Spinal Tuberculosis: Diagnosis and Management
Article information
Abstract
The spinal column is involved in less than 1% of all cases of tuberculosis (TB). Spinal TB is a very dangerous type of skeletal TB as it can be associated with neurologic deficit due to compression of adjacent neural structures and significant spinal deformity. Therefore, early diagnosis and management of spinal TB has special importance in preventing these serious complications. In order to extract current trends in diagnosis and medical or surgical treatment of spinal TB we performed a narrative review with analysis of all the articles available for us which were published between 1990 and 2011. Althoug h the development of more accurate imaging modalities such as magnetic resonance imaging and advanced surgical techniques have made the early diagnosis and management of spinal TB much easier, these are still very challenging topics. In this review we aim to discuss the diagnosis and management of spinal TB based on studies with acceptable design, clearly explained results and justifiable conclusions.
Introduction
Although the first documented spinal tuberculosis (TB) cases date back to 5,000-year-old Egyptian mummies, the first modern case of spinal TB was described in 1779 by Percival Pott [1]. Spinal involvement occurs in less than 1% of patients with TB [2,3] but the increasing frequency of TB in both developed and developing countries has continued to make spinal TB a health problem [2,4]. Spinal TB (Pott's disease) is the most common as well as one of the most dangerous forms of skeletal TB and accounts for 50% of all cases of skeletal TB. Although the thoracolumbar junction seems to be the most common site of the spinal column involvement in spinal TB, any part of the spine can be affected [5]. Furthermore, the incidence of neurologic complications in spinal TB varies from 10% to 43% [1].
Recently, the development of multidrug resistant TB, frequency of infection in immunodeficient individuals, more accurate imaging modalities, and advances in spinal reconstruction techniques have all changed the management of Pott's disease [2].
Advanced imaging techniques such as magnetic resonance imaging (MRI) make the early diagnosis of spinal TB easier and a considerable number of patients with spinal TB are diagnosed earlier and treated more effectively before significant neurological deficits develop. However, patients can still present late with considerable spine deformity [1].
Since the advanced imaging modalities and different treatment protocols are developed during these years and drug resistance mandates applying innovative strategies to treat this serious disease, new reviews are always required to assess modern diagnostic modalities and treatment options.
The objective of this review is to discuss the diagnosis and management of spinal TB according to the recent studies published in the literature.
Materials and Methods
In order to extract current trends in diagnosis and medical or surgical treatment of spinal TB we performed a narrative review with analysis of all the articles available to us published between the years 1990 and 2011.
The reports about different aspects of spinal TB, with acceptable design, clearly explained results and justified conclusions according to the data were included in this review. Since, one of the aims of this review was to discuss the historical aspects of TB management we included articles regardless of their time of publication.
Pathophysiology
There are two distinct types of spinal TB, the classic form or spondylodiscitis, and an increasingly common atypical form which is spondylitis without disc involvement [6]. In adults, the involvement of the intervertebral disc is secondary to spread from adjacent infected vertebra whereas in children it can be primarily due to the vascularized nature of the intervertebral disc. The basic lesion in Pott's disease is a combination of osteomyelitis and arthritis, usually affecting more than one vertebra. The anterior aspect of the vertebral body adjacent to the subchondral plate is commonly involved [7]. Spinal TB can include any of the following: progressive bone destruction leading to vertebral collapse and kyphosis, cold abscess formation (due to extension of infection into adjacent ligaments and soft tissues), spinal canal narrowing by abscesses, granulation tissue or direct dural invasion resulting in spinal cord compression and neurologic deficits [7].
Diagnosis
Differentiating spinal TB from pyogenic and fungal vertebral osteomyelitis as well as primary and metastatic spinal tumors may be difficult when only clinical and radiographic findings are considered [8]. A history of tuberculosis, a positive skin test (its value declines in endemic areas), and an elevated erythrocyte sedimentation rate (ESR) may be useful in the diagnosis of spinal TB [8,9]. Biopsy plays a valuable role in the diagnosis of spinal TB infection. The use of DNA amplification techniques (polymerase chain reaction or PCR) may facilitate rapid and accurate diagnosis of the disease [10]. Culturing the organisms is slow and may be inaccurate. Nevertheless, it is still a precious diagnostic method in order to recognize the causative germs. In a small number of cases with imaging and clinical findings suggestive of spinal infection, no organism can be cultured despite multiple attempts. Mycobacterial infection as well as fungal involvement should be considered in these cases.
