Introduction
Degenerative spondylolisthesis may occur as a result of one or more of the following causes: degenerative changes in discs, facet joints, and ligamentous structure, disc herniation, or previous surgical intervention. The aim of surgical treatment of degenerative spondylolisthesis should be to provide an early relief of symptoms and long-term effectiveness. If conservative treatment is ineffective, the most common surgical procedure is spinal fusion combined with decompression of the neural elements. Recent surgical trends for this pathology are spinal fusion and decompression of the spinal segment by means of the instrumentation technique. Herkowitz and Kurz [1] stated that the patients who underwent the combined fusion and decompression operation had better results than those who underwent decompression alone. In contrast, several investigators have found a little difference in the results between the patients who underwent fusion and those who did not undergo fusion [2,3].
Many follow-up studies of posterolateral fusion or posterior lumbar interbody fusion (PLIF) have been reported [4-7]. On the other hand, only a few have focused on anterior lumbar interbody fusion (ALIF) for spondylolisthesis [8-10]. Since 1981, ALIF has been the preferred surgical method at our department, because ALIF is a reasonable method from the view point of the biomechanics of degenerative spondylolisthesis. We performed direct decompression of the dura via discectomy, according to the Tsuji [11] method . Satisfactory nerve root decompression may be achieved via total discectomy and restoration of intervertebral height, followed by anterior insertion of interbody grafts [12-14].
The aims of the current study were to evaluate the long-term clinical and radiologic results after ALIF for degenerative spondylolisthesis with spinal stenosis and to assess the underlying mechanism of the postoperative adjacent disc disease.
Materials and Methods
1. Patient demographics
Between 1981 and 1992, a total of 28 patients underwent ALIF for degenerative spondylolisthesis with spinal stenosis. Of these, 20 patients were followed clinically and radiographically for more than 10 years (final follow-up rate, 71.4%). There were 6 male and 14 female patients, and their average age at surgery was 58.0 ┬▒ 7.2 years (range, 44 to 70 years). All patients had spondylolisthesis of 3 mm or more, without spondylolysis. Moreover, their myelograms showed a complete or an incomplete block.
The average length of the follow-up period was 17.1 years (range, 10.9 to 23.3 years). Degenerative spondylolisthesis occurred at the L3 level in 5 cases, and the L4 level in 15 cases.
2. Surgical procedures and aftercare program
Operative intervention was indicated when conservative management consisting of rest, physiotherapy, or antiinflammatory medications failed to alleviate the symptom complex of leg pain, intermittent claudication, and neurological changes associated with spondylolisthesis.
During surgery, the extraperitoneal approach through an oblique abdominal skin incision was used, allowing the skin to be pulled down to the level beyond the left iliac crest. Three thick cortico-cancellous bone grafts were harvested from the inner table of the left iliac bone, followed by total discectomy and bone grafting. We performed direct decompression of the dura via discectomy. In total discectomy, we removed the anterior/posterior annulus fibrosus and posterior longitudinal ligament as much as possible, according to the Tsuji [11] method. ALIF is a reasonable approach to correct spinal malalignment in anterior spondylolisthesis, because anterior translation in anterior flexion and a greater tilt of the vertebra are observed. Bone grafts were impacted as firmly as possible [11,15,16].
After ALIF, ceramic interspinous block (CISB) insertion was performed in the lateral position. The CISB provides early stabilization of the posterior lamina, and can prevent the separation of the anterior graft-vertebra bone interfaces, which increases the union ratio [11,15,16]. Briefly, a small median skin incision was made just above the interspinous level identical to the level of ALIF. The supraspinous ligament was removed, followed by minimal resurfacing of adjacent margins of the spinous processes using an appropriately sized dual chisel. The CISB was firmly inserted into the interspinous space using an original inserter.
The patient began walking with a body cast or a flame corset from 2 weeks after surgery. The cast application period was 4 to 6 weeks, followed by return to work with a short or soft lumbar support.
