Introduction
Chondrosarcomas are malignant cartilage forming tumours. Up to 60% of tumours arise in the thoracic spine and the remaining arise from the lumbar spine (20% to 39%) and the cervical spine (19% to 20%) [1]. The incidence of chondrosarcoma arising from vertebral appendages has not been described in literature. Chondrosarcoma arising from the spinous process is exceedingly rare. There is only one case report of a primary chondrosarcoma arising from spinous process of the first thoracic vertebra (T1) mentioned in the literature [2]. We report a rare presentation of a patient with multiple osteochondromata and a chondrosarcoma arising from the spinous process of 3rd lumbar vertebra treated with marginal excision of the tumour.
Case Report
A 34-year-old gentleman presented to us with a painless mass over the left paraspinal region incidentally noticed one year earlier. He was not aware of any previous swelling in the same region, or other swellings in the body. Examination revealed a 11×4 cm non-tender, hard, immobile swelling in the left paraspinal region of the lumbar spine (Fig. 1). There were no palpable swellings elsewhere in the appendicular or axial skeleton.
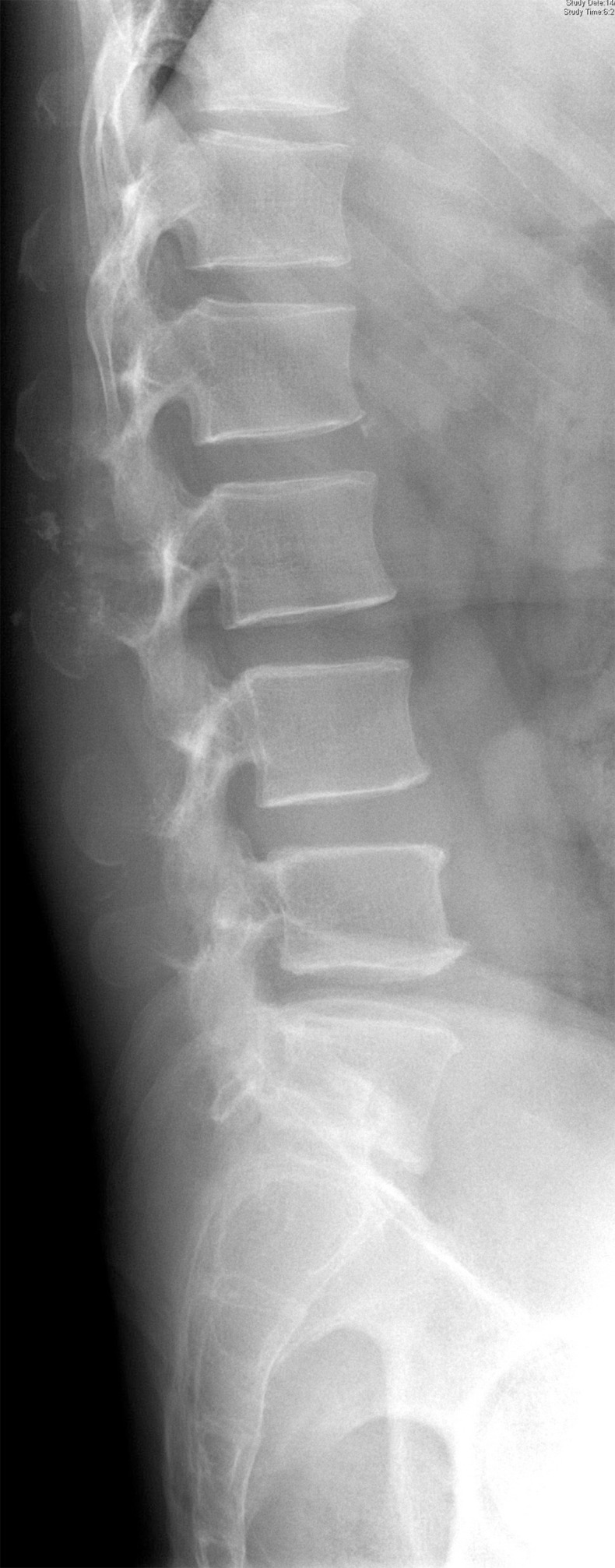
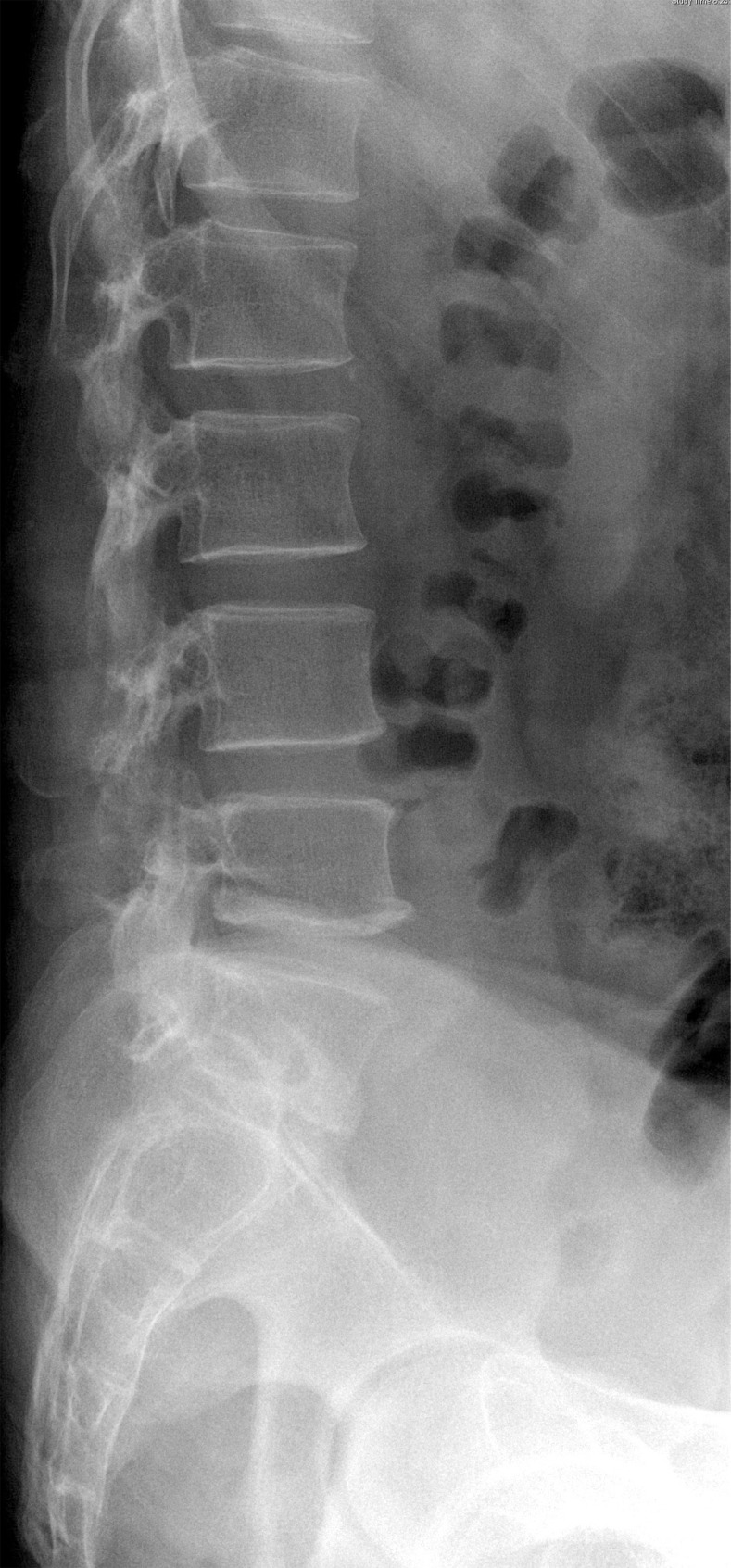
Plain radiographs of the lumbar spine demonstrated. A soft tissue swelling with calcifications, there were mild osteolysis and scalloping seen over the superior border of the spinous process of third lumbar vertebra (Fig. 2). A radiological skeletal survey revealed multiple exostoses in both distal femora, proximal tibiae, proximal humeri, multiple ribs and scapula ranging from 1 to 2 cm in size (Fig. 3).
