Introduction
Lumbar spinal stenosis is a degenerative disease commonly seen in elderly individuals. Surgical intervention is commonly required for patients who fail conservative treatment. Minimally invasive spine surgery has become a research hotspot in the treatment of spinal degenerative diseases with the rapid development of technology in recent years [1]. An increasing number of minimally invasive surgery techniques and results have been reported. Microscopic decompression (MD) unilateral laminectomy and unilateral laminectomy for bilateral decompression are considered to be the routine methods of standard minimally invasive surgery for lumbar spinal stenosis [2ŌĆō4]. However, MD technology has some shortcomings, including poor visual field, difficult instrument operation, possible insufficient decompression, and longer operation time than other minimally invasive procedures [5ŌĆō10]. The prevalence of unilateral biportal endoscopic (UBE) technology, also known as biportal endoscopic spinal surgery (BESS), has made up for some of the deficiencies of MD technology. It uses two channels on the same side of the spine: one observation channel and one operation channel. It uses saline to continuously irrigate the deltoid space of the multifidus muscle to create a clear surgical field of vision. It can be completed with power drills and conventional open surgical instruments. Total spinal canal decompression surgery can be performed under a microscope [11]. UBE/BESS technology has been successfully applied to the treatment of degenerative spinal diseases and has been rapidly ŌĆ£revisedŌĆØ in recent years due to its wide field of vision, the large operating angle of the instruments, and the same operating habits as traditional open surgery [12,13]. However, the safety and effectiveness of the emerging UBE/BESS technology in the treatment of lumbar spinal stenosis remain controversial [14ŌĆō17].
For the first time, this study compared the area of dural sac expansion, the change in C-reactive protein (CRP) value, and the change in patient satisfaction (the modified MacNab score) with lumbar spinal stenosis after two surgical technology treatments compared with the previous meta-analysis [2,18]. The research sample size was increased, and the persuasiveness and credibility of the results were improved.
Methodology
PubMed, Web of Science, Embase and Cochrane Library, China National Knowledge Infrastructure, WanFang, and VIP databases were used to conduct a comprehensive search. Using subject terms, free words, and a combination of the two, the following search terms were used: ŌĆ£unilateral biportal endoscopy,ŌĆØ ŌĆ£biportal endoscopic spinal surgery,ŌĆØ ŌĆ£biportal endoscopic,ŌĆØ ŌĆ£spine endoscopy,ŌĆØ ŌĆ£microscopic decompression,ŌĆØ ŌĆ£minimally invasive spine,ŌĆØ and ŌĆ£lumbar canal stenosis.ŌĆØ The Boolean operations ŌĆ£ANDŌĆØ and ŌĆ£ORŌĆØ were used to search. English or Chinese was the language used, and the search time was from the establishment of the database to July 30, 2021. This study did not require Institutional Review Board approval and/or informed consent.
1. Inclusion and exclusion criteria
Studies were selected that satisfied the following inclusion criteria: (1) compared the clinical results and laminectomy and decompression efficacy alone in patients with lumbar spinal stenosis treated with UBE and MD techniques. (2) The comparison outcome had at least one of the following: clinical, surgical, and imaging-related parameters (pre- and postoperative Visual Analog Scale [VAS] for leg pain, Oswestry Disability Index [ODI] score, surgery time, blood loss, complications, hospital stay, etc.). (3) The full text could be obtained; complete and useful data could be extracted. The measurement data were expressed as averages┬▒standard deviation. Excluded studies were as follows: (1) case reports, review articles, published abstracts, studies involving fewer than 10 patients, and duplicate data and (2) articles with unavailable access to the full text.
2. Study selection
The research object was determined by reading the title and literature abstract according to two independent authors (L.J. and Y.J.). The full text was searched if a decision could not be made. Disagreements were resolved through consensus and discussion with a third party (Y.H.). A bias risk assessment was performed. The reason for nonconformity or exclusion of the study was recorded and described.
3. Data extraction
Relevant data were extracted by two independent investigators after intensive reading of the full text, mainly including the name of the first author, publication year, study type, sample size, average age, complications, outcome indicators, and follow-up time. Data were statistically tabulated. The third researcher participated in the discussion and made a decision through consultation if there was a disagreement. If necessary, the authors of the literature were contacted to clarify relevant information of the research.
4. Quality assessment
For randomized controlled trials, the evaluation quality refers to the standards recommended by the Cochrane system [19]. For nonrandomized controlled trials, the quality of the literature was evaluated according to the Risk of Bias Assessment of Non-randomized Studies (RoBANS) guidelines [20]. If the two investigators disagreed, they discussed and resolved the point of disagreement. If there were still differences, the third party joined the discussion and helped settle the disagreement.
5. Statistical analysis
Review Manager software ver. 5.3 (the Cochrane Collaboration, London, UK) was used to perform statistical analysis and the results are represented by forest diagrams. The heterogeneity test was performed when the data were merged. The fixed-effects model was adopted if there was no obvious heterogeneity between the data (I2Ōēż50%). The heterogeneity was analyzed if there was heterogeneity (I2>50%). A random-effects model was used if the heterogeneity could not be removed qualitatively. A funnel chart was used to analyze the publication bias of the literature if there were more than 10 studies included in a certain outcome index. The odds ratio was calculated for the binary variables and the relative risk was used as the effect scale. The mean difference was used for continuous variables. Different evaluation scales and large errors exist between the individual measured values and standardized mean difference combined statistics were selected if the numerical units are different. A p<0.05 indicates that the difference between the two groups is significant.
