Introduction
Computer-assisted navigation has been widely adopted in spinal surgery because of its ability to aid in visualization, especially in complex spinal cases. Over the past three decades, advancements in technology have resulted in improved outcomes in orthopedic oncology, total knee arthroplasty, total hip arthroplasty, trauma surgery, and spinal surgery [1]. With the continuous increase in healthcare costs in the United States, efforts have been devoted to analyzing the effectiveness and value of novel technologies [2].
Approximately 1.62 million spinal procedures are performed in the United States each year, and this number is predicted to gradually increase over the next decades [3–5]. For example, thoracolumbar fusion procedures had a 63% increase in prevalence from 2004 to 2015 [4]. Similarly, the rate of cervical fusion procedure increased from 23.7 to 50.6 per 100,000 population from 1997 to 2012 [5]. Cervical and thoracolumbar spinal procedures are expected to increase over the next 2 decades [4,5]. Therefore, trends in the costs and utilization of technologies during these procedures, specifically computer-assisted navigation, should be assessed because of the rise in the number of thoracolumbar and cervical surgical cases coupled with the increasing concern over costs and resource utilization in healthcare [6].
Previous studies explored the application of computer-assisted navigation in orthopedics and analyzed its impact on patient outcomes in specific orthopedic subspecialties [7,8]. Some prior studies claimed that computer-assisted navigation in orthopedic surgery has gained increased acceptance in practice in recent years [7], but studies have yet to examine the trends associated with the utilization of computer-assisted navigation for cervical and thoracolumbar spinal surgery on a broader scale via a national-level database. In the present study, computer-assisted navigation procedures involve stereotactic navigation through computed tomography or fluoroscopic images to provide a projection of a patient’s anatomy (Fig. 1). This procedure provides insights into complex anatomy that will help surgeons better navigate previously hard-to-visualize areas. Some commonly used systems include Medtronic O-arm, StealthStation, Iso-C C-arm, and NaviVision [9]. Given the increased adoption of computer-assisted navigation for spinal surgery in the past decade, this study aims to assess the trends in the cost and utilization of computer-assisted navigation in cervical and thoracolumbar spinal surgery to better inform the surgeons of changes in practice.
Materials and Methods
1. Study population
Data recorded in 2015–2018 in the National Readmission Database (NRD), which contains data from approximately 18 million discharges in the United States every year, were retrospectively analyzed. In particular, data from 28 geographically dispersed states were collected, accounting for 58.7% of all the US hospitalizations. With the NRD, readmissions can be examined regardless of the expected payer type. However, the Healthcare Cost and Utilization Project (HCUP) Data Use Agreement forbids the reporting of frequencies fewer than 11 to account for healthcare privacy concerns when this database is used.
The International Classification of Diseases 10th revision (ICD-10) codes were implemented in the 3rd quarter of 2015. The ICD-9 and ICD-10 codes were utilized for the 2015 dataset because of the change in the 3rd quarter, and the ICD-10 codes were solely used for 2016–2018 datasets. The sampling weights provided by HCUP were used to adjust the analysis for all discharges in the United States. The institutional review board exemption was obtained from our institution for this study. The requirement for informed consent from individual patients was omitted because of the retrospective design of this study.
2. Inclusion and exclusion criteria
All the patients who underwent cervical and thoracolumbar spinal surgery with the aid of computer-assisted navigation were identified using ICD-9 and ICD-10 procedure codes. Of these patients, those who underwent elective and nonelective procedures were kept for subgroup analysis. Table 1 provides a list of all the ICD codes utilized in this study.
3. Patient characteristics
Patient characteristics, including demographic information (sex and age), diagnoses, and health insurance payer type, were obtained from the NRD.
Preoperative comorbidities were also identified using ICD-9 and ICD-10 via the R comorbidity package, which is utilized to calculate Charlson and Elixhauser comorbidity scores. Each value within R comorbidity corresponds to a particular preexisting medical condition identified in either the Charlson or Elixhauser index. Charlson and Elixhauser indices are two of the most well-known and utilized metrics of predicting patient outcome because of specific comorbidities. For the Charlson comorbidity index, which was developed by Charlson et al. [10], 17 comorbidities and their respective weights were included. A given patient’s comorbidities were then factored in to estimate the mortality risk. The same procedure was performed with the Elixhauser comorbidity index; however, Elixhauser et al. [11] defined 30 comorbidities for utilization [12].