3. Clinical assessment
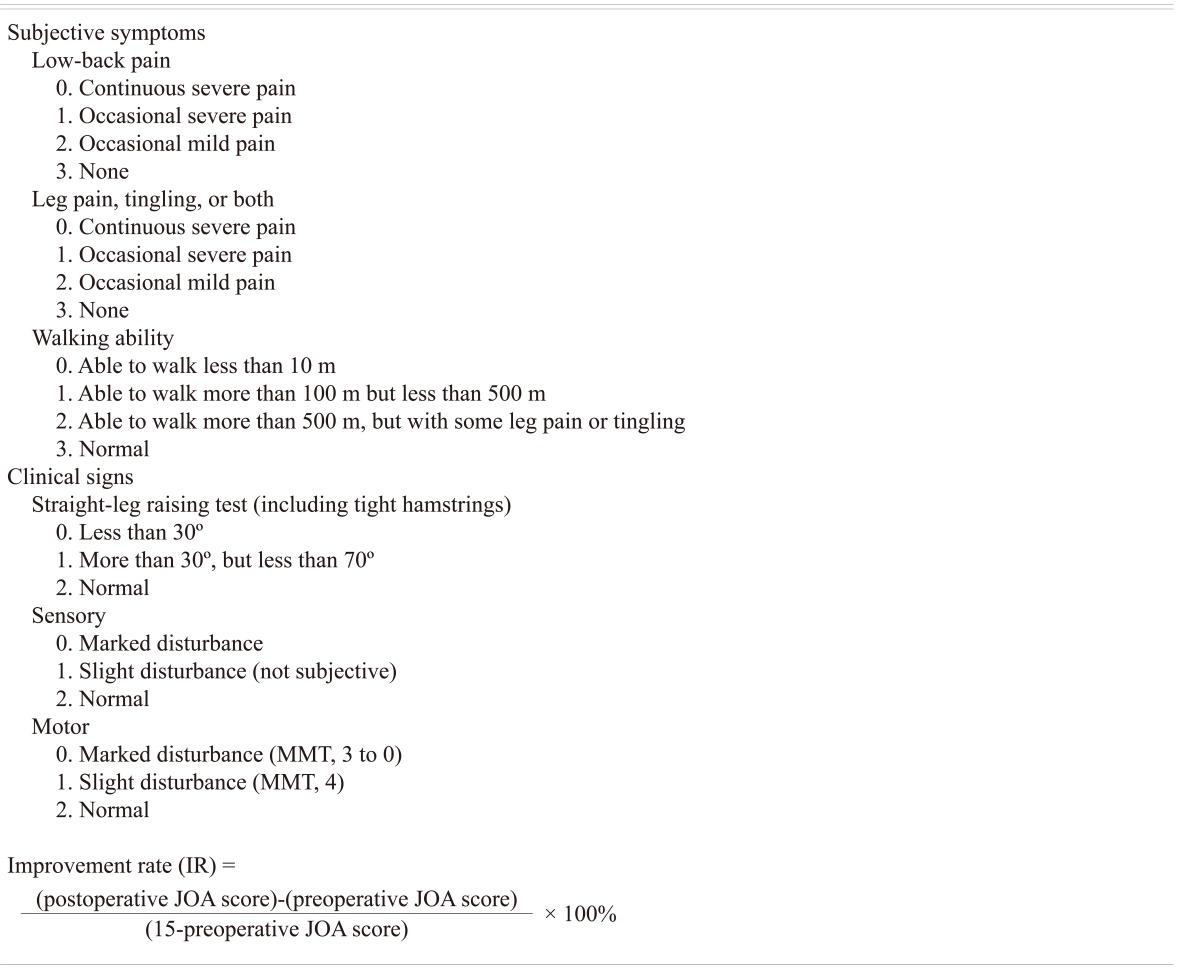
Preoperative clinical data were obtained from the medical records and preoperative radiographs (posteroanterior/lateral lumbosacral spine series). Operation data were also reviewed. Follow-up evaluation was performed via clinical visits. The Japanese Orthopaedic Association score (JOA score) for low back pain (JOA score, 15-point-method) was used to evaluate the clinical outcome according to the previous paper [17]. The items of subjective symptoms (9 points: low back pain, leg pain, and walking ability), clinical signs (6 points: sensory and motor disturbance, the angle of positive straight leg raising test) were evaluated. A completely normal condition would receive 15 points as is the total of the best score. The postoperative improvement rate was determined by the equation mentioned in Table 1. Moreover, a survival curve was generated using the Kaplan-Meier method [18].