Results
1. Literature search
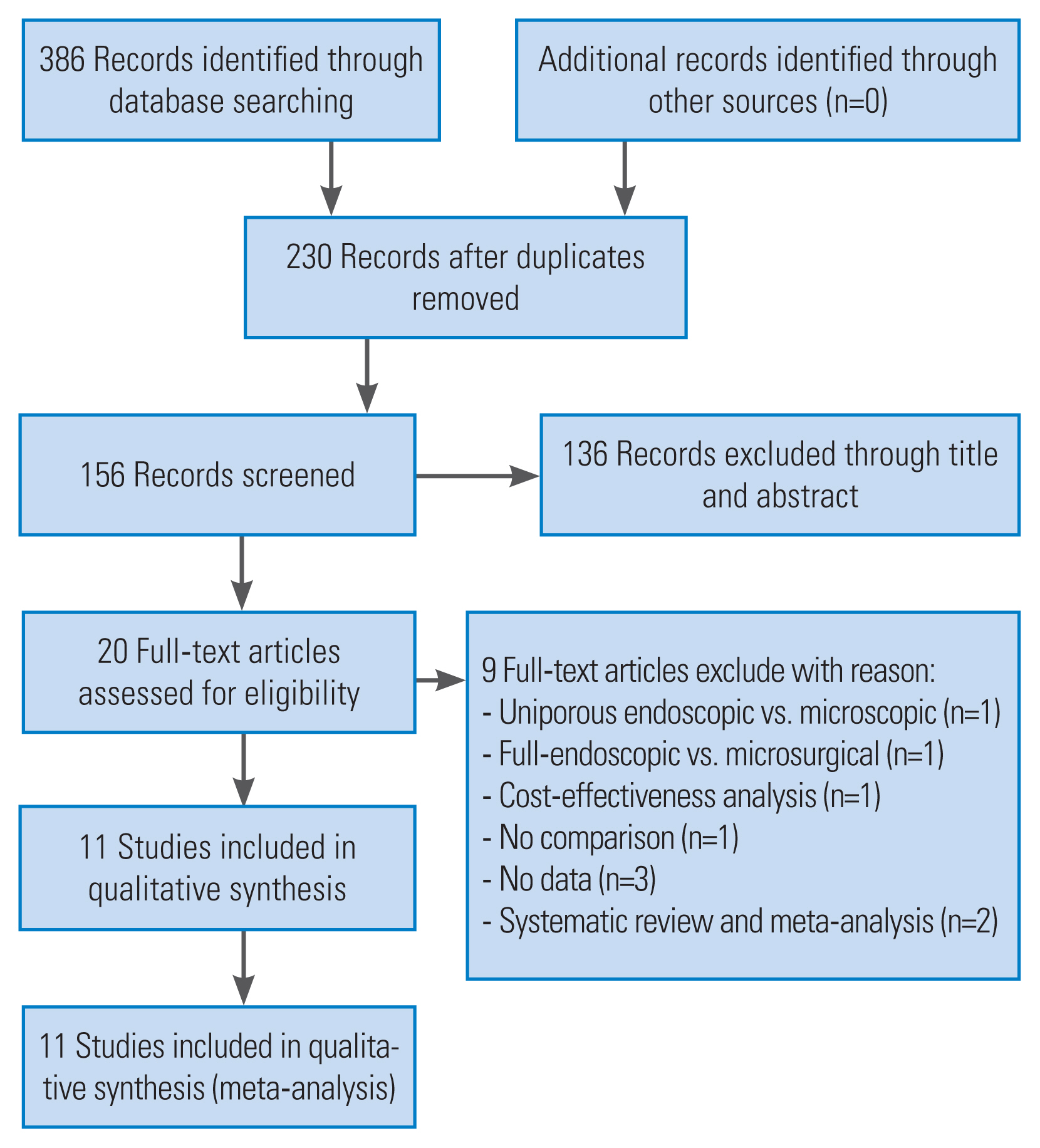
A total of 386 related documents were obtained through a preliminary search. Eleven articles were ultimately included [15,21ŌĆō30] (Fig. 1, Table 1) after rescreening by eliminating duplicate documents, reading titles and abstracts, and full text. There were 10 articles in English [15,21ŌĆō28,30] and one article in Chinese [29]. There were 930 patients, including 449 patients in UBE and 521 in MD.
2. Study characteristics and risk assessment
Only two of the included studies were randomized controlled trials [26,27] and the overall quality was moderate to high, according to the Cochrane system (Fig. 2). The remaining nine studies were nonrandomized controlled trials [15,21ŌĆō25,28ŌĆō30]. Risk assessment was conducted according to the RoBANS guidelines. Each study had a certain degree of bias. Table 2 shows the specific evaluation results.
