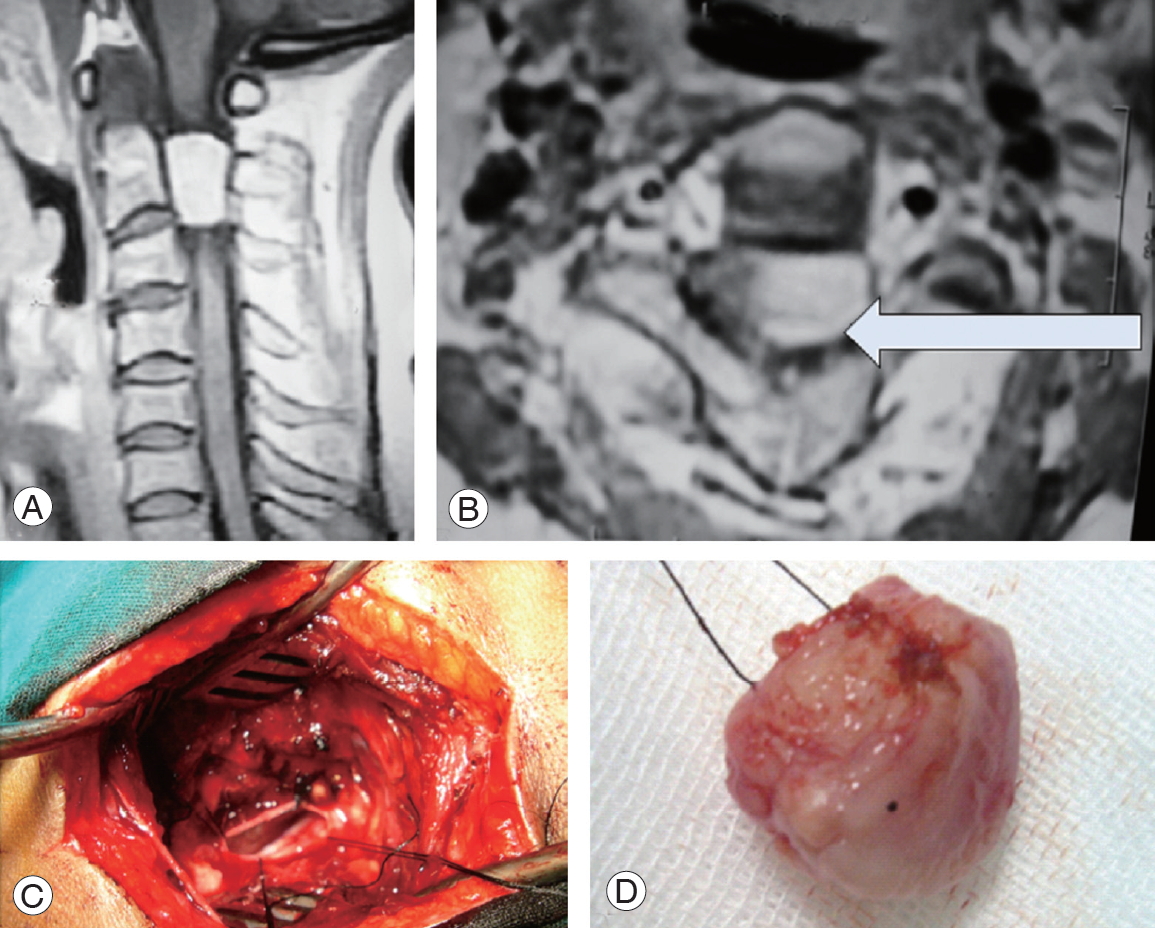
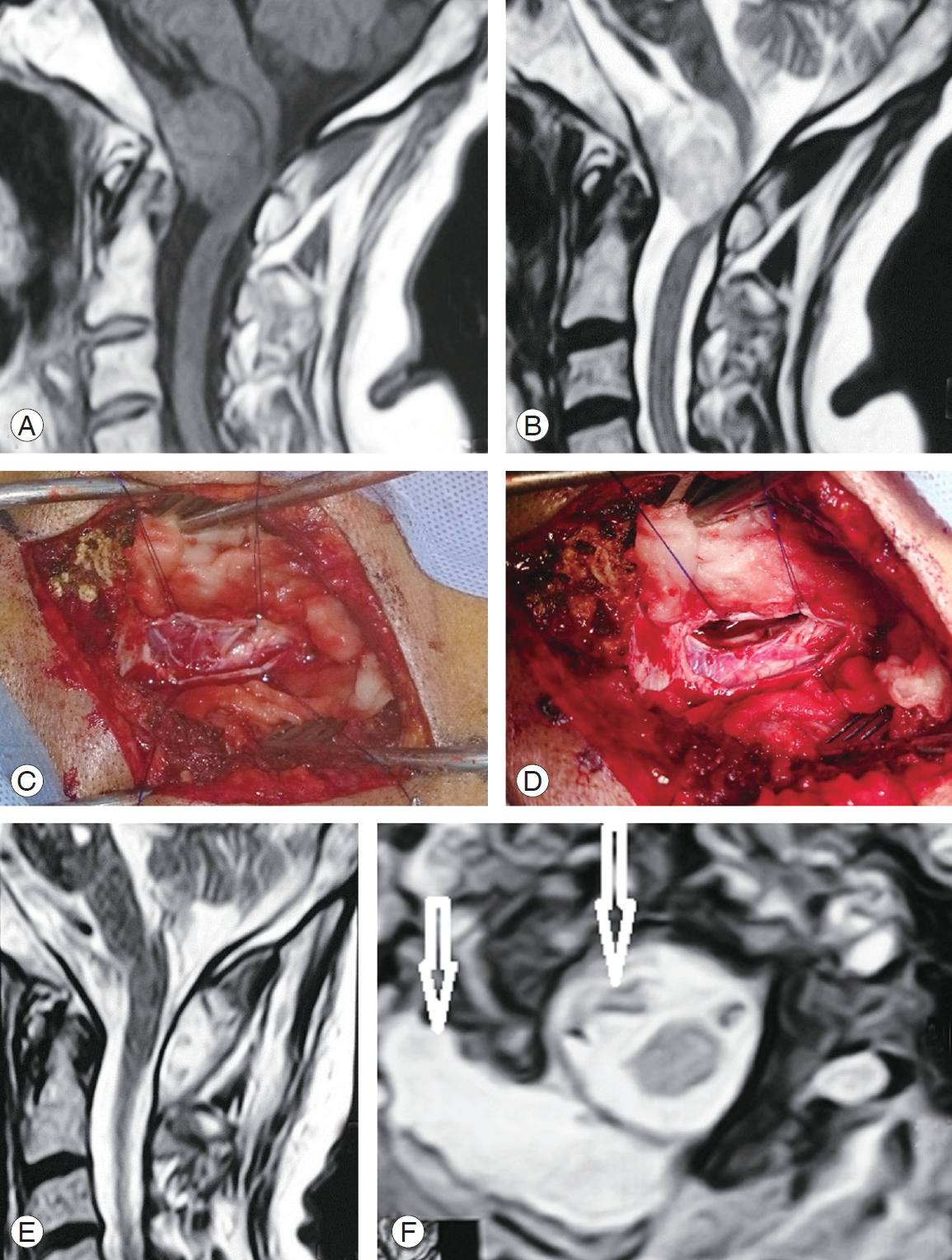
Tumor debulking was performed using a combination of thermal bipolar coagulation, rongeurs, curettes, and ultrasonic aspirator. In the case of some meningiomas, the lesion was easily suckable through the suction apparatus. Internal tumor cavitation of the mass allows tumor mobilization with limited cord traction. Neurophysiological monitoring, when available, was essential for safe complete mass removal and prevention of neurological deficit [4]. This facility was available only in the final three patients. If the tumor was not big enough, we used bipolar cauterization in the plan between the dura and tumor; thus, the tumor was de-vascularized and removed it as one piece (Figs. 3, 4). The dural base needed to be cleaned and/or coagulated with bipolar at the end of each procedure. On two occasions, a small piece of the tumor was attached to the ipsilateral intradural vertebral artery and cauterized using bipolar and left in situ (Fig. 5).