Computed tomography (CT) provides bony detail, while MRI evaluates the involvement of soft tissue and abscess formation. The relative preservation of the disc, rarefaction of the vertebral endplates, anterior wedging, the presence of separate pre- and paravertebral or intra-osseous abscesses with a subligamentous extension and breaching of the epidural space, concentric collapse of vertebral body, ivory vertebra which is seen at conventional radiographs and refers to an increase in opacity of a vertebral body while preserving its size and contours (with no change in the opacity and size of adjacent intervertebral discs), neural arch tuberculosis, circumferential or pan vertebral involvement, extradural tuberculoma, subdural granuloma, intramedullary tuberculoma, and multilevel spinal TB are considered as the diagnostic clues for this disease in various imaging modalities [8,9,11-14]. Significant bone destruction can be detected on plain radiographs or CT scan (Figs. 1, 2) [15]. However, epidural granulomatous tissue or tuberculoma of the spinal cord may not be detected by these tools [8]. Among the various types of imaging modalities, MRI has the ability to diagnose the disease earlier and more accurately than plain radiographs [9]. Although not specific to spinal TB, there is a decrease in signal intensity of the involved bone and soft tissues on T2-weighted images and the increase in intensity of a uniform thin rim enhancement is a pathogenomic finding suggesting either caseation necrosis or a cold abscess in tuberculosis [16]. In the evaluation of spinal TB with isolated involvement of the posterior elements, MRI is also useful in diagnosis and assessment of the treatment response [17].
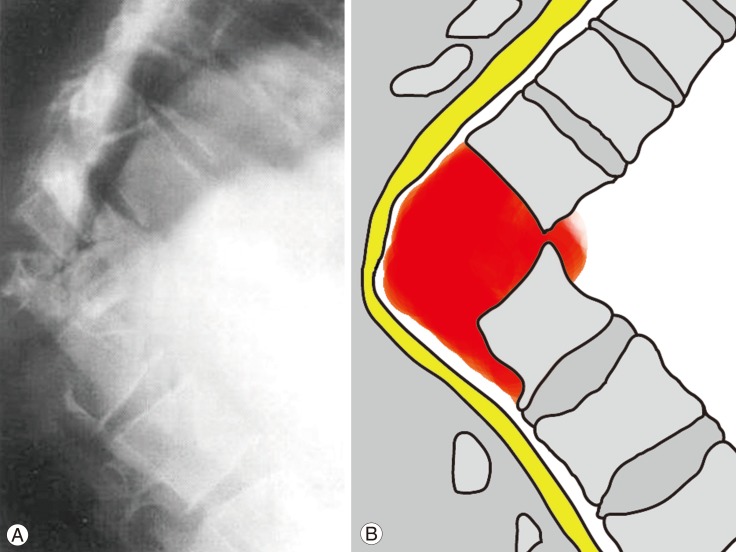
(A) Lateral radiography shows severe kyphosis resulting from significant destruction of two contiguous vertebral segments by tuberculosis infection in the thoracolumbar junction (Modified from Rahimi-Movaghar [15], with permission from Faculty of Medicine, Tehran University of Medical Sciences). (B) Schematic representation of the pathology, affecting the intervertebral disc, vertebral bodies, and anterior paravertebral region (orange). The posterior elements are also involved. As a result of such a significant deformity, noticeable compression endangers spinal cord (yellow).

In comparison to pyogenic discitis, the most distinguishing feature of spinal TB is bony destruction with relative preservation of the intervertebral disc and heterogeneous enhancement. In pyogenic discitis, bone destruction and homogenous enhancement is more frequently observed [18]. The presence of an abscess and bone fragments differentiate spinal tuberculosis from neoplasia and if there is any doubt an image-guided biopsy is indicated [19]. In 88.5% to 96.4% of the cases, a CT/fluoroscopic-guided fine-needle aspiration cytology biopsy is helpful and yields a diagnosis [20,21].
Classification of Spinal TB
In 1985, Kumar [22] introduced a 4-point classification for posterior spinal TB based on site of involvement and stages of the disease. One of the most important limitations attributed to this classification system was only including posterior spinal TB which is relatively rare.
In 2001, Mehta and Bhojraj [23] introduced a new classification system for spinal TB using MRI findings. They classified patients to 4 groups according to the employed surgical technique. Group A consisted of patients with stable anterior lesions and no kyphotic deformity, who were managed with anterior debridement and strut grafting. Group B consisted of patients with global lesions, kyphosis and instability, and were managed with posterior instrumentation using a closed-loop rectangle with sublaminar wires plus anterior strut grafting. Group C patients had anterior or global lesions along with a high operative risk for transthoracic surgery due to medical comorbidities and probable anesthetic complications. Therefore, these patients underwent posterior decompression with the anterior aspect of the cord being approached through a transpedicular route and posterior instrumentation performed using a closed-loop rectangle held by sublaminar wire. Finally, group D patients had isolated posterior lesions that needed only a posterior decompression [23]. This classification only categorizes thoracic lesions which is the most important limitation of this system.