4. Hospital costs
Patients’ total charges, which are reported by the NRD and adjusted for inflation by using the consumer price index, were analyzed.
5. Statistical analysis
Data were statistically analyzed using SciPy ver. 1.6.1 (https://scipy.org/). The association between time and the number of patients receiving spinal surgery with computer-assisted navigation, the total charges of patients, and the ratio of patients with Medicare to patients with private insurance were examined through linear regression analysis.
Results
1. Patients’ characteristics: cervical
A total of 48,116 cervical spine cases were included: 1,880 in 2015, 10,999 in 2016, 16,790 in 2017, and 18,447 in 2018 (Pearson correlation coefficient=0.756, p=0.049) (Table 2, Supplement 1).
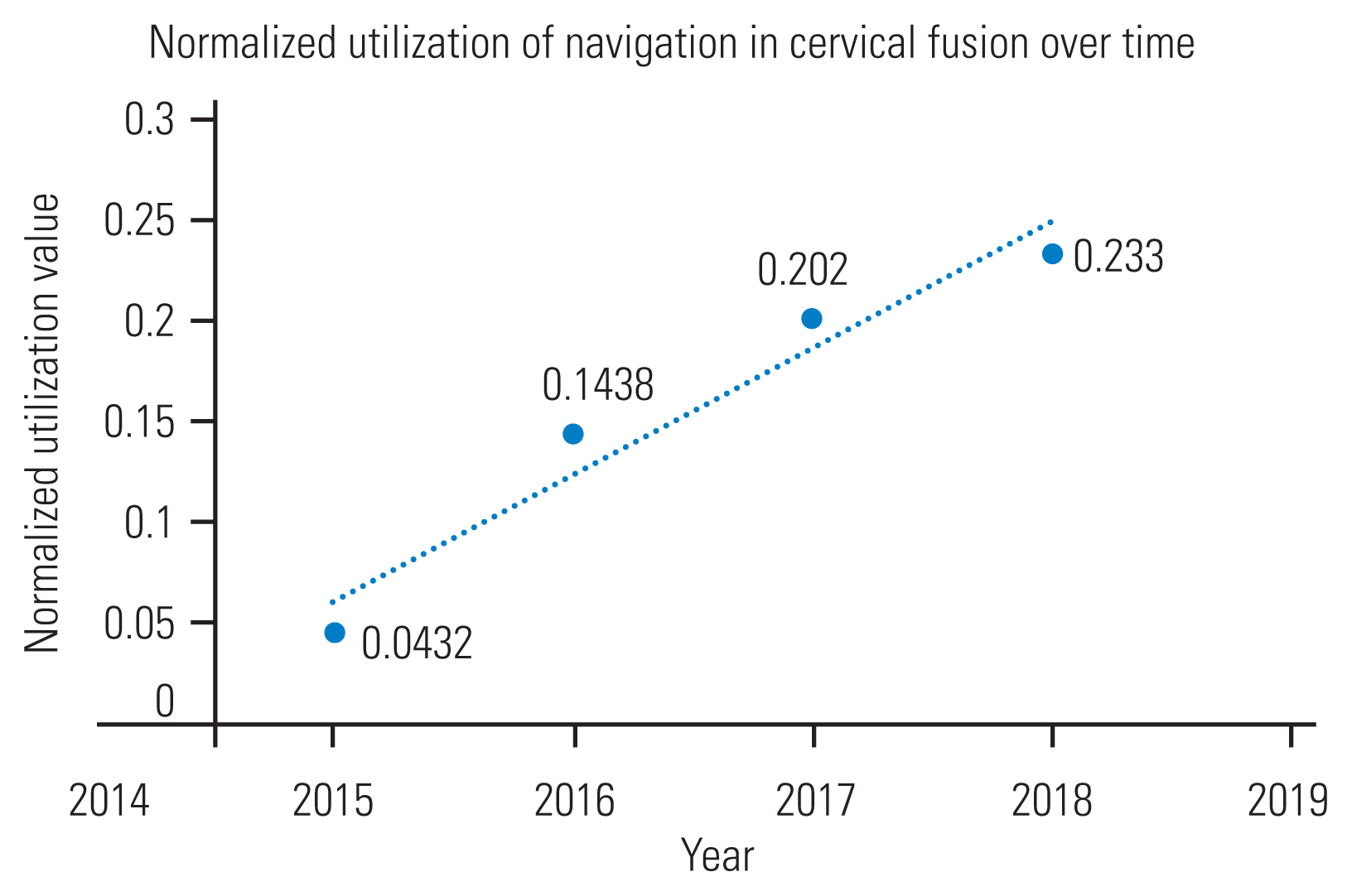
The cases that utilized computer-aided navigation were normalized to the total number of cervical cases in each respective year to account for the potentially increasing number of cervical cases through the years. The proportions from 2015 to 2018 were 0.0432, 0.1438, 0.202, and 0.233, respectively (Pearson correlation coefficient=0.970, p=0.030) (Fig. 2).