Adequate hemostasis was ensured, water-tight closure of the dura was performed, and an epidural closed drainage system was inserted; its track is designed through muscle and skin away from the deep facial suture line. The wound was meticulously closed in layers obliterating any dead space, and sterile drape was applied. The drain was removed after 24 hours if there was no cerebrospinal fluid (CSF) leakage in the drain. If CSF came out through the drain, it was left in situ until the CSF stopped or left for a week and then removed. Parenteral third generation cephalosporins were continued for 3 days perioperatively. Patients were discharged from the hospital after drain removal and scheduled for outpatient clinic visits.
All the patients were followed up routinely and regularly at the outpatient clinic for 12 months. Postoperative MRI with gadolinium enhancement was performed for all patients to ensure completeness of tumor excision.
2. Statistical analyses
The IBM SPSS statistical software program ver. 25.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis of the study data. The outcome descriptive data are presented as mean, standard deviation, and range values. Kolmogorov-Smirnov test was performed to prove data to be parametric. For comparison of pre-post data, paired t-test was used. For comparison between the data groups, independent samples t-test was used. A chi-square test was used to compare the proportions and prove associations between variables. Univariate and multivariate testing were used to check the associations between different variables. Spearman correlation coefficients were calculated among the variables. A p-value <0.05 was considered to indicate statistical significance.
Results
The far-lateral approach was used in 23 ventral and ventrolateral upper cervical meningiomas. In all our patients, the lateral approach was conducted smoothly and provided excellent exposure and good access that enabled effective tumor resection. All the patients had soft operative and postoperative course without significant adverse events. Operatively documented total tumor removal was achieved in 21 patients and subtotal in two where a small tumor portion was left attached to the intradural vertebral artery and was cauterized in situ with bipolar. This was documented in the postoperative MRI that was performed for all patients (Fig. 5). The mean operative time was 135±40 minutes (range, 110–380 minutes, while the mean operative blood loss was 450±210 mL (range, 200–850 mL), and the mean hospital stay was 4.3±2.2 days (range, 2–7 days) (Table 1).
Histopathological results revealed that psammomatous meningiomas were reported in 16 patients (69.6%), fibroblastic meningiomas in five patients (21.7%), and meningothelial meningiomas in two patients (8.7%).
At the final follow-up that was conducted at 27.6±21 months (range, 12–60 months) and according to the JOA score; 16 patients were classified into grade 0 (normal, 16–17) and seven into grade II (12–15) (Fig. 1). Root pain also improved in all five patients with preoperative radiculopathy and urinary precipitancy, while gait disturbance improved remarkably in eight patients (53%) and moderately in seven patients (47%). One patient showed asymptomatic local tumor recurrence 3 years after the surgery on routine MRI imaging and refused further surgery, while preferring to undergo follow-up.
Univariate and multivariate analyses showed that there were no significant associations of clinical outcome with tumor severity, pathological subtype of the tumor, duration of symptoms, age, and sex. Moreover, there were no significant associations of tumor resection completeness with the tumor level, tumor pathological subtype, or tumor topography (ventral or ventrolateral). Spearman correlation showed no statistically significant correlations among the study variables.
In four patients, the drain was left in situ because of CSF leakage into the drain for 5–7 days; thereafter, the drain was removed. One patient experienced superficial wound infection that was treated with frequent dressing and parental antibiotics for 1 week. Another patient experienced DVT that was treated with anticoagulants and followed up with our hospital vascular outpatient clinic as well. There was no reported neurological deterioration or other reported morbidity or mortality.
Discussion
Ventral and ventrolateral meningiomas of the upper cervical spine and foramen magnum pose a challenge to surgeons treating these lesions. The surgical removal of these lesions through the standard posterior midline approach involves a high risk of morbidities, and total resection is not possible in certain patients [9]. The far-lateral approach provides an alternate safe access that allows adequate exposure and gross total resection in these ventral and ventrolateral meningiomas of the upper cervical cord and brain stem [19].
Upper cervical meningiomas and foramen magnum are common neoplasms. Foramen magnum meningiomas represent 3% [3], high-cervical lesions represent 27% (n=9), and low-cervico-thoracic lesions represent 73% (n=24) of all spinal meningioma cases [2].