To overcome the limitations described, Oguz et al. [24] developed a new classification system in which spinal TB is classified in to three main types, with type I lesions being subdivided in to two subtypes. In this classification system, lesions are classified as follows: 1) Type I, one-level disc involvement and soft tissue infiltration without abscess, collapse and neurologic deficit. 2) Type I-A, lesions only limited to vertebra and therefore, manageable with fine needle biopsy and medical therapy. 3) Type I-B, abscess formation exceeds the vertebra and the treatment is debridement using an anterior, posterior or endoscopic approach. 4) Type II, one- or two-level disc degeneration, abscess formation and mild kyphosis correctable with anterior surgery. Although instability is not seen in this type, neurological deficit may be present. The treatment includes debridement with an anterior approach and fusion with strut tri-cortical graft. 5) Type III, one- or two-level disc degeneration, abscess formation, instability and deformity that cannot be corrected without instrumentation. Decompression and stabilization of the deformity via an anterolateral, posterior, or combined approach is necessary.
Although this classification system provides a practical classification, it has no special focus on posterior lesions and therefore, this can be considered as the main limitation of this classification system [25].
Management
Historically, spinal TB was managed by rest and decreased weight bearing on the diseased vertebrae by application of an immobilizing bandage, and by promoting the natural processes of healing by general hygienic measures [26].
Simple aspiration or drainage of the abscesses [27] and removing the lesion through the confined posterior route [26] were the first surgical approaches introduced for this disease although the results were not promising enough. In 1895, Menard used an anterolateral extrapleural approach which had been developed and modified by other authors for the debridement of diseased tissues, mechanical decompression of the cord, and bone grafting for anterior spinal fusion [28-31]. This was the first approach to provide adequate exposure for the treatment of dorsal lesions [27]. The transpleural anterior approach was initially introduced by Hodgson and Stock [32] and although this approach requires advanced postoperative care, it has been frequently used [28,33].
Posterior spinal fusion had been advocated and used extensively by Albee [34] and Hibbs [35] in the management of spinal TB. Furthermore, in 1946, Alexander performed a lateral decompression with preservation of the spinal stability by avoiding the laminae and posterior intervertebral joints [33].
Nowadays, the systemic treatment with anti-tuberculosis medications before and after the surgical debridement, the careful debridement of the entire focus of infection, and the successful method to reconstruct for spinal stability are the key aspects in the treatment of spinal tuberculosis [36].
For decision making and management of spinal TB, it can be broadly classified as two groups of lesions: those with neurologic complications and those without [9]. In patients without neurologic deficit, medical therapy is the treatment of choice and surgical intervention may be needed in relatively few cases. In cases with neurologic complications, medical therapy is the first choice again but when indicated, combination of medical and surgical treatments yield the best results. Laminectomy is recommended in patients with posterior complex disease and spinal tumor syndrome. Late onset paraplegia is best prevented by early diagnosis and appropriate treatment. In patients who are expected to have severe (>60 degrees) post treatment kyphosis, one of the surgical goals in the active stage of treatment should be to improve kyphosis [37].
Medical Therapy
Spinal TB is a medical disease and antituberculosis drugs have a main role in the recovery and response of patients [9,38-43]. The efficacy of antituberculosis drugs and other conservative means have been shown in several studies for the treatment of spinal TB in the absence of neurologic deficit, instability, and deformity regardless of presence of paravertebral abscess [38,44-47]. Adequate early pharmacological treatment can prevent severe complications [44]. Combination of rifampicin, isoniazid, ethambutol, and pyrazinamide for two months followed by combination of rifampicin and isoniazid for a total period of 6, 9, 12 or 18 months is the most frequent protocol used for treatment of spinal TB [9]. Tuli's middle-path regimen is widely used with good results [48] and short-course chemotherapy regimens have been demonstrated to have excellent results except in patients younger than 15 years with an initial angle of kyphosis of more than 30 degrees and whose kyphosis increases substantially [49].
In a randomized controlled trial conducted by the Medical Research Council of the UK, the results of surgery and antituberculosis chemotherapy were compared for management of patients with spinal TB [49]. One arm of the trial showed a small but significant advantage of surgery over chemotherapy in preventing progression of kyphosis, but the other arm did not demonstrate superiority of surgery over chemotherapy during long-term follow-up of the patients.