3. Operation time
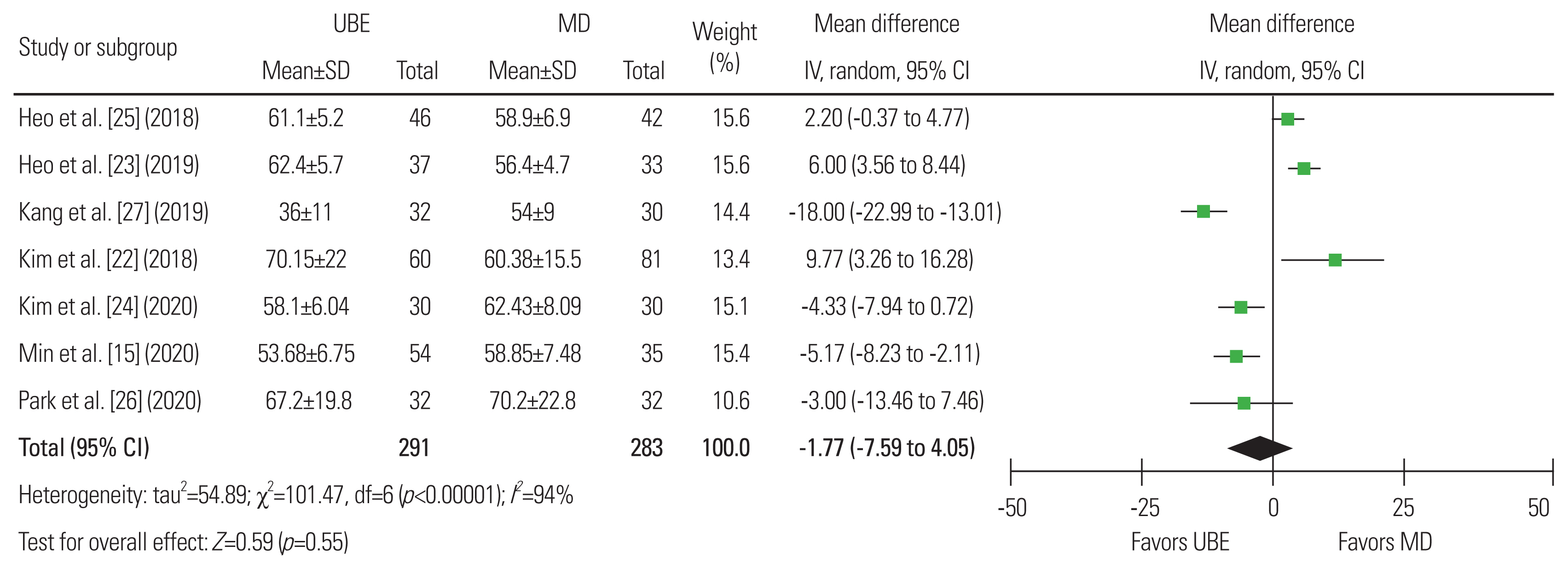
Seven studies were included to evaluate the operation time of the two surgery types with 291 patients in the UBE group and 283 in the MD group [15,22ŌĆō27]. There was statistical heterogeneity between the study groups (I2=94%). Thus, the random-effects model was used for statistical analysis and was grouped according to the different study types. There was no significant difference between the two (mean difference, ŌłÆ1.77; 95% CI, ŌłÆ7.59 to 4.05; p=0.55]. Therefore, in terms of operation time, a difference could not be identified between the two surgical methods (Fig. 3).
4. Blood loss
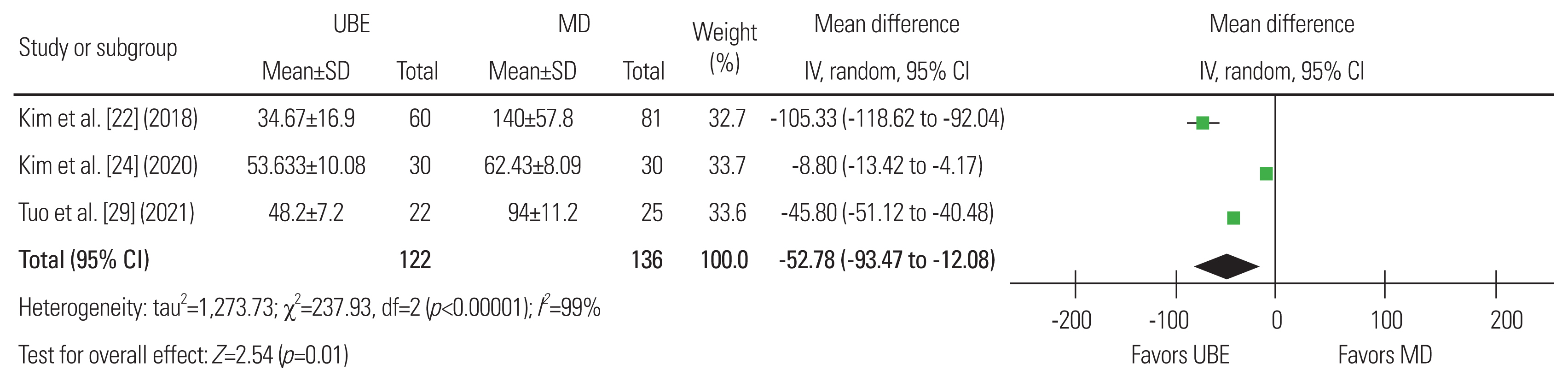
Three articles were included [22,24,29], with 112 patients in the UBE group and 136 in the MD group. The heterogeneity analysis showed significant heterogeneity (I2=99%) and a random-effects model was used. Results showed that blood loss was significantly different, favoring the UBE surgery group (p=0.01; mean difference, ŌłÆ52.78; 95% CI, ŌłÆ93.47 to ŌłÆ12.08). A mean difference of ŌłÆ52.78 mL (95% CI, ŌłÆ93.47 to ŌłÆ12.08 mL; p=0.01) concluding that UBE surgery results in less bleeding than MD surgery was revealed using these data for meta-analysis (Fig. 4).