2. Patient characteristics: thoracolumbar
A total of 27,093 thoracolumbar cases were included: 2,169 in 2015, 5,171 in 2016, 9,045 in 2017, and 10,708 in 2018 (Pearson correlation coefficient=0.9895, p=0.010) (Table 2, Supplement 2).
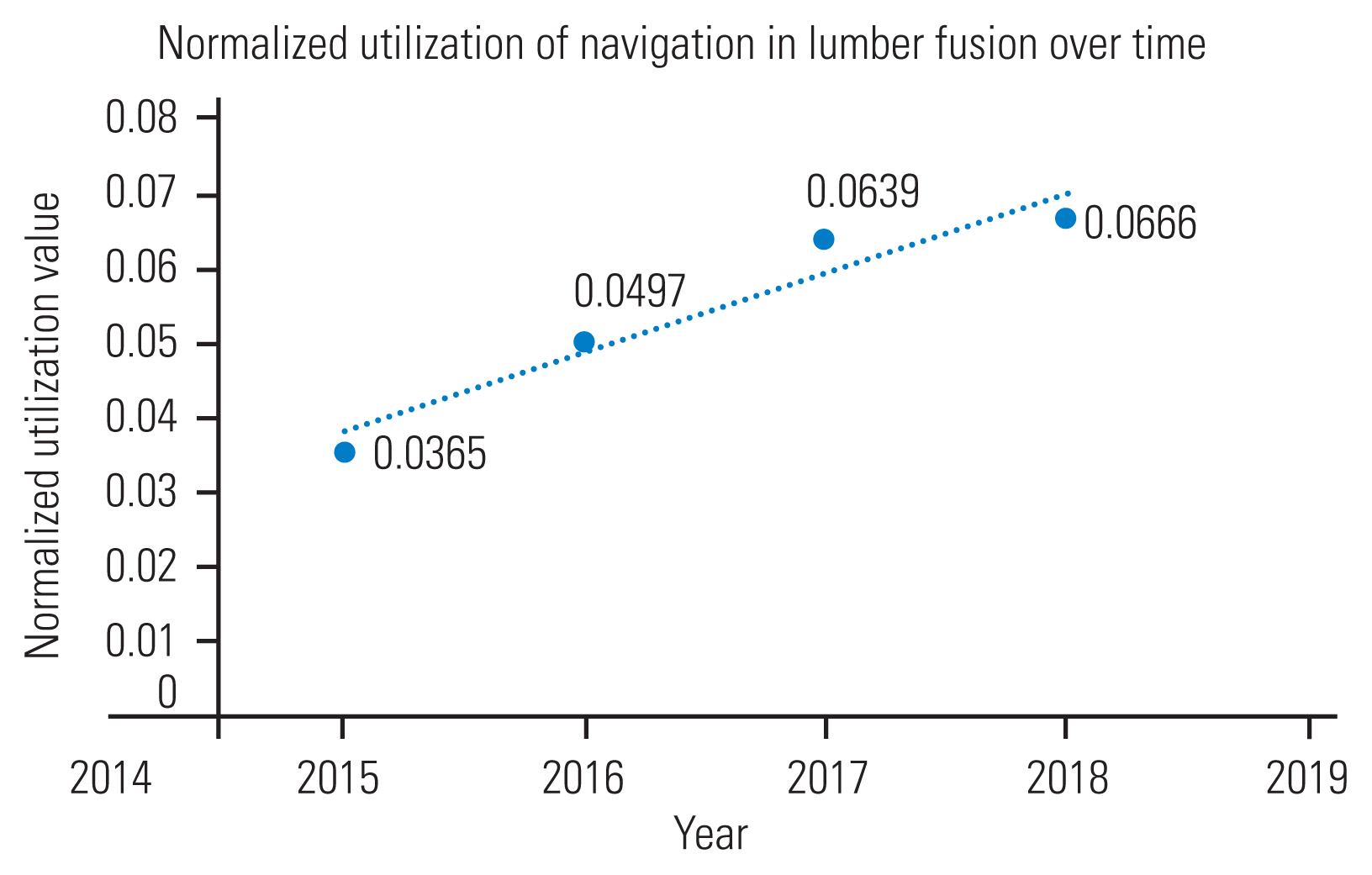
The cases that utilized computer-aided navigation were normalized to the total number of thoracolumbar cases in each respective year to account for the potentially increasing number of thoracolumbar cases through the years. The proportions in 2015, 2016, 2017, and 2018 were 0.0365, 0.0497, 0.0639, and 0.0666, respectively (Pearson correlation coefficient=0.969, p=0.031) (Fig. 3).
3. Patient characteristics: comorbidities
Of the patients who underwent cervical surgery with the use of navigation in 2015, 8.56% had 3+ Charlson comorbidities, and 14.0% of those that did not involve navigation had 3+ comorbidities. In 2018, 22.5% of patients who underwent cervical navigation surgery had 3+ comorbidities, whereas 13.2% who had surgery without navigation had 3+ comorbidities. For patients who