Early diagnosis of spinal TB is very important as adequate early pharmacological treatment can prevent severe complications [44]. Combination of rifampicin, isoniazid, ethambutol, and pyrazinamide for two months followed by combination of rifampicin and isoniazid for a total period of 6, 9, 12 or 18 months is the most frequent protocol used for treatment of spinal TB [9]. The proposed regimen of World Health Organization (WHO) with total duration of 6 months consists of primary treatment with isoniazid, rifampicin, pyrazinamide, and ethambutol for two months followed by four months of therapy with isoniazid and rifampicin (Table 1) [50]. WHO does not give much attention to spinal TB but the American Thoracic Society recommends 9 months of treatment with the same first drugs consumed for the first two months following by seven months of therapy with isoniazid and rifampicin in the continuation phase, while the Canadian Thoracic Society recommends a total time of treatment as long as 9 to 12 months.

It has been demonstrated that the combination of antituberculous therapy for 6 or 9 months and surgical excision of the lesion with bone grafting is as effective as 18 month treatment [49,51]. Moreover, ultra-short course chemotherapy (i.e., treatment with antituberculosis drugs for less than 6 months) has been reported to be as effective as short course and standard antituberculosis treatment when it is combined with anterior partial excisions of pathological vertebrae, large iliac strut graft, and anterior or posterior internal instrumental fixation [52]. After 4-6 weeks of chemotherapy, tuberculosis symptoms and vertebral pain improves in almost all patients, and the ESR and C-reactive protein (CRP) also decreases [53]. ESR and CRP are reliable parameters evaluating the response to treatment and prognosis of spinal tuberculosis [38,54]. However, prolonging the duration of disease or interval to obtain a negative CRP is associated with poor clinical outcomes [55]. Medical treatment alone even improves the neurological deficit [38]. Thus, generally speaking, surgery is not the most appropriate first choice of treatment in many instances [38].
Some authors suggest combining hyperbaric oxygen therapy with antituberculosis treatment to decrease the duration of treatment [41], but more studies are required to support this finding.
Craniovertebral junction TB with the main manifestation of suboccipital pain and neck stiffness [56] is commonly managed with prolonged antituberculosis treatment combined with rigid external immobilization [40,45]. In at least one study, complete clinical and radiological healing occurred in all patients with conservative management [40].
Different components of medical therapy are shown in Table 2, and indications of medical therapy are demonstrated in Table 3.
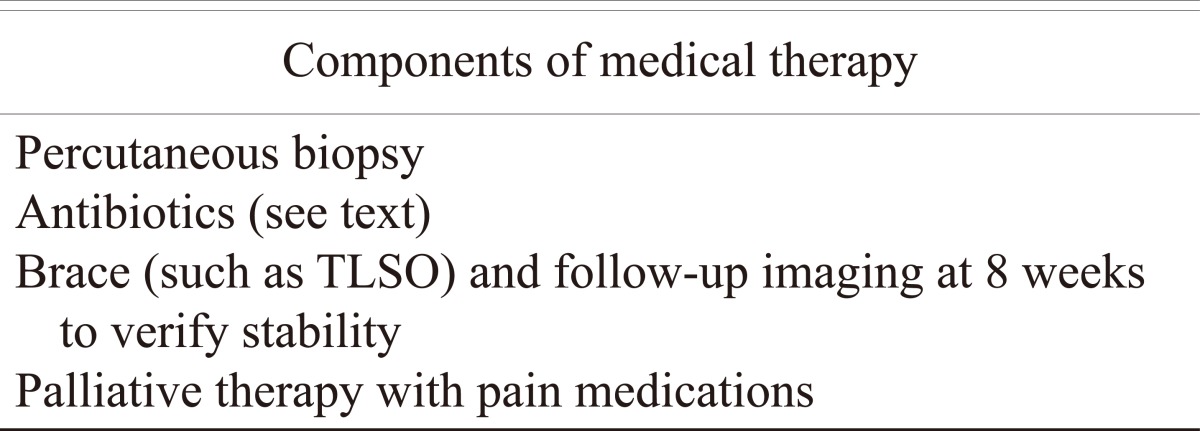
Different components of medical therapy
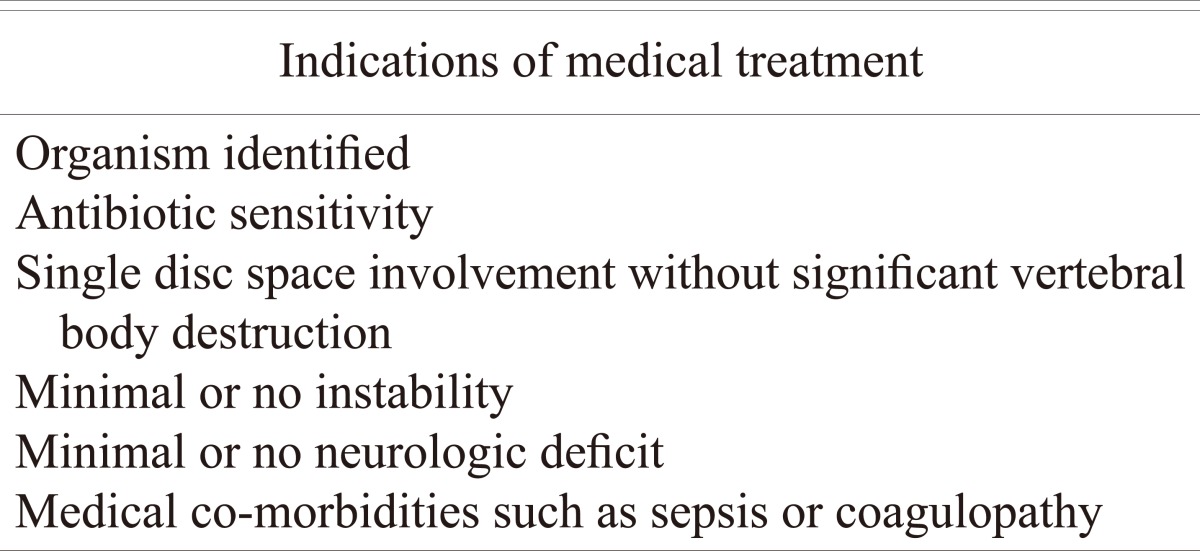
Indications of medical treatment (note that the majority of cases can be treated non-surgically)
Indications of Surgical Intervention