5. Area of dural sac expansion
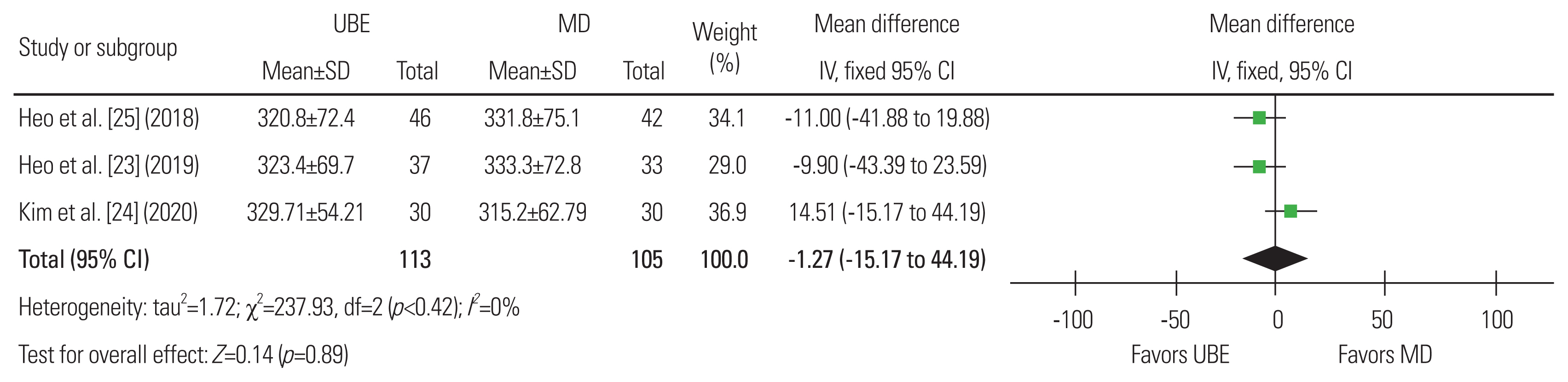
Three articles were included, with 113 patients in the UBE group and 105 in the MD group [23ŌĆō25]. The heterogeneity analysis showed that heterogeneity was not apparent (I2=0%) and the fixed-effects model was used. A mean difference of ŌłÆ1.27 (95% CI, ŌłÆ19.30, 16.77; p=0.89), suggesting that UBE surgery is similar in the degree of postoperative dural expansion to MD surgery, was shown using these data for meta-analysis (Fig. 5).
6. Postoperative complications
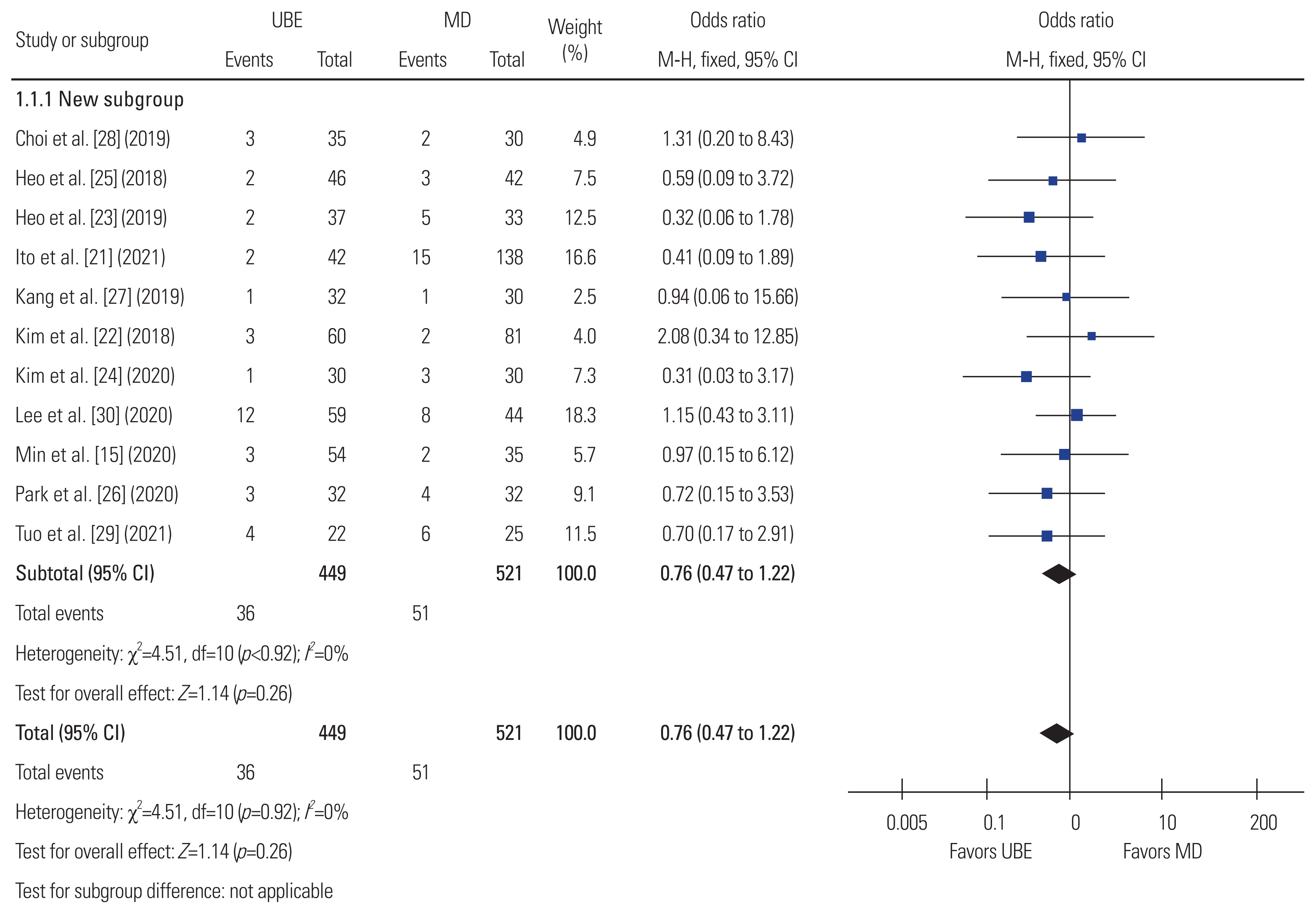
Eleven articles were included, with 449 patients in the UBE group and 521 in the MD group [15,21ŌĆō30]. The heterogeneity analysis showed that heterogeneity was not obvious (I2=0%). The fixed-effects model was used. A mean difference of 0.76 in postoperative complications (95% CI, 0.47 to 1.22; p=0.26), suggesting that UBE surgery is similar in terms of postoperative complications to MD surgery, was shown using these data for meta-analysis (Fig. 6).