had thoracolumbar navigation, 3.92% had 3+ comorbidities in 2015, and 15.1% who did not undergo the procedure with navigation had 3+ comorbidities in that same year. In 2018, 8.24% of patients with thoracolumbar navigation had 3+ comorbidities, and 11.7% of patients with nonnavigation had 3+ comorbidities (Table 3).
4. Total hospital costs and Medicare ratio: cervical
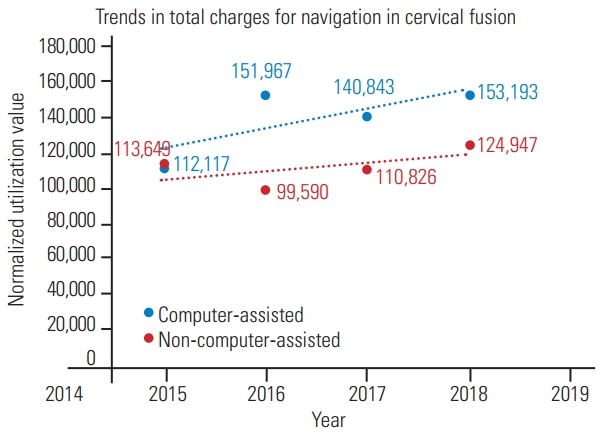
The average total charges of patients who received computer-assisted navigation during cervical fusion surgery in 2015, 2016, 2017, and 2018 were $112,117, $151,967, $140,843, and $153,193, respectively, after adjustments for inflation were made (Pearson correlation coefficient=0.758, p=0.242). These values were compared with the average total charges for nonnavigated cervical cases (2015, $113,649; 2016, $99,590; 2017, $110,826; and 2018, $124,947). The average charges for nonnavigated cases were grossly and significantly (p=0.046) lower than those for navigated cases (Fig. 4). The ratios of patients with Medicare to those with private insurance were 0.949 and 0.868 in 2015 and 2018, respectively.