4. Radiological assessment
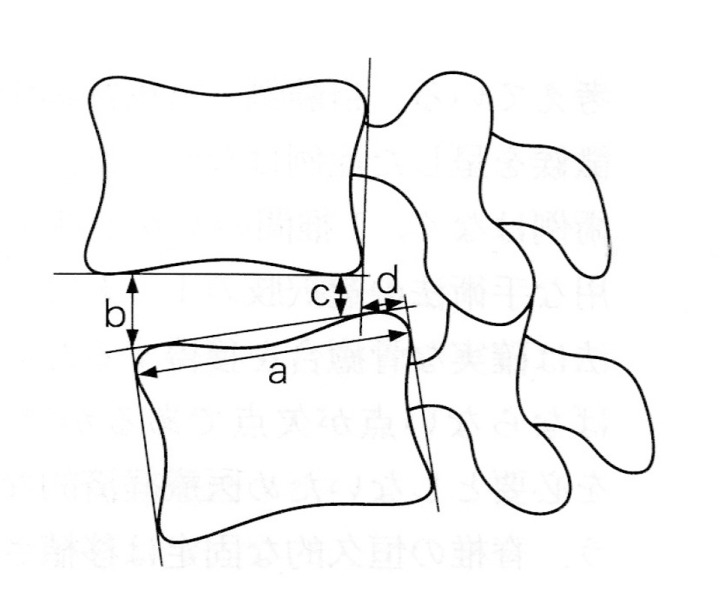
Radiologic analysis was based on the following radiologic items: vertebral slip and disc space narrowing. These parameters were measured before and after surgery. In a lateral radiograph taken with the patient in the standing position, the vertebral slip was measured using the Taillard's method [19]. The intervertebral disc height was expressed as the ratio of the disc height index according to the previous study [20-22]. Briefly, this parameter was assessed by the sum of measurements of the anterior and posterior height of the disc to the anteroposterior diameter of the underlying vertebral body (Fig. 1). The union of the grafted bone was evaluated by a series of radiographs or tomograms according to the methods mentioned in the previous report [17]. The interbody graft union was evaluated by distinct new bone formation at the anterior/posterior margins of the graft.
The postoperative adjacent disc degeneration was defined as intervertebral disc narrowing of more than 10% of the disc height index, and/or the progression of the vertebral slip (2 mm or more), compared with that on the preoperative radiographs. These criteria were based on the previous report [20-22]. Based on these data, we classified the progressive pattern of the adjacent disc degeneration into three types; disc space narrowing (DSN), segmental instability with translation (SIT), or collapse or spontaneous union (CSU).
Results
1. Clinical results and time course
Before the operation, all the patients had leg symptoms, such as radicular leg pain, numbness, or intermittent claudication. Bilateral leg symptoms were observed in 16 patients, and unilateral symptoms were observed in 4 patients, preoperatively. These radiculopathies occurred predominantly in the L5 roots. Urinary disturbance was observed in 7 patients. All patients were followed up for a minimum of 10 years after the surgery.
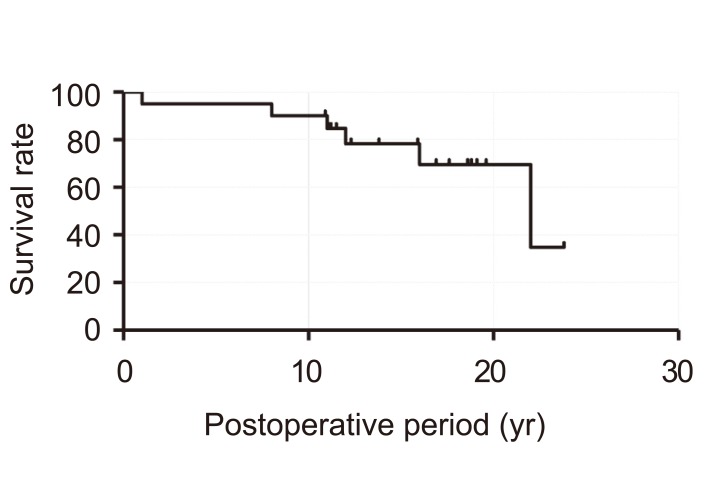
The mean preoperative JOA score was 7.1 ┬▒ 1.8 points. At 1 year, 5 years, and 10 years or more (at the final examination) after surgery, the mean JOA scores were 12.4 ┬▒ 2.2 points, 12.7 ┬▒ 2.6 points, 12.0 ┬▒ 2.5 points, respectively (excluding the data of the reoperated cases). From the graph of the Kaplan-Meier method, the final clinical results (after 10 years or more) had obviously worsened. In the long-term follow-up, six patients (30% of total cases) were required to undergo a salvage operation due to the adjacent disc degeneration. Although, ALIF seemed to provide satisfactory overall clinical results in the mid-term (until 10 years), clinical results of the long-term follow-up data became worse because of deterioration symptoms due to adjacent spinal stenosis (Fig. 2).