7. Hospital stay
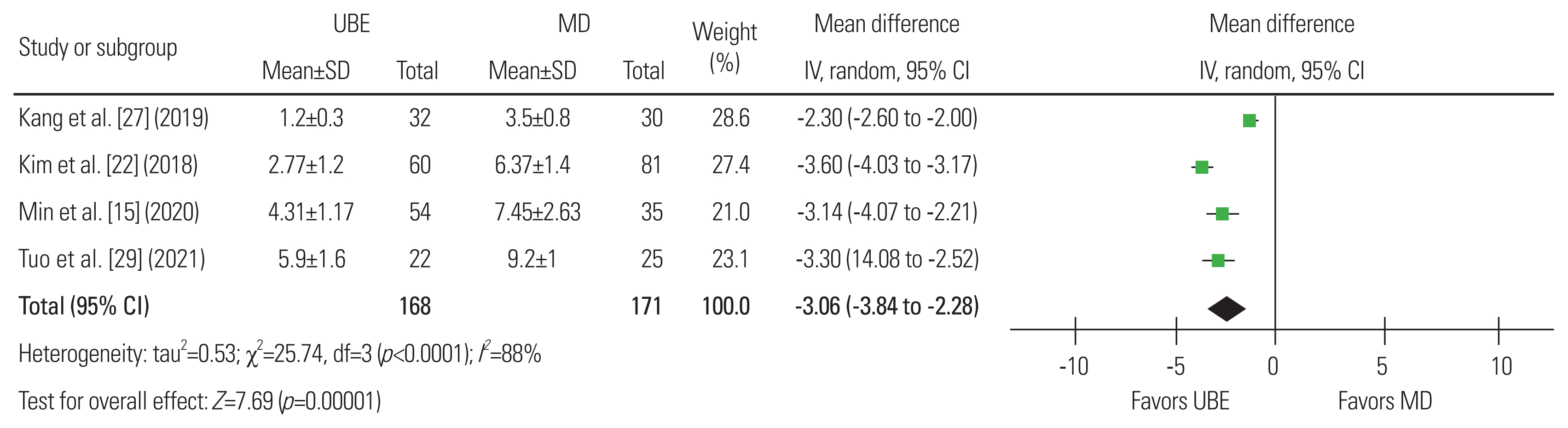
Four articles were included, with 168 patients in the UBE group and 171 in the MD group [15,22,27,29]. The analysis of heterogeneity showed significant heterogeneity (I2=88%), and a random-effects model was used. A meta-analysis of these data revealed a mean difference of ŌłÆ3.06 days (95% CI, ŌłÆ3.84 to 2.28 days; p<0.01), concluding that the UBE operation has a shorter hospital stay than the MD operation (Fig. 7).
8. C-reactive protein changes 1 week after surgery
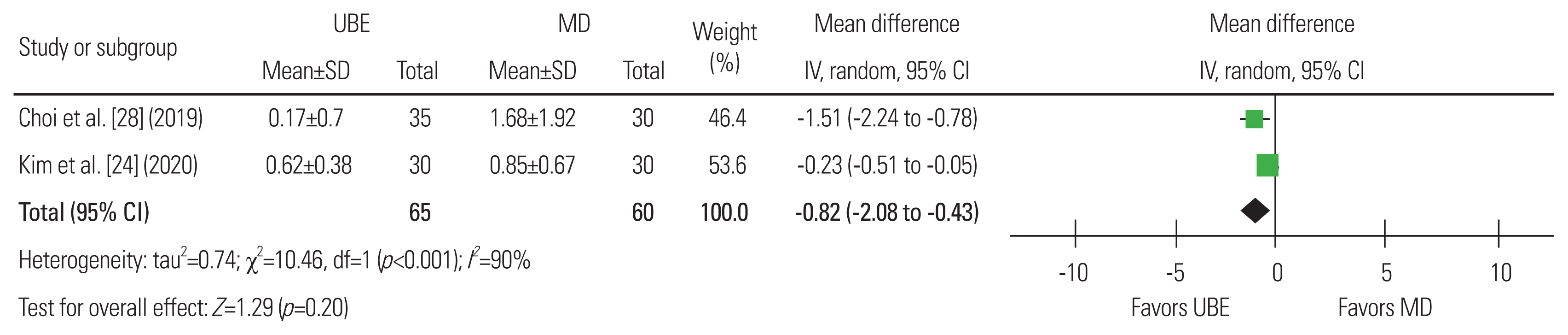
Two articles were included, with 65 patients in the UBE group and 60 in the MD group [24,28]. Significant heterogeneity was observed (I2=90%), and a random-effects model was used. A mean difference of ŌłÆ0.82 mg/L (95% CI, ŌłÆ2.08 to 0.43 mg/L; p=0.20), suggesting that UBE surgery is similar in terms of CRP value at 1 week after surgery to MD surgery, was shown using these data for meta-analysis (Fig. 8).