5. Total hospital costs and Medicare ratio: thoracolumbar
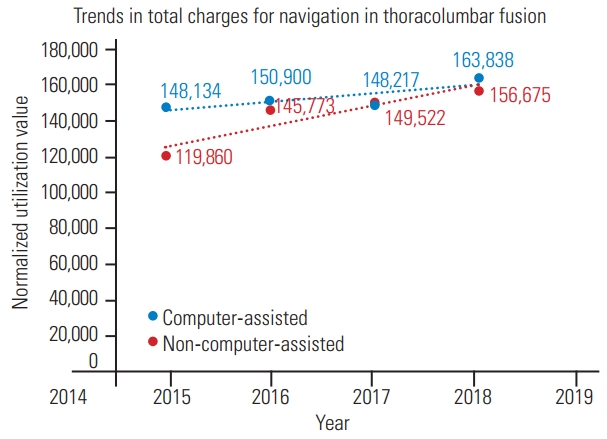
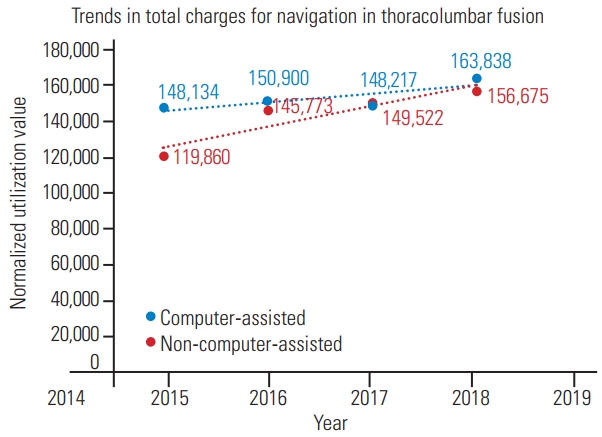
The average total charges of patients who received computer-assisted navigation during thoracolumbar fusion surgery in 2015, 2016, 2017, and 2018 were $148,134, $150,900, $148,217, and $163,838, respectively (Pearson correlation coefficient=0.766, p=0.234). These values were compared with the average total charges for nonnavigated thoracolumbar fusion cases (2015, $119,860; 2016, $145,773; 2017, $149,522; and 2018, $156,675). The average charges for nonnavigated cases were overall grossly but not significantly (p=0.31) lower than the charges for navigated cases (Fig. 5). The ratio of patients with Medicare to those with private insurance increased from 1.17 in 2015 to 1.36 in 2018.
Discussion
New technologies often emerge in the healthcare industry primarily to improve patient outcomes. They are accessible, cost effective, and accurate. For instance, computer-assisted navigation, a technological system invented in the early 1990s and first applied in orthopedics in 1997, has the potential to improve surgical outcomes by helping surgeons with navigational planning and procedural reproducibility [1,12]. Our study found a consistent increase in utilization from 2015 to 2018. Cervical and thoracolumbar cases with navigation significantly increased and remained significant even after normalization was made for the total number of fusion cases in each year. This finding indicated that the adoption of computer-assisted navigation utilization increased from 2015 to 2018. The associated total charges for cervical and thoracolumbar spinal surgery also increased during this period even when adjustments were made for inflation. However, neither thoracolumbar cases nor cervical cases had a significant increase in total charges. The average charges for the cases that utilized computer-assisted navigation were compared with those for noncomputer navigated cervical and thoracolumbar spinal surgery cases to reveal a potential increase in the cost burden of patients. The number of navigation-aided cases was consistently higher than that of nonnavigation cases. This difference was statistically significant for cervical cases but not for thoracolumbar cases. Therefore, cervical fusions utilizing navigation might cause an additional cost burden to patients.