2. Radiologic results
All patients had anterior spondylolisthesis. Myelograms of all the patients demonstrated spinal canal stenosis at the spondylolisthetic levels. The mean vertebral slip was 9.1 ┬▒ 3.9 mm (range, 3 to 20 mm) and the average percentage of vertebral slip was 17.8 ┬▒ 5.3% (range, 6 to 50%) by the Taillard's method [19]. After surgery, the mean vertebral slip was decreased to 7.0 ┬▒ 4.4 mm (12.2%, p < 0.05), and it was maintained until the final follow-up (7.0 ┬▒ 4.4 mm, 12.0%; p < 0.05). The mean preoperative intervertebral disc height index at the spondylolisthetic level was 0.41 ┬▒ 0.10. At 1 year after surgery, the disc height index was 0.43 ┬▒ 0.09 and it was maintained until the final follow-up (disc height index, 0.42 ┬▒ 0.09). We measured the lumbar lordosis (L1-L5) on the X-rays, both preoperatively and postoperatively. Preoperatively, the average lumbar lordosis was -0.8 ┬▒ 8.96. However postoperatively, the average lumbar lordosis was 4.85 ┬▒ 6.05. There was an increase in lordosis in 12/20 cases, postoperatively.
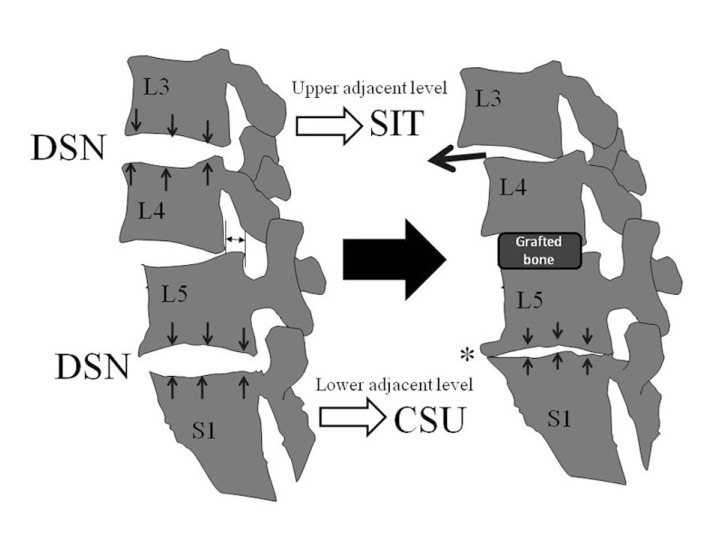
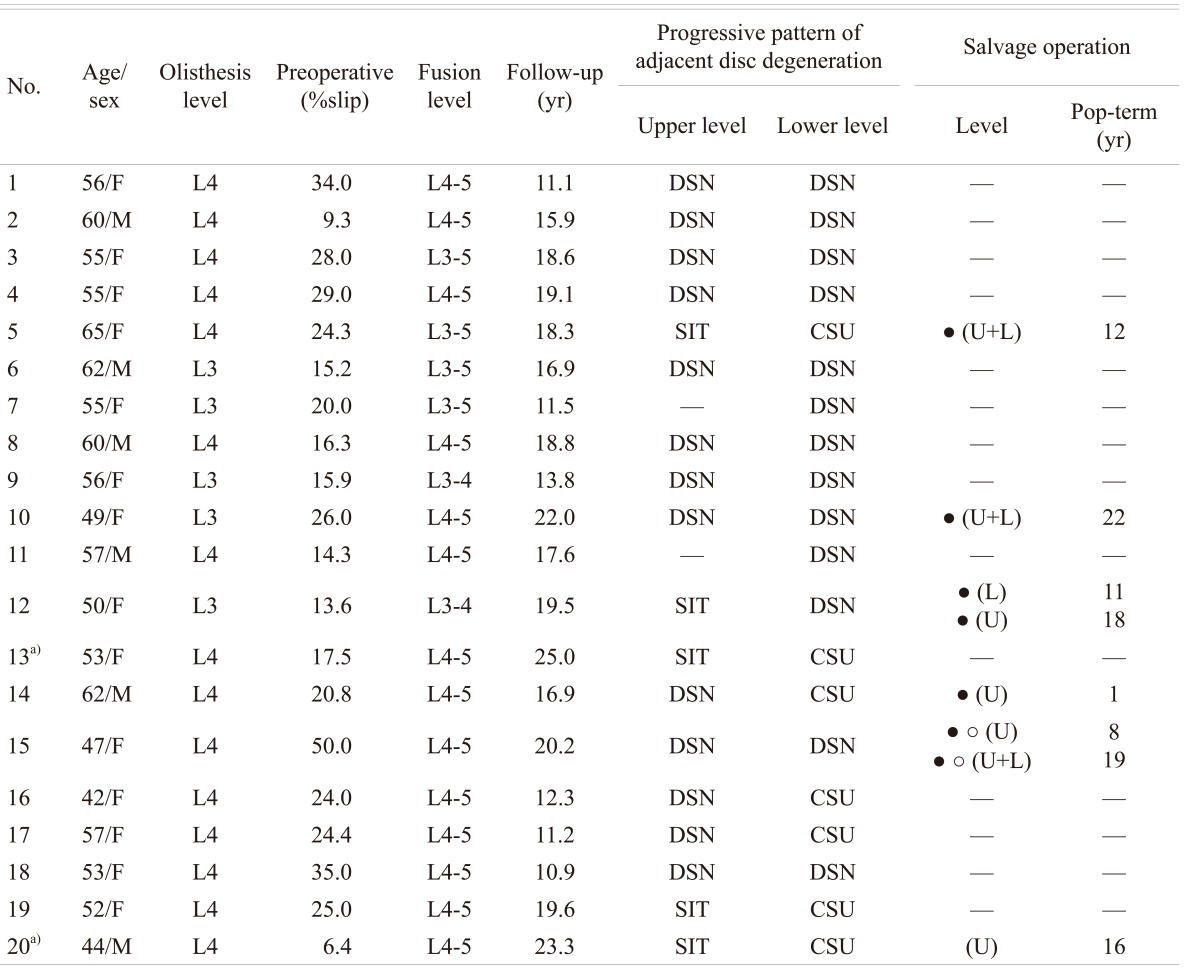
However, the adjacent disc degeneration was observed in all cases. Although, upper adjacent level degeneration was observed in 18 cases (90% of total cases), lower adjacent disc degeneration was observed in all cases. No cases had only upper disc degeneration. The initial stage of disc degeneration was DSN. However after that, the progressive pattern of disc degeneration was different according to the adjacent levels (upper level or lower level). At the upper level, the intervertebral disc showed spondylolisthetic changes (SIT). But the lower discs had osteophyte formation, and occasionally lead to CSU (Fig. 3). The lower level corresponded to the L5-S1 level in 18 of 20 cases, because ALIF was mainly performed at the L4-5 level. Salvage surgeries were mainly performed at the upper level, at an average of 11.7 years postoperatively (Table 2).