9. Visual Analog Scale score
Eight articles were included, with 597 patients in the UBE group and 586 in the MD group [15,22ŌĆō26,28,29]. Both the overall and group heterogeneity analyses showed mild heterogeneity (I2Ōēż50%), and the fixed-effects model was used. A meta-analysis of these data revealed a mean difference of ŌłÆ0.04 in the VAS score (95% CI, ŌłÆ0.14 to 0.06 score; p=0.47). There was no significant difference between the two groups in terms of VAS for leg pain at the end of follow-up (more than 12 months) (Fig. 9).
10. Oswestry Disability Index score
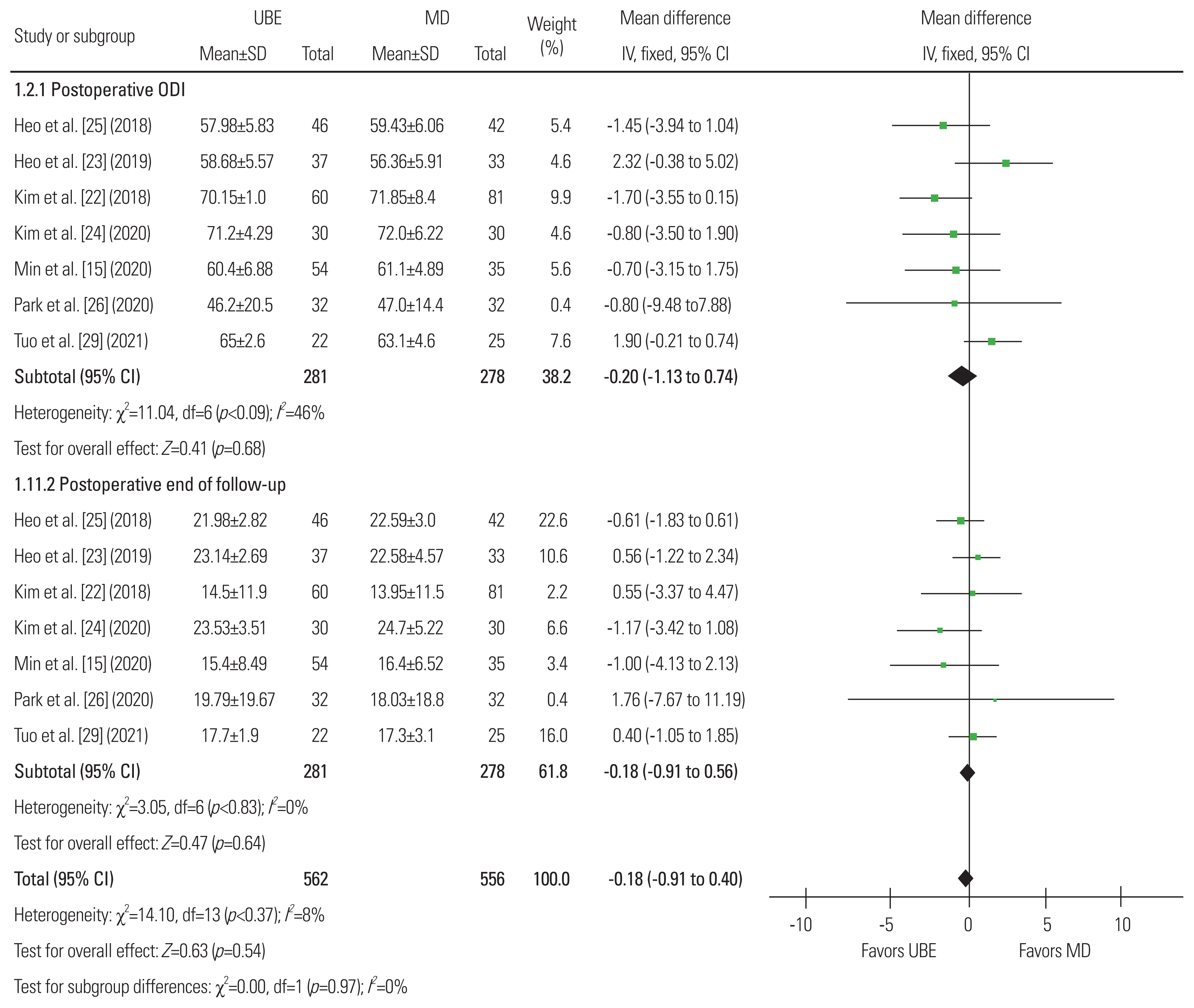
Seven articles were included, with 562 patients in the UBE group and 556 in the MD group [15,22ŌĆō26,29]. Both the overall and group heterogeneity analyses showed that heterogeneity was not obvious (I2<50%) and the fixed-effects model was used. A meta-analysis of these data revealed a mean difference of ŌłÆ0.18 in the ODI score (95% CI, ŌłÆ0.76 to 0.40; p=0.54). There was no difference between the ODI score at the preoperative ODI and the ODI score at the last follow-up (more than 12 months) (Fig. 10).
