Introduction
A benign fibrous histiocytoma (BFH) is a member of the fibrohistiocytic groups of soft-tissue tumors. Spinal involvement is extremely rare and most reports of BFH of the spine are of skeletal bone tumors [1-4]. To the best of our knowledge, this is the first report of a soft-tissue BFH that occurred in the intraspinal extradural space along the lumbar spine. We report this case of a rare intraspinal, biopsy-proven BFH that was excised completely by surgery.
Case Report
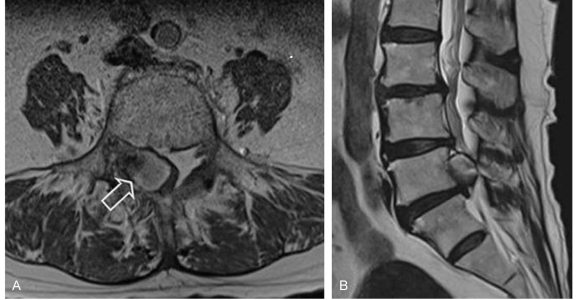
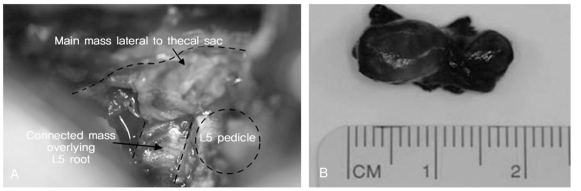
A 66-year-old female presented with severe claudication symptoms in both legs that were more prominent on her right side. Her symptoms had been slowly intensifying over the past seven months. The pain did not respond to conservative treatments, such as medication, physical therapy or pain clinic management. According to her prior medical history, she had suffered gouty arthritis and hyperparathyroidism for several years. On the physical examination, the test for straight leg raising was positive on the right side (50┬░). Her right leg pain radiated along the L5 dermatome. The patient had 4/4 strength of both feet dorsiflexors and big toe dorsiflexors. The laboratory findings revealed leukocytosis (15,200 cells/mm3), elevated erythrocyte sedimentation rate (ESR, 61 mm/hr) and normal C-reactive protein. Her uric acid level was also high (9.2 mg/dl). The laboratory results suggested manifestations of the active phase of gouty arthritis, but intraspinal abscess formation was also possible. Preoperative magnetic resonance images showed a huge intraspinal, extradural, thecal-sac-compressing soft-tissue tumor that extended along the right L5 root to the neural foramen (Fig. 1). The volume of the intraspinal mass was so large that the shape of the thecal sac appeared like a crescent on the T2-weighted axial image. It was decided to remove the mass because the bilateral leg symptoms were believed to be caused from the thecal sac, which was thinly compressed and deviated to the left side. The operation was conducted 10 days after admission due to the hypercalcemia (12.7 mg/dl) and elevated white blood cell and ESR levels. The tumor was a relatively well-marginated, bilobular, inhomogeneous soft-tissue mass with some fluid-containing cystic portion. A right-side unilateral total facectectomy was performed to remove both the intraspinal and foraminal tumor masses. There was moderate adhesion between the ventral cystic tumor mass and thecal sac (Fig. 2). The sheath of the cystic portion of the tumor was so fragile that it was perforated during the dissection and chocolate-color turbid material gushed out from the mass. Complete removal of the mass was possible without neural damage. The intraspinal cystic mass was connected to the solid portion of the remaining mass overlying the L5 root exit zone. Isthmectomy of the L5 lamina was inevitable because the underlying foraminal portion of the tumor extended to the endpoint of the L5-S1 neural foramen. The cystic and solid portion masses were sent for a biopsy and the collected fluid was cultured to identify any microorganisms. Iatrogenic instability resulting from the unilateral facectectomy and hemilaminectomy was expected. Accordingly, posterior interbody fusion with cage insertion and screw-rod fixation were performed. No microorganisms were cultured. The microscopic view of the removed mass revealed a large amount of fibrohistiocytic cells, plump granular cells showing a storiform arrangement with some vascular ingrowths (Fig. 3). After surgery, her bilateral leg pain improved immediately, and the motor power of ankle dorsiflexion returned to the normal range. There was no recurrence of leg pain or motor weakness at the last six months follow-up after surgery. The follow-up magnetic resonance imaging revealed no residual or recurred mass.
Discussion
The most prevalent sites of soft-tissue BFHs are the skin and eyeballs, followed by the pharynx, larynx, trachea and lungs. The incidence of BFH in males is approximately double that of females. BFHs originate from the connective tissue, and the tumor is also called an xanthofibroma. Spinal involvement from cervical to sacral vertebra is reported very rarely [2]. The main features of the tumor are abundant xanthomatous cells with foamy, translucent cytoplasm [5]. Histiocytic and xanthomatous cells are localized between the meshes of the fibroblastic network, which sometimes appears in a storiform pattern. The cystic portion of the tumor in this case was considered to be the necrotic portion of the xantho-amorphous portion.
Soft tissue BFHs can be distinguished from other tumors, such as eosinophilic granuloma, non-ossifying fibroma, malignant fibrous histiocytoma or pigmented villonodular synovitis, from the clinical symptoms, age of detection, prevalent site and radiology and histology features [1,2]. Old age, non-skeletal tumors, absence of the cytological atypia or high mitotic rate, no pigment or crystal formation, no definite eosinophilia, all indicate a diagnosis of BFH. It is believed that this tumor was not associated with gout, hyperthyroidism or any other infectious conditions of the patient. Treatment of an epidural tumor of a BFH involves complete removal. In our case, the tumor adhered to thecal sac and L5 root. Therefore, the unilateral facet joint was excised inadvertently and interbody fusion was performed to regain stability.
We encountered a rare case of BFH as an intraspinal epidural lumbar soft-tissue mass. To our knowledge, this is the first report of spinal involvement with a soft-tissue BFH. We report this case along with a brief history and the radiological and histological findings.