In 1988, George et al. [23] introduced and described the far-lateral approach for tumors anterior to the foramen magnum, a technique similar to that described by Heros [24] for the treatment of vertebral and vertebrobasilar lesions. The far-lateral approach and its variations have become a standard technique for many surgeons dealing with the foramen magnum and upper cervical lesions [12].
This retrospective clinical cohort study reports on 23 patients with upper cervical meningiomas from C4 up to the foramen magnum. The mean patient age was 57 years, with 74% of the patients being women. All patients were operated using the far-lateral approach. The far-lateral approach is a unique and fairly recent approach that is not commonly used in comparison to the standard posterior midline approach. It has been assumed that this technique is safe and effective, especially for ventral and ventrolateral cervical meningiomas. Our experience and results in these patients advocate the safety and efficacy of this technique.
1. Cervical meningiomas characteristics
In this series, the mean patient age was 57±15 years (range, 41–66 years). Other series have reported similar figures with mean ages of 63, 60, and 55.6 years, respectively [2,25,26]. In our series, 74% of the patients were women, and 26% were men. Similar sex distribution has been reported previously [2,25,26]. The mean duration of preoperative symptoms in this series was 13±10 months, and the mean duration of symptoms was 10.3 months in a previous trial [26].
2. Posterior versus anterior technique
Since several decades, the standard posterior midline approach has been practiced with reasonable safety and good clinical outcomes. Although posterior or posterolateral meningiomas can be safely and effectively resected using the standard posterior midline approach, the optimal approach for ventral or ventrolateral meningiomas remains controversial. Resection of these meningiomas could result in significant spinal cord or brain stem retraction, inadequate access and exposure, high rate of incomplete resection, and high morbidity [19,26]. Many authors have reported that patients operated via the standard posterior midline approaches showed worse clinical outcomes [14,27]. Goel et al. [28] reported what was contradicting that, when he reported gross total removal of 14 out of 17 ventral or ventrolateral meningiomas with similar results to other authors.
3. Some technical details
A key point of the far-lateral approach is the manipulation of the vertebral artery. Our approach is a modification of the trans-facetal variation proposed by Salas et al. [12], while we used the retro-facet approach. Our surgical corridor or access for the intradural lesion was a laminotomy between the fact joints anteriorly and the base of the corresponding spinous processes posteriorly. This approach was designed only for intradural tumors; where, in these lesions, there is no need to drill the facets or the condyles. In extradural lesions with bony involvement, it is mandatory to mobilize the vertebral artery and hinge it anteriorly to achieve complete tumor resection.
In our series, tumor topography and relation to the spinal cord were the major determinants of the surgical access; 30.4% (n=7) were ventral, and 69.6% (n=16) were ventrolateral. Slin’ko and Al-Qashqish [25] reported 24% ventral lesions and 76% ventrolateral; they used different approaches in their series, including dorsal, dorsolateral, and ventrolateral, depending on the tumor severity and topography. Tey also reported that the clinical outcome in patients with ventral lesions was worse than in those with ventrolateral lesions. Similarly, Schaller [2] reported ventral tumor position in six patients (18%), ventrolateral in 19 (58%), and posterior in 8 (24%).
According to our technique, and in agreement with Joaquim et al. [6] who proposed a technique of cutting the dentate ligaments and mobilizing the spinal cord to protect against neurologic injury and reported no neurologic deterioration in their technique demonstration. Dentate ligaments cutting relaxes the spinal cord, facilitates spinal cord and spinal roots manipulation, and prevents cord traction and root tension during tumor resection.
The histopathological subtype plays an important role in the ease of performing the procedure because the meningothelial lesion was easily suckable and could be removed easily with the suction nozzle, while the psammomatous lesion was tough, hard, and fibrotic that necessitated the use of ultrasonic aspiration for safe and complete tumor resection.