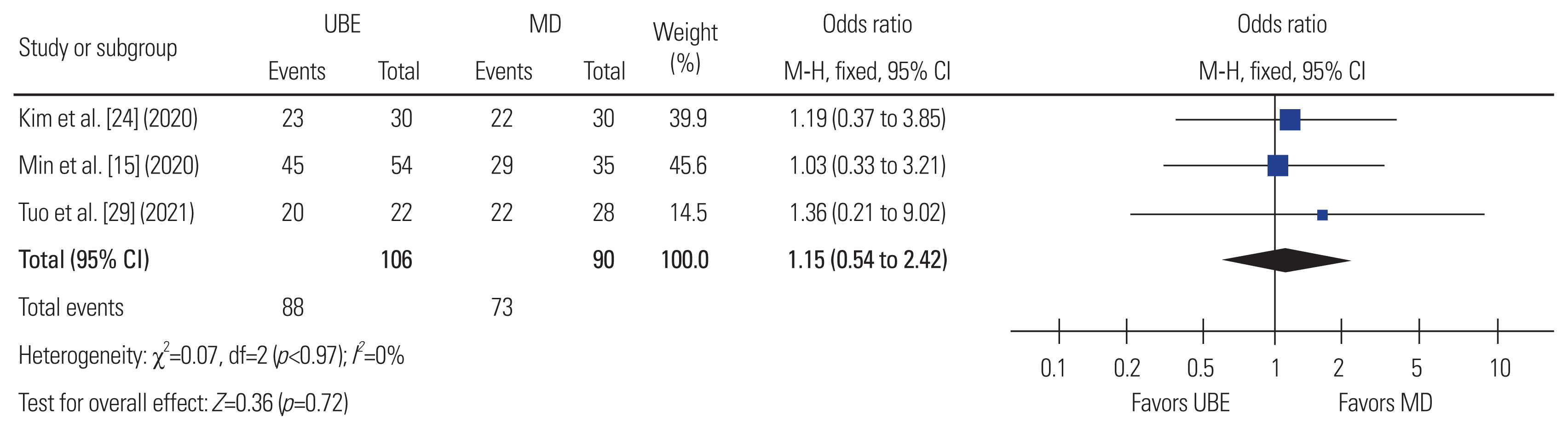
11. The patient satisfaction (the modified MacNab score)
Only three articles were included, with 106 patients in the UBE group and 90 in the MD group [15,24,29]. The heterogeneity analysis showed that the heterogeneity was not obvious (I2=0%) and the fixed-effects model was used. A meta-analysis of these data revealed a mean difference of ŌłÆ0.18 (95% CI, ŌłÆ0.76 to 0.40; p=0.54). Thus, it was not possible to determine a difference in patient satisfaction based on the postoperative modified MacNab score between the two types of surgery (Fig. 11).
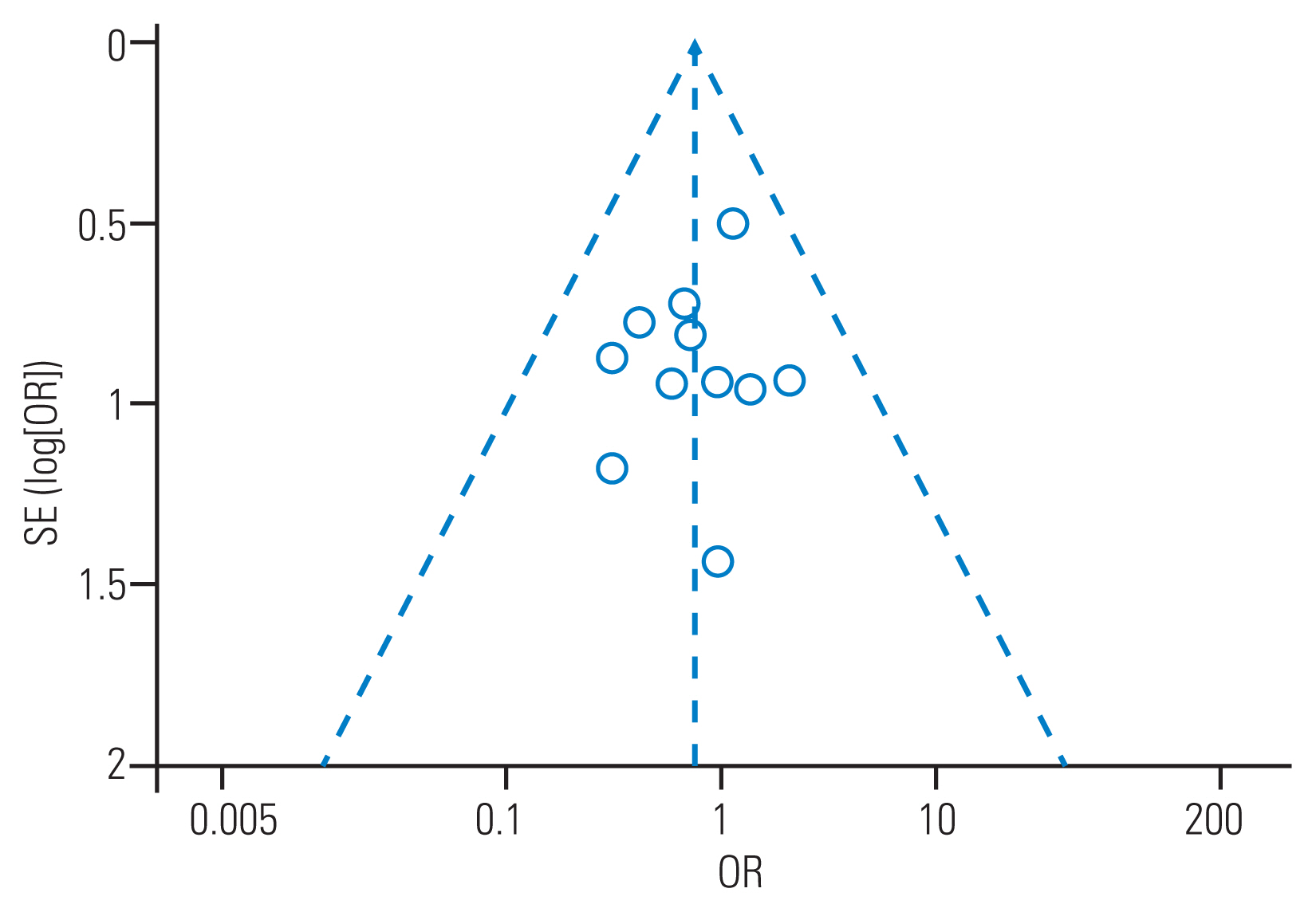
12. Publishing bias evaluation
The postoperative complications with the most included literature were selected for publication bias analysis, and a funnel chart was made. The 11 points in the figure were roughly symmetrically distributed, indicating that publication bias had a small effect on the results (Fig. 12).