As the utilization of navigation in cervical and thoracolumbar spine surgeries grows, the cost of care for more patients likely increases because of the utilization of a more advanced technology. Computer-assisted navigation has been proven to be more expensive than traditional methods when it is used intraoperatively in some orthopedic surgery types, such as total knee arthroplasty [12]. In the case of cervical and thoracolumbar spinal surgery, our evidence showed that the total charges for patients generally increased from 2015 to 2018. Our comparison of nonnavigated costs over time highlighted a potentially increasing cost burden specific to computer-assisted navigation in spinal surgery. As such, the possible rising cost burden coupled with an increased implementation of this technology should be further analyzed to determine the effectiveness of computer-assisted navigation in improving patient care and surgeon capabilities. With spinal surgeries under recent criticisms for their associated cost for patients [13], trends in the total charges of computer-aided navigation-utilizing procedures over time should be examined to predict the effect of this technology on the industry in the future. The computer-aided navigation charges over time observed in this study increased, so the perceived benefit of this technology to a surgeon’s performance and patient outcomes in cervical and thoracolumbar spine procedures should be explored. Previous studies claimed that the use of computer-aided navigation can improve the accuracy of pedicle screw placement in thoracic spinal surgery; however, future studies should explore the effect of navigation on patient outcomes [14,15].
Indications for computer-aided navigation utilization during cervical surgery differ from those during thoracolumbar surgery. Although computer-aided navigation is more typically used in thoracolumbar surgery for three-dimensional visualization, minimally invasive surgery, and pedicle screw implementation [15,16], it is used less typically in cervical surgery to assist surgeons with instrumentation in patients with atypical spine anatomy [17]. Therefore, costs, utilization, and demographics varied among the cervical and thoracolumbar populations in this study.
The distribution of the age and gender of patients receiving computer-aided navigation for cervical and thoracolumbar fusion has not changed significantly over time. Additionally, the insurance coverage distribution has remained largely unchanged over time, and the number of thoracolumbar patients covered by Medicare has slightly increased compared with that of patients covered by private insurance. We hypothesized that this increase in the number of patients covered by Medicare for computer-aided navigation-utilized thoracolumbar surgeries was due to the more routine use of computer-aided navigation, specifically for thoracolumbar procedures. Computer-aided navigation has become commonly used for operating in the thoracolumbar region [8,16], so more of these cases are likely covered by Medicare plans. This finding might account for the increase in the thoracolumbar population and the lack of increase in the percentage of Medicare-covered patients among cervical cases.
Another notable large discrepancy between 2015 and 2018 was the readmission rate. For cervical cases utilizing computer-aided navigation, the rate of 90-day readmission increased substantially from 2.9% in 2015 to 27.0% in 2018. Computer-aided navigation is utilized in cervical cases involving typically complex spinal anatomy [17], such as C1–C2 deformity. Revision surgery readmission rates likely increased substantially from 2015 to 2018 because of the increased adoption of computer-aided navigation for complex cervical cases in patients with increased comorbidities. For cervical and thoracolumbar surgeries performed with computer-aided navigation, the percentage of patients who had higher Elixhauser and Charlson comorbidity scores (>3) increased between 2015 and 2018, indicating potentially more difficult and complex cases because of the higher likelihood of comorbidities (Table 3).
More specifically, the percentage of patients with 3+ comorbidities in the navigated cervical group over time substantially increased compared with that of the nonnavigated cervical group (13.94% versus –3.4%, respectively). This finding differed from the comparison between the thoracolumbar navigated and nonnavigated groups. In the thoracolumbar cases, the percentage difference over time in patients with 3+ comorbidities was more similar (4.32% versus –3.4%, respectively). This observation could explain the differences in the increased readmission rates over time in cervical navigated cases and thoracolumbar cases. Patients with higher Charlson comorbidity indices have a higher readmission risk of revision or associated medical complications, thus increasing the readmission rates of cervical cases over time. Similarly, the change in 90-day readmission rates of the navigated thoracolumbar cases increased between 2015 (4.0%) and 2018 (13.4%). However, this increase in percentage was lower than that of the cervical results.