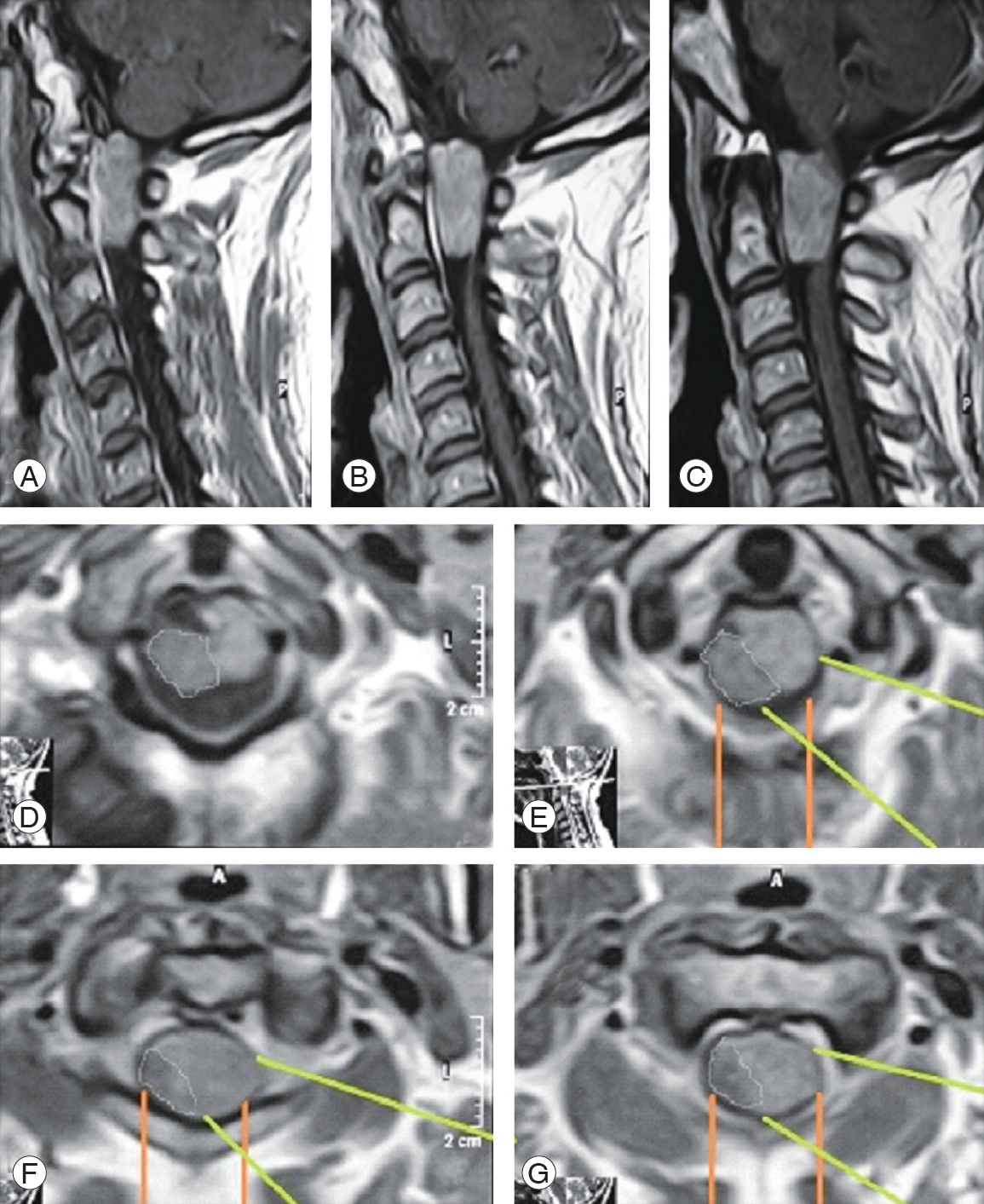
If we look critically at the MRI images of these ventral and ventrolateral meningiomas, we can see that the axis of vision of the surgeon as well as the surgical access and the working corridor for these tumors are more direct in the lateral approach (Figs. 6, 7; white and green lines). Moreover, in the posterior approach, the surgeon would work indirectly on a big part of the tumor (Figs. 6, 7; yellow and orange lines). These images clearly demonstrate the advantages of the visual axis and surgical corridor of the lateral approach that would be disadvantageous with the posterior approach. This significantly affects the safety of this procedure and the ability to remove such ventrally located lesions entirely.