Discussion
MD technology has always been the gold standard treatment for lumbar spinal stenosis [3,4]; however, it has certain limitations. It is limited in the scope of operation of the device and the field of view, which may lead to unsatisfactory decompression effects because this technique uses one incision. At the same time, the technology has a long learning curve, which makes it difficult for spinal surgeons to learn [5ŌĆō10]. In recent years, the emerging UBE/BESS technology has used arthroscopic and conventional instruments. Through two channels, the instruments have the advantages of greater operating space and flexibility and a greater field of view. At the same time, it also has the advantages of less intraoperative bleeding and trauma; a smaller, shorter learning curve; increased safety and efficiency; and fewer complications. This technique has been applied to the treatment of lumbar spinal stenosis and has achieved satisfactory results [31ŌĆō33].
From this study, there was no significant difference between the two surgical procedures in terms of operation time, postoperative dural expansion area, complications, or the modified MacNab score. The two surgical techniques included complications, preoperative VAS for leg pain and last follow-up (>12 months) VAS for leg pain, and preoperative ODI score and last follow-up (>12 months) ODI score, and there were no significant differences in any of the aspects. However, a subgroup analysis was carried out due to heterogeneity, and results showed no significant differences. This indicates that these two techniques may be equally applicable to the treatment of lumbar spinal stenosis, are safe and effective, and have similar clinical effects.
The spinal canal decompression extent can be studied using magnetic resonance imaging to measure the dural mater area after surgery. Two minimally invasive surgical techniques were used to treat lumbar spinal stenosis after sufficient decompression, and spinal canal stenosis was significantly enlarged. UBE technique was more flexible and the decompression was more thorough although there was no significant difference between the two, especially for patients with severe lumbar central canal stenosis [34]. Pao et al. [11] showed that the average increase in the cross-sectional dural area after the UBE technique was 105.9┬▒39.5 mm2, which corresponds to a preoperative increase of 201.9%┬▒188.0%. Our comparison results also showed that the UBE technique has greatly improved after surgery. Research has shown that the technology has a short learning curve and can safely and effectively reduce pressure [11].
Serum creatine kinase (CK) and CRP have been used as parameters to assess muscle injury and acute inflammation, respectively. It was impossible to compare the two techniques in terms of surgical trauma due to the lack of postoperative CK data in this study. The results may have been affected by the large heterogeneity of the included studies although the results of this study showed that there were no significant differences in CRP 1 week after the operation. Choi and Kim [28] found that CK and CRP after the UBE technique were lower than those after the MD technique, indicating that the risk of muscle destruction and postoperative infection in UBE surgery was considerably smaller than that of the MD technique [24]. The UBE technique mainly causes less muscle damage through the intermuscular approach and the continuous saline can better flush the inflammatory debris.
The results of this study showed that the UBE technique has lower intraoperative blood loss and hospital stay than the MD technique. There were still significant differences between the two surgical techniques although the included studies were heterogeneous. The average length of hospital stay for patients treated with the UBE technique was 3.06 days shorter than that with the MD technique, likely due to UBEŌĆÖs ability to minimize tissue damage and reduce operative muscle and ligament damage, intraoperative blood loss, and postoperative back pain recovery time [15,22]. This indicates that UBE technology may have some advantages over MD technology and patients undergoing UBE surgery may return to daily activities earlier. The stability of the spine is one of the factors that affects the patientŌĆÖs early activities in the ground. Studies have shown that UBE technology causes minimal damage to the soft tissues and facet joints behind the spine. It can also safely and effectively decompress lumbar spinal stenosis and maintain segmental stability [11,35]. Pao et al. [11] showed that after adequate decompression of lumbar spinal stenosis treated with UBE technology, the contralateral facet joint preservation rate was 92.9% and that of the approach side was 84.2%. This may be another advantage of this technology.
This study has some limitations that need to be acknowledged. First, the best evidence for a systematic review is a randomized controlled trial. However, this systematic review only included two randomized controlled trials and the remaining nine were retrospective controlled studies, which may have distorted the results due to selection and recall bias. Second, the few included studies and the inconsistency of the results of the included studies indicate a high degree of variability in the results. Third, in the data included in this study for comparison, only the intraoperative blood loss and hospital stay were significantly different, and the heterogeneity showed obvious heterogeneity, which may be related to factors that depend on the operation situation and other variables. Further studies should be conducted with the same baseline and a larger sample size. The results of this study still have practical guiding significance despite the limitations.
Conclusions
There were no significant differences in the efficacy or safety of UBE and MD technology in the treatment of patients with lumbar spinal stenosis. However, UBE technology has less intraoperative bleeding and a shorter hospital stay. It can be well applied to lumbar spinal stenosis. It has a slight advantage and is a better surgical option than MD technology. More randomized controlled studies are needed to strengthen the current findings due to the inclusion of fewer studies.