The indications for surgery in Pott's disease are cases with neurologic deficit [38,55], paravertebral abscess, spine instability due to kyphotic deformity (especially in kyphotic angles of 50 to 60 degrees or more which is likely to progress) [9,55,57-62], resistance to the current antituberculosis drugs (which is more encountered nowadays in association with the presence of human immunodeficiency virus [HIV] infection) [9,55], and to prevent/treat complications such as late-onset paraplegia [9].
If surgical treatment of Pott's disease is indicated, delay can cause severe kyphosis, leading to respiratory system dysfunction, painful costopelvic impingement, and paraplegia. It is recommended to perform early surgical intervention to prevent significant spinal instability and neurologic deficit [39].
Teegala et al. [63] developed clinicoradiologic grading from one to three for craniovertebral junction tuberculosis. The higher the grade of the disease, the more association there is with the restriction of active neck movement, severe motor deficit, severe bone destruction (involvement of more than one Denis vertebral column), and cord compression. They recommended early surgical intervention for all patients with grade 3. However, few cases with grade 1 or 2 will need delayed surgery. Employing this scoring system for management of patients with craniocervical junction TB is associated with rapid recovery, early mobilization, and good clinicoradiological outcomes regardless of the initial grade of the disease in patients [61].
Although surgery may not be necessary in advanced stages of craniovertebral junction disease [40], it is recommended for patients with an indefinite diagnosis, initial severe or progressive neural deficit, respiratory distress in the presence of documented mechanical compression, and dynamic instability after conservative treatment [45]. Transoral decompression procedures followed by occipitocervical fusion and antituberculosis drugs have been used with good results in patients with craniocervical junction TB in the presence of cervical myelopathy [64]. In the presence of atlantoaxial dislocation, simultaneous anterior neural decompression via a transcervical retropharyngeal approach, and posterior arthrodesis plus 18 months of antituberculosis chemotherapy have been associated with good long-term results in patients with atlantoaxial dislocation TB [65].
In conclusion, indications for surgery in spinal TB should be limited to tissue sampling when the diagnosis is doubtful, drainage of an abscess in cervical spine (causing difficulty in swallowing and breathing), drainage of a large paravertebral abscess (that does not respond to 3 to 6 months antituberculosis treatment), persistent or deteriorating neurologic deficits in spite of antituberculosis treatment, recurrent neurologic complications, presence of instability in spinal column, and severe kyphotic deformity [27]. Children may need earlier surgical intervention compared to adults due to their growth potential in order to prevent kyphotic deformity [27].
Indications of surgical intervention are shown in Table 4. Table 5 shows the management of epidural abscesses.