4. Histopathology
Histopathological results revealed that psammomatous meningiomas were reported in 16 patients (69.6%), fibroblastic meningiomas in five patients (21.7%), and meningothelial meningiomas in two patients (8.7%). Similar reports (66%, 22%, and 11%, respectively) have been documented previously [2], while other studies have reported contradictory findings [3,10,19,20,25,26], which reported the meningothelial subtype as the most common in 49%, 90%, 56%, 39%, and 55%, respectively. The analysis of our reported data and that reported by others has shown that the histopathological subtypes did not influence the clinical or radiological outcomes [3,26,29].
5. Clinical and radiological outcomes
According to the JOA score, 70% of our patients recovered completely, 30% showed reduction in their preoperative symptoms, and none of them showed worsening of the condition. Flores et al. [26] reported full recovery of preoperative neurology in 73% of his patients. Slin’ko and Al-Qashqish [25] conducted a 39-month follow-up study and reported full recovery in 70 patients (50%), improvement in 53 patients (38%), no change in 10 patients (7%), and neurological deterioration in seven patients (5%). In his series, Schaller [2] reported that preoperative neurological deficits resolved in 79% (n=26) and deteriorated in 21% (n=7). Further, he added that all the latter had meningiomas of the psammomatous type. He stressed that surgery of spinal psammomatous meningiomas was associated with a less favorable outcome than surgery of other pathological subtypes [2]. In contrast, Arnautovic et al. [3] reported that the pathological subtype did not influence the clinical outcome; however, the meningothelial subtype was associated with most of the gross total removal cases.
Some studies have reported good prognostic outcomes with the following factors: posterior or lateral tumor position in the spinal canal, location below C4, age <60 years, duration of preoperative symptoms, total tumor resection, adequate access and exposure, no cord traction, and microsurgical technique [2,25]. One other important factor was that the general outcome and recovery was associated with the date of each reported series; thus, more recent the series, better the patient outcome. This reflects the improvement in facilities as well as the experience of the involved team.
Gross total removal was achieved in 91% of our patients; this was achieved in 85.7%, 67% by others [3,26]. Total tumor resection was achieved via different posterior approaches in 74% of the patients in an earlier trial [25]. We found no impact of the histological subtypes on tumor resection or clinical outcome, as reported by others [26,29].
A literature review showed that the general outcome was better with the lateral approach as compared to that with the standard posterior midline approach [3,6,7,25,30]. This difference was related to the group of patients with ventral and ventrolateral meningiomas who have been treated with the posterior approach.
6. Morbidity
We had no case of postoperative neurological deterioration in this series; however, previous studies have reported a prevalence of 7% and 3% [25,26]. The first series used different surgical approaches; this explains the increased morbidity with posterior approaches [25].
We reported four patients with continuous CSF collection into the drain who responded with time and conservative measures. This was reported in another lateral approach as CSF collection in one patient out of 10 responded to conservative measures [17], CSF leakage in three patients out of 30 responded to temporary external drainage [26], CSF leak in two of six with controlled well [27], they attributed this leakage to excessive dural cauterization to control bleeding during the procedure. Meanwhile, one study that employed the posterior approach reported that only one of 18 patients had CSF leakage [7].
We reported only one case with recurrence at postoperative 3 years. Studies that have used the lateral approaches reported no recurrence at the 5-year follow-up [26,30]. In our series, we did not report any postoperative lower cranial nerve palsy in any patient. This was reported in many other studies, especially those that reported on lesions at the foramen magnum [3,9,26].
7. Adjuvant therapy
Fortunately, all our meningiomas were World Health Organization grade I, and only in two patients, a very small piece of the tumor was left attached to the vertebral artery and cauterized in situ. Thus, there was no need for adjuvant therapy. Fractionated stereotactic radiosurgery (CyberKnife; Accuray Inc., Sunnyvale, CA, USA) adjuvant therapy was used by Flores et al. [26] on one occasion with successful local tumor control. Adjuvant stereotactic radiosurgery should be considered in patients with residual or growing residual tumors or if reoperation carries a high rate of morbidity.