The increased percentage of patients with higher Elixhauser and Charlson comorbidity scores in 2018 compared with that in 2015 led to an increase in the 90-day readmission rate in thoracolumbar fusion cases. Prior comorbidities were shown as independent predictors of readmission, so the higher comorbidity scores were a potential reason for higher readmission rates [18,19]. Likewise, Whitmore et al. [20] showed that the increasing Charlson comorbidity score is associated with a significantly higher risk of complications in patients undergoing spinal surgery. Moreover, the increase in readmissions and comorbidity scores likely contribute to the increase in charges for cervical and thoracolumbar navigation cases. Thus, the trend of increasing cost over time cannot be entirely attributed to the growing utilization of this new technology, that is, as comorbidities and readmissions increase, average charges potentially increase.
A notable trend in thoracolumbar and cervical cases in terms of the proportion of elective and nonelective procedures was observed. In comparison with the percentage in 2015, the percentage of elective cervical and thoracolumbar procedures in 2018 decreased; conversely, the percentage of nonelective procedures subsequently increased although these changes were much more dramatic for the cervical cases (Table 2). In other fields, nonelective cases are more associated with intraoperative complications and postoperative adverse outcomes [20]. Based on this hypothesis, an interpretation of our findings is that nonelective cases are overall more likely to be complicated from the start than elective procedures [21]. However, further studies should be conducted to elucidate this discrepancy. We also hypothesized that this trend of increasing proportion of nonelective cases could be associated with the increase in computer-assisted navigation utilization. As more surgeons become comfortable using this advanced technology in their operating room, they are potentially more likely to use it during atypical procedures, such as nonelective cases.
Although ICD-10 codes are specific to the use of computer-aided navigation in thoracolumbar or cervical spinal surgery, no ICD-9 codes specific to either type of procedures are established. As a result, the patient populations of NRD datasets that use ICD-9 codes (2015) should be estimated using ICD-9 codes for the general use of computer-aided navigation coupled with ICD-9 codes for either thoracolumbar or cervical spinal surgery. The low number of cervical cases that utilized computer-aided navigation from the NRD is partly attributed to coding estimation, that is, an ICD-9 code specific to cervical computer-aided navigation cases is unavailable; as such, we used a combination of computer-aided navigation-specific codes and cervical fusion surgery-specific codes. The 2015 data incorporated ICD-9 and ICD-10 codes because of the national coding alteration that occurred in October of that calendar year. This change in the coding system could contribute to the trends found in this analysis, so future studies should include data recorded in 2019 onward to confirm the continuation of the trends identified in this study. The number is low because most cervical cases (>80%) are anterior fusion cases [22,23], which are usually not subjected to computer-aided navigation because instrumentation in these procedures can normally be placed without aided visualization [7,22]. Additionally, this study found that the adoption of navigation in cervical cases was greater than that in thoracolumbar cases. This finding was likely due to the more complex anatomy of the cervical region, but this assumption could not be made because of the limitations of the NRD’s classification system for patient diagnosis. Future studies should focus on comparing prior diagnosis of the abnormal spinal anatomy between cervical and thoracolumbar navigated cases and their associated clinical outcomes and costs. We postulated that the utilization of navigation in spinal surgery will continue to increase over time as more surgeons are trained on computer-aided navigation. More data will have to be collected beyond 2018 to further assess utilization and total charge trends over the past 4 years and identify if they align with the results obtained in this study.
Conclusions
The prevalence of computer-aided navigation in cervical and thoracolumbar spinal surgery significantly increased from 2015 to 2018 even when the overall increase in cervical and thoracolumbar fusion cases was considered. This finding indicates that the proportion of these surgeries involving navigation increases. The use of these technologies is also associated with an increase in total charges for patients even when adjustments for inflation are made and when the cost trends of nonnavigated spinal cases are compared. Further research should be conducted to determine whether computer-aided navigation is necessary and cost effective for patients, especially when it is used for spinal procedures. With the advent and increased acceptance of computer-assisted technology and methods, appropriate analysis should be performed to ensure that the use of this technology indeed provides cost effective benefits to patients undergoing cervical and thoracolumbar spinal fusion surgeries.