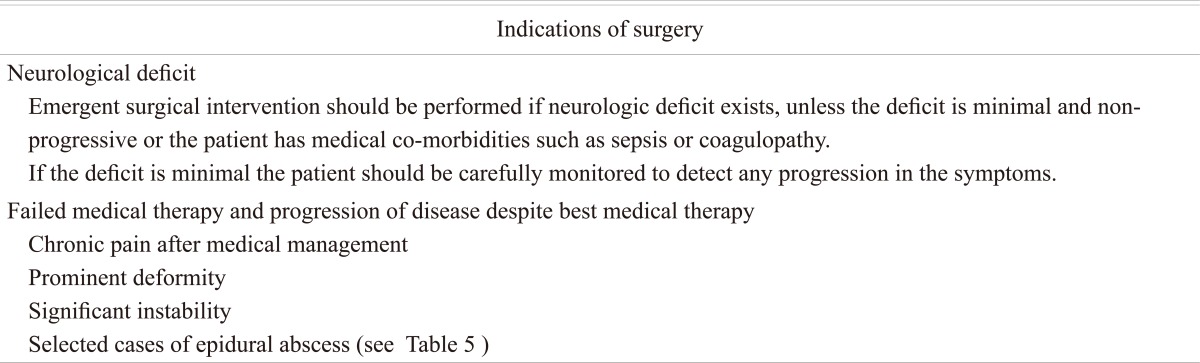
Indications of surgery (note that medical therapy should always be started as well)
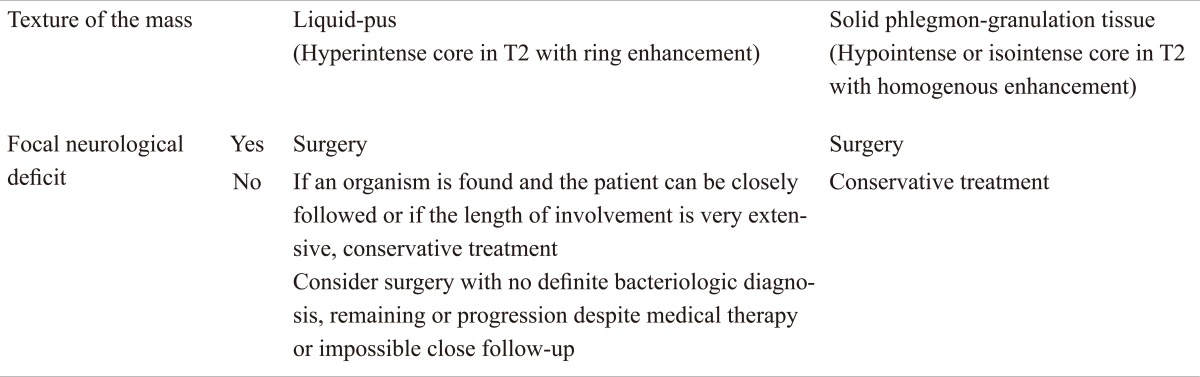
Surgical vs. medical therapy for epidural abscess
Surgical Techniques
The following techniques are currently used for the treatment of TB spondylitis: 1) posterior decompression and fusion with bone autografts, 2) anterior debridement/decompression and fusion with bone autografts, 3) anterior debridement/decompression and fusion, followed by simultaneous or sequential posterior fusion with instrumentation, and 4) posterior fusion with instrumentation, followed by simultaneous or sequential anterior debridement/decompression and fusion [55].
The posterolateral or transpedicular approach has been used extensively for the management of spinal TB. This approach is a viable and importantly a safe surgical option for ventral decompression in thoracic spine TB when followed by antitubercolusis treatment for 18 months and immobilization in an alkathene shell for 3 months [66,67]. Pedicle screw fixation has also been advocated [9,68].
In the setting of non-equipped medical centers, the anterolateral approach is feasible and safe and provides 360 degree exposure for lesions located in the spine from the second thoracic vertebra down to the fifth lumbar vertebra. Using this approach, anterior debridement, decompression, bone grafting (anterior or posteriorly), posterior implant fixation, and kyphosis correction are all options [27,60]. Some authors suggested that anterior instrumentation in the presence of active disease can be dangerous and may fail or be associated with additional complications [27]. However, in our experience instrumented stabilization in a tubercular infected bed seems to be safe if meticulous debridment is performed [69]. On the other hand, some authors reported series of patients that underwent one-stage anterior interbody autografting and anterior instrumentation with good results [68,70,71]. Regarding the type of bone graft, some authors suggested fresh-frozen allograft and anterior instrumentation which is superior to rib grafts in supporting the anterior spinal column. Although fusion occurs late following the use of allografts, the grafts remain stable [72]. Certainly, reoperation to remove the anteriorly placed implants is complex and is associated with higher risks than the first operation [73]. Supplementary posterior fusion should be considered to prevent postoperative kyphosis when this procedure is performed in children [74].
From a biomechanical view point, neither anterior nor posterior approaches alone can stabilize the spinal column as well as combined approaches in cases of spinal TB. Therefore, several authors have suggested that the combined approach may yield better outcomes and prevent future kyphosis more efficiently [75-78]. Performing posterior instrumentation and fusion combined with anterior debridement and fusion in order to shorten the external immobilization period and hospital stay, obtains good and long lasting correction of kyphosis, and prevents further collapse and graft failure and has been recommended in many recent studies [60,67,75,79-81]. However, changes in sagittal alignment have shown that this strategy provides limited kyphosis correction [80]. These combined approaches can be specifically beneficial when doing an anterior correction of a fixed kyphotic deformity with concomitant wedge resection of the posterior elements [27]. Combined approaches can be performed in two ways: 1) Anterior-posterior, anterior debridement/decompression and fusion is performed first; 2) Posterior-anterior, posterior fusion with instrumentation is the first stage. There were no differences in clinical or radiological parameters between these two groups, indicating that either of these two surgical techniques may be selected depending on the patient's condition [55]. One-stage surgical management in children with spinal TB by anterior decompression and posterior instrumentation has been shown to be both feasible and effective [82].