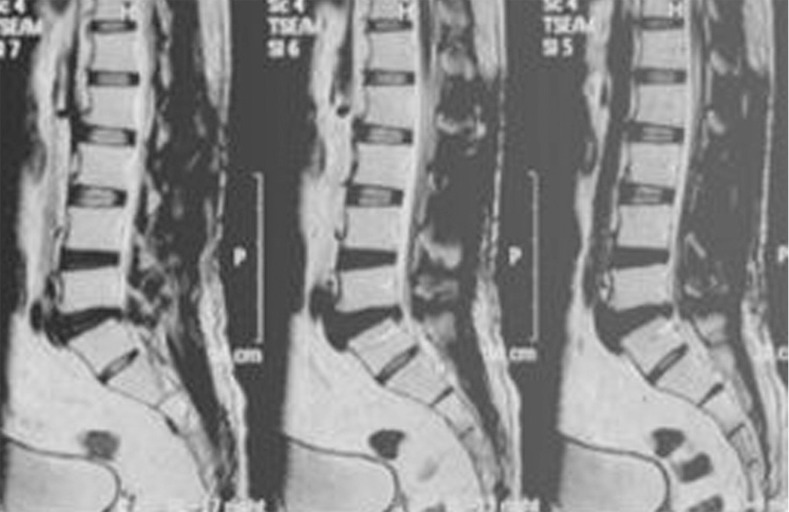
Magnetic resonance imaging (MRI) revealed a large lobulated paraspinal mass involving the multifidus muscle extending from L2-L5 spinous process level measuring 4.7×11.5 cm hypointense in T1 weighted, and hyperintense in T2 weighted/short tau inversion recovery, with no extension into the spinal canal (Fig. 4). A radionucleotide technetium 99 m bone scan did not show any increased uptake at the level of the lesion.
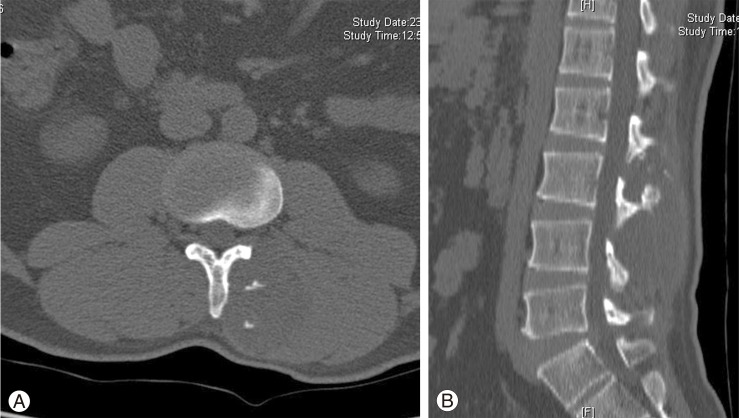
Computed tomography (CT) showed intra-lesional calcifications within the swelling, which arose from the spinous process of 3rd lumbar vertebra (Fig. 5).
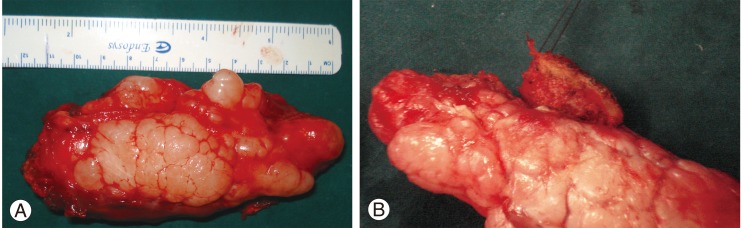
At surgery, a 11×4×4 cm lobulated mass was seen in the left paraspinal region displacing the muscles, arising from the spinous process of L3 vertebra and indenting the lamina of L3 vertebra (Fig. 6). A marginal resection of the tumour and L3 spinous process was done. The postoperative period was uneventful.