3. Illustrative cases
1) Case 1
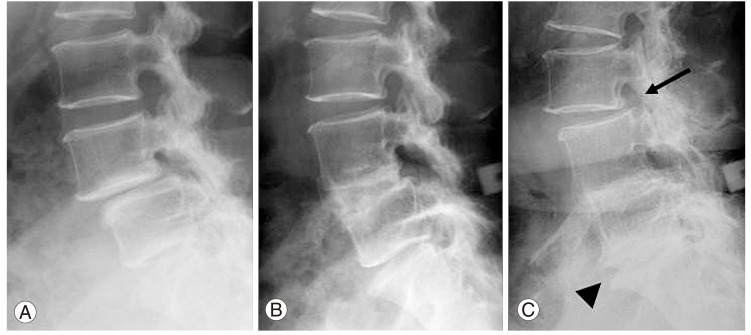
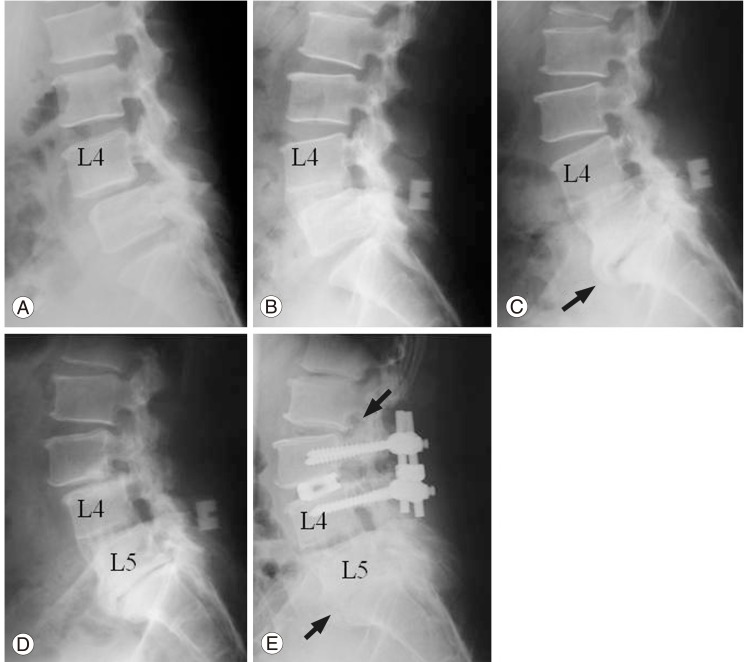
A 53-year-old woman presented with bilateral leg and low back pain. The preoperative JOA score was 4 points. A radiograph showed L4 degenerative spondylolisthesis (17.5%), and an intervertebral disc height index of 0.13. After ALIF, the percentage of vertebral slip was decreased to 11.8%, and the intervertebral disc height was increased to 1.47. The deterioration of the vertebral slip and collapse of grafted bone gradually occurred, but complete union of interbody graft was achieved. At the latest follow-up (25.0 years after surgery), adjacent disc degeneration was observed at both the levels on the radiographs and magnetic resonance imaging (MRI). She reported an occasional low back pain. The upper adjacent disc height index (L3-4) was decreased from 0.43 to 0.26 (decreased ratio, 39.5%) on the plain radiograph. The progressive pattern of was SIT. However, at the lower disc level (L5-S) the collapse of the disc space was observed. The progressive pattern of disc degeneration was CSU (Fig. 4).
2) Case 2
A 44-year-old man reported experiencing low back and bilateral leg pain (in the L5 area). The preoperative JOA score was 10 points. Lumbar spine radiographs showed L4 degenerative spondylolisthesis, (vertebral slip, 6.4%) and an intervertebral disc height of 0.32. After ALIF at L4-5, the vertebral slippage disappeared, and the intervertebral disc height index increased to 1.56. After 16 years, segmental stenosis occurred at the upper disc level (L3-4). This segment showed symptomatic SIT. So the patient underwent the PLIF surgery using instrumentation. At the latest follow-up, 23.3 years after initial surgery, radiographs and MRI showed adjacent disc degeneration at the next level (DSN at L2-3). The disc height index of L2-3 was decreased from 0.52 to 0.31 (decreased ratio, 40.4%). The disc level (L5-S1) lower to the ALIF showed the changes of CSU. He reported experiencing an occasional low back pain, but there was a limited disability (Fig. 5).
Discussion
The characteristic observation in spondylolisthesis includes anterior collapse of disc space. Therefore, it is generally an indication for spinal fusion in an extended position, through the restoration of disc height and vertebral slip.