Recently, minimally invasive spinal techniques are introduced as alternative surgical approaches to address different pathologies in the spine, even if fusion is indicated [83]. Such techniques including posterolateral endoscopic debridement and irrigation have also been used with good results for the management of spinal TB [84-87].
Combined anterior and posterior fusion is sometimes preferred in young cases without significant co-morbidities with either of the following indications: 1) Both anterior and posterior involvement, 2) More than three segments involved, 3) Significant degree of kyphosis associated with overt destruction of one or two vertebral bodies, 4) Thoracolumbar junction involvement.
Certainly, to achieve the best results, the surgical treatment of choice for each patient should be individualized. According to different reports, considering the following factors could be helpful in order to select the approach [26,27,55,59,60,63,67,73-75,77-82,88].
1-Patient's age
2-Presence of medical co-morbidities
3-Location of bony destruction (anterior, posterior or both)
4-Location of the compressive lesion with respect to the dura (anterior, posterior or both)
5-Density of the compressive lesion (pus or solid extradural lesion)
6-Patient's bone stock
7-Number of segments involved
8-Degree of kyphotic deformity
9-Region of involvement (craniovertebral junction, cervical, cervicothoracic junction, thoracic, thoracolumbar junction, upper lumbar, cauda equina)
Corrections of Kyphotic Deformity during Active and Healing Phases of Spinal TB
Spinal TB is the one of the most common causes for a kyphotic deformity in patients from many parts of the world, and particularly in developing countries. There is an average increase in kyphosis of 15 degrees in all patients treated conservatively, and a deformity greater than 60 degrees may develop in 3% to 5% of patients. The progression of deformity occurs in two separate phases: active phase of the disease (phase-I) and after healing of the lesion (phase-II) [89]. Development of neurologic deficit and paraplegia after healing of the spinal TB lesion is associated with a worse prognosis than when these complications occur during the active phase of disease [37].
Severity of the kyphosis angle before treatment, level of lesion, and patient's age affect the deformity progression. In general, adults have an increase of less than 30 degrees during the active phase with no additional change while children can experience considerable changes even after healing the TB lesion [89]. The severe spinal deformity in children is likely due to the cartilaginous nature of their bone. Rajasekaran et al. [90] demonstrated that considerable morphological changes develop during growth in both the kyphosis fusion mass and the uninvolved levels above and below the lesion in pediatric cases with healed spinal TB, and these changes result in a variable progression of the deformity during growth. Therefore, they recommended regular follow-up and monitoring of these cases until completing the growth period. Progression of deformity during the active phase as well as after healing the lesion can be classified as follows: Type-I, growth causes an enhancement of deformity. Type-I, disease can be subdivided in continuous progression (type-Ia) and after a lag period of three to five years (type-Ib). Type-II, growth causes a decline in deformity. This could occur immediately after the active phase (type-IIa) or after a lag period of three to five years (type-IIb). Type-III, progression shows minimal change during both active and healing phases and is generally observed in patients with limited disease.
In types I, II, and III progression occurs approximately in 39%, 44%, and 17% of child cases respectively, during the growth spurt. Spine-at-risk radiologic signs can be used for recognizing the children who are at high risk for development of progressive deformity. Children younger than seven years of age, with three or more affected vertebral bodies in the thoracic or thoracolumbar spine and two or more 'at-risk signs', are likely to have progression of the kyphosis with growth and therefore should undergo surgical correction. For the best results, surgery for preventing deformity must be performed relatively early [91], and stabilization with posterior and anterior instrumentation is recommended in patients with severe disease to achieve favorable results [89,91].
A spinal instability score higher than 2 seems to reliably predict patients who will have an increase of more than 30° kyphosis and a final deformity greater than 60°. This can affects the patient's quality of life by potentially causing late onset paraplegia and other neurologic complications [9,59].
Various techniques have been employed to correct the kyphotic deformity in advanced spinal TB. A single-stage posterior Smith-Peterson osteotomy [92] or pedicle subtraction osteotomy (PSO) [93] may not be useful techniques to correct extremely severe kyphotic deformity with a Konstam's angle exceeding 90° [94]. Vertebral column resection through a single-stage anterior-posterior approach is associated with significant blood loss and morbidity with major complications [95]. The traditional two-stage technique allows a thorough decompression with the best long term results, but requires two operations and has increased morbidity [96]. Therefore, recently several reports attempted to introduce new approaches for correction of kyphotic deformity in spinal TB.