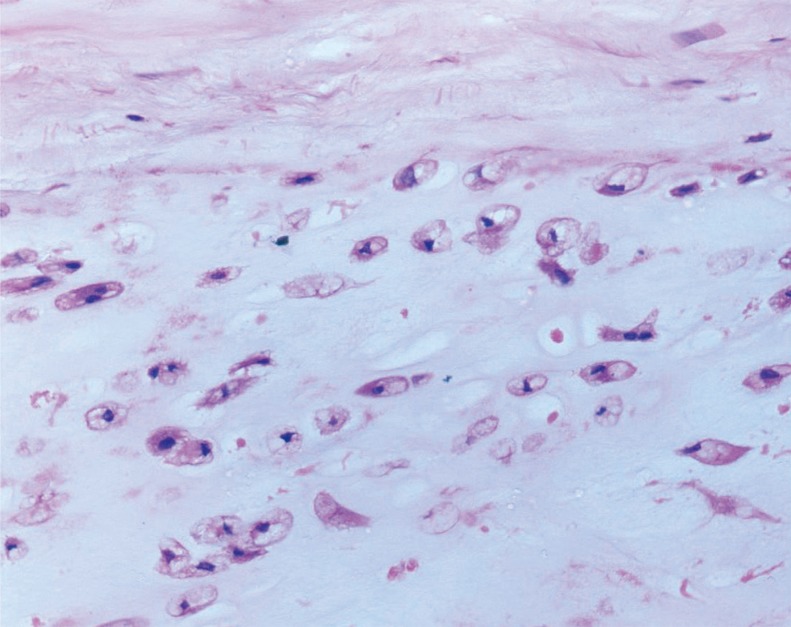
Histopathology revealed a low grade classical chondrosarcoma arising from the L3 spinous process. Curettings from the L3 lamina demonstrated the margins to be free of tumour (Fig. 7).
At one year follow-up, patient had no complaints of pain or recurrence of the swelling. Clinical examination revealed no obvious swelling at the operated site. Plain radiographs showed absent spinous process of the lumbar 3rd vertebra with no evidence of any recurrence (Fig. 8). MRI also confirmed the same (Fig. 9).
Discussion
Chondrosarcoma is a common primary malignant tumour of the bone arising from cartilage cells. Chondrosarcoma is the second most common tumour of the spine after multiple myeloma. Chondrosarcoma may be classified as primary (arising de novo) or secondary (arising from a pre-existing osteochondroma or enchondroma). They may also classified as central (medullary) or peripheral (arising from the surface of the bone). Spinal osteochondromas are extremely uncommon accounting for up to <1% to 9% of all osteochondromas [3-5]. 56% to 80% of osteochondromas arise from cervical spine while 20% to 36% from thoracic spine [6]. Rarely they arise from the lumbar spine [7].
Chondrosarcomas arising from the vertebral axis usually present as a slowly growing mass with an insidious onset, associated with pain and local tenderness, usually associated with neurological deficits at the time of presentation [1].
Radiological features of chondrosarcoma of the spine do not differ from those of rest of the skeleton. Chondrosarcoma usually appear as osteolytic lesions with endosteal scalloping and cartilaginous matrix calcifications. Punctate, pop-corn like calcifications, arcs and ring types have been described for matrix mineralization which is pathognomonic for chondrosarcoma. Chondrosarcoma of the spine usually belong to the mesenchymal or clear cell histological types [1].
Our patient presented with a painless mass incidentally noticed with neither neurological symptoms nor clinical signs of malignancy. The plain radiological and other imaging studies showed classical features of a chondrosarcoma. Histopathology revealed a classical low grade chondrosarcoma unlike the described histological varieties of chondrosarcoma involving the spine.
The only other reported case is a chondrosarcoma of the spinous process arising from the thoracic (T1) vertebra, presenting with a painful mass and neurologic symptoms. Radiography had revealed lytic destruction of posterior elements mainly spinous process. The CT scan showed destruction of laminae and spinous process (centered within the spinous process) with encroachment into the spinal canal [1].
We present our case as a unique presentation of a spinal chondrosarcoma, in view of its rarity, unusual site of origin and histological features of a classical chondrosarcoma.