ALIF is one of the reasonable surgical methods for this pathology [11]. Dennis et al. [23] investigated the disc height after ALIF using autogeneous, cadaver, or mixed iliac crest grafts. They found that 46% of levels were actually narrower than their preoperative heights. Kumar et al. [24] also investigated the subsequent behavior of the disc height after ALIF with femoral strut allograft. Disc height was maintained only in 59% of cases. The disc degeneration in spondylolisthesis is considered to be more severe than that in any other disc pathology, such as herniation, spondylolysis, and so on.
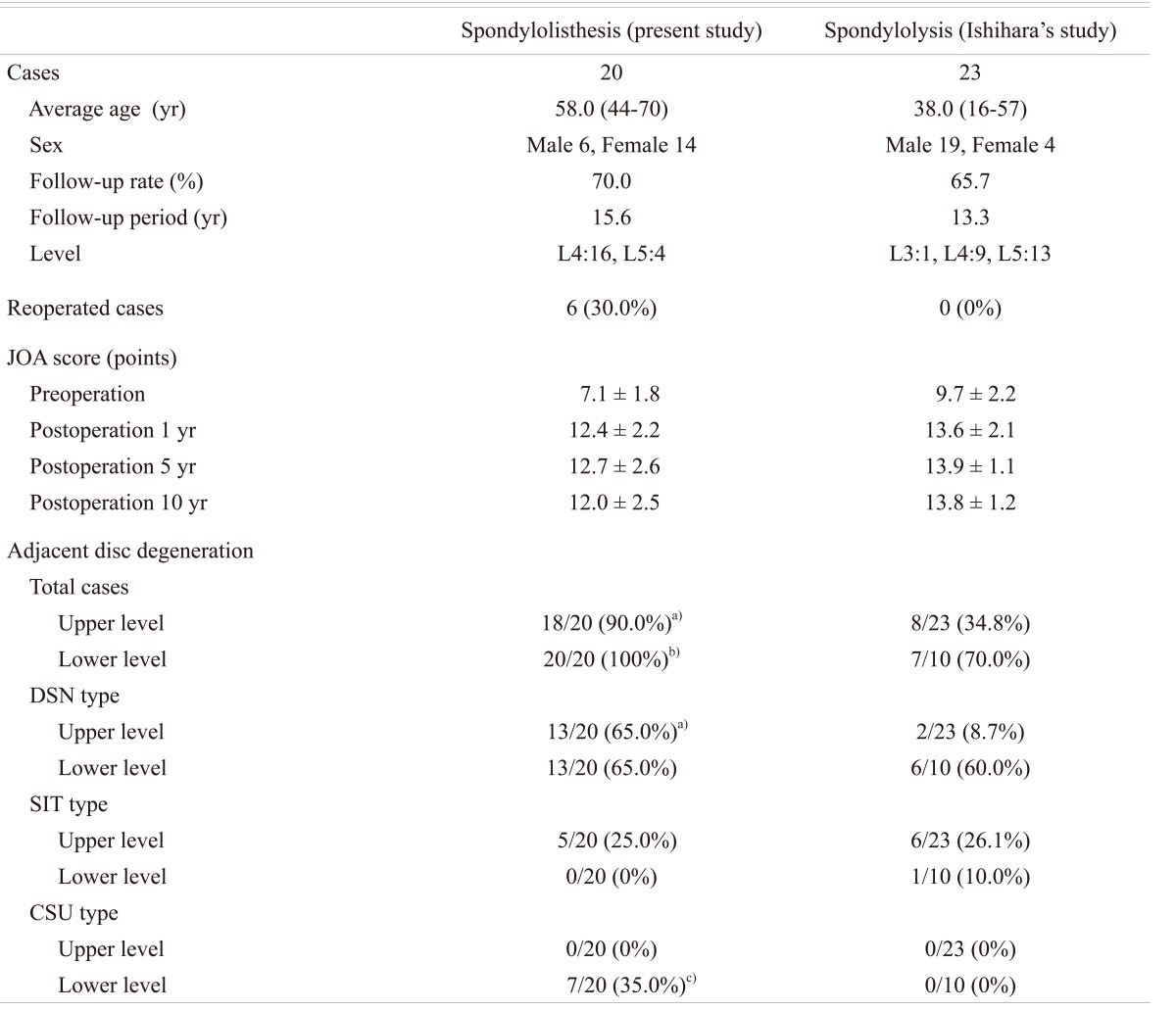
We compared the clinical results of ALIF for spondylolisthesis and for isthmic spondylolisthesis, which we had previously reported (Table 3). The long-term follow-up result of ALIF for spondylolisthesis was worse, and the rate of adjacent disc degeneration was high. Moreover, we performed repeated surgery for adjacent disc degeneration in 6 cases (30%) of this series (present study). One of the reasons for this is the older age population. These patients had severe multi-level disc degeneration and ligament hypertrophy before the initial surgery. Therefore, decompressive laminectomy combined with some type of spinal fusion seems to be beneficial for the treatment of degenerative spondylolisthesis. However, an additional fusion surgery is not always required in case of degenerative spondylolisthesis without symptomatic instability.
Most patients presented with lower leg symptoms, such as radicular leg pain, numbness, or intermittent claudication. In case of spinal stenosis associated with spondylolisthesis (Meyerding type I) [25], we performed decompressive surgery alone [20]. Several authors have advised that fusion surgery should be performed only as a second stage procedure whenever necessary [3]. The indications for ALIF are controversial: our indications for ALIF were Meyerding type II or more, and Meyerding type I with instability (symptomatic and dynamic). Symptomatic instability means severe low back pain or stiffness induced by body motion or manual labor. Most of the patients experience morning stiffness in the low back, or apprehension, frequently. Dynamic instability indicates an abnormal range of motion or translation on the lateral flexion-extension radiographs. Panjabi and White [26] stated that translation of 10 degrees or more at L4-5, or 15 degrees or more at L5-S1 indicated radiological instability. Moreover, abnormal translation of about 2 mm or more is detectable on the plain radiographs. Johnsson et al. [27] stated that pre- and postoperative olisthesis of less than 2 mm should not be counted. According to their criteria, we assessed the dynamic instability on the plain radiograph. We have performed ALIF in cases with these pathologies [11].
In the treatment of degenerative spondylolisthesis with symptomatic or dynamic instability, fusion surgery including ALIF is necessary and important. Takahashi [10] reported that the patients generally maintained satisfactory results up to 65 years of age. To date, the problem of the adjacent disc degeneration after spinal fusion has been pointed out [28,29]. Biomechanical data suggested that the mobility and the intradiscal pressure of the adjacent discs were increased after single-level fusion [8]. Clinically, adjacent disc degeneration has been implicated as a cause of low back pain. Rahm and Hall [29] reported that adjacent disc degeneration occurred in 35% of patients and was associated with worsening of clinical results with time. But, Seitsalo et al. [30] showed that spinal fusion did not significantly increase the rate of adjacent disc degeneration after a mean period of 13.8 years. They found no correlation between the number of degenerated discs or the degree of degeneration and subjective low back pain symptoms. It is important to clarify the cause of recurrent low back pain after ALIF, in order to improve the long-term clinical results.
In our study, the rate of bone union in the grafted area was 100%. The union rate was superior to the rate reported in the best results of a previous Japanese study [9]. Now, the main problem was that of the adjacent disc degeneration. We found different progressive patterns of the disc degeneration according to the levels (upper or lower). The initial stage of disc degeneration was DSN. However after that, the progressive pattern of disc degeneration was different according to the adjacent levels (upper level or lower level). At the upper level, the intervertebral disc showed SIT, but the lower discs showed osteophyte formation, and occasionally lead to CSU (Fig. 3). Salvage surgeries were performed more frequently at the upper level than at the lower level at an average of 11.7 years after the initial operation (Table 2). Therefore clinically, the upper level is important because upper adjacent disc degeneration leads to the symptomatic disorders, which often require repeated surgery during the long-term follow-up.
Although ALIF provided satisfactory overall clinical results in the mid-term, the frequency of salvage surgeries was gradually increased due to the adjacent disc degeneration. A key decision of whether to prevent the adjacent disc degeneration during a long-term follow-up needs to be made.
Conclusions
Although ALIF provided satisfactory overall clinical results in the mid-term (until 10 years), clinical results of the long-term follow-up data became worse. We found different progressive patterns of disc degeneration according to the adjacent levels (upper or lower). The upper level is especially important because upper adjacent disc degeneration leads to symptomatic stenosis due to SIT, which often requires repeated surgery.