A modified multilevel vertebral column resection through a single posterior approach has been introduced for management of deformity. Wang et al. [94] reported results of posterior-only multilevel vertebral column resection for correction of severe spinal TB kyphosis with the Konstam's angle above 90°. Their findings showed that this approach is effective to correct extremely severe Pott's kyphosis. In another study, Deng et al. [97] reported preliminary results on posterior en bloc spondylectomy in patients with spinal TB and angulated kyphotic deformity. They used this technique in 34 patients and the anterior column TB lesion was completely removed by an en bloc spondylectomy with autograft being utilized to stabilize the anterior column. Also, posterior pedicle screw fixation and fusion were performed. These results confirmed that their technique is safe and effective for treatment of spinal TB with a fixed and sharply angulated kyphotic deformity [97].
In severe kyphosis following spinal TB in children, Rajasekaran et al. [98] introduced a new surgical approach. They described a technique of posterior closing-anterior opening osteotomy, which allowed them to correct a rigid post-tubercular deformity as high as 118°. The procedure involved extensive laminectomy, pedicle screw fixation of three levels above and three levels below the apex, a wedge osteotomy at the apex of the deformity from both sides, anterior column reconstruction by appropriate-sized titanium cage and gradual correction of deformity by closing the posterior column using the cage as a hinge [98]. The same approaches were employed in adult patients with good results. This technique has several advantages including approaching just from a posterior, single-stage correction, while allowing for significant correction and fewer complications [99,100].
Careful monitoring and vision of the spinal cord must be performed during deformity correction surgery to prevent elongation of the spinal cord. In cases of late onset paraplegia after healing of the lesion, internal kyphectomy is a viable option and can be performed with acceptable results [59].
In conclusion, although there is paucity of literature on the management of spinal kyphotic deformity caused by TB in children during the healing phase of the disease, combined anterior and posterior osteotomy, deformity correction, and instrumented fusion have been shown to arrest progression of kyphosis and improve neurologic symptoms [101].
Relapse and Recurrence
Using multidrug therapy, the recurrence rate for skeletal TB is approximately 2%, although the relapse rate was much higher when a single drug regimen was prescribed [27]. Long-term multidrug antituberculosis regimens will likely reduce the relapse rate of spinal TB [27].
Multidrug-resistant TB
Currently, multidrug-resistant TB is a global concern and is encountered in 3% of all new cases and 12% of retreatment cases. Multidrug-resistant tuberculosis is defined as a resistant organism to rifampicin and isoniazid while 'other drug resistance' is defined as any resistance to another drug [9]. Lack of clinical or radiological improvement, development of a new lesion or a cold abscess, or an increase in bone destruction in spite of medical treatment for 3 to 5 months may indicate multidrug-resistant TB [9].
For the treatment of multidrug-resistant TB, an average of 6 antituberculosis drugs for at least 24 months is recommended [102]. The most recent WHO recommendations are now posted on their website. These call for 5 drugs that are expected to be effective in the initial intensive phase and 4 drugs that are likely to be effective in the continuation phase. Duration of the initial phase is 6 to 9 months and the total therapy lasts 20 to 24 months. These drugs are not safe and adverse reactions will develop in a considerable number of patients [102]. Therefore, close monitoring of patients for development of adverse reactions is necessary [9]. Also, early surgery may be indicated to confirm the diagnosis, isolate the organism, and reduce the bacterial load [9]. The determinants of a successful outcome in multidrug-resistant TB are as follows:1) Progressive clinical improvement at 6 months following chemotherapy, 2) Radiologic improvement during treatment, 3) Disease with Mycobacterium TB strains that are resistant to less than or up to three antitubercular drugs and the use of less than or up to four second-line drugs in treatment, and 4) No change of regimen during treatment [102].
Atypical Forms of Spinal TB
Atypical spinal TB is defined as compressive myelopathy with no detectable spinal deformity and the absence of radiological appearance of a typical vertebral lesion [9,13,103]. In other words, any forms of spinal TB that do not manifest with typical clinical and radiologic features of the disease are considered to be atypical spinal TB [14]. An incidence of 2.1% has been reported for atypical TB [104].
Diagnosis of these lesions needs special attention with high clinical suspicion because they are rare and difficult to diagnose. Therefore, they may be diagnosed in the late stages. However, it has been suggested that these lesions can have the same outcome and prognosis as typical spinal TB if diagnosed and treated at the early stages [14]. The treatment principles for patients with atypical spinal TB are similar to those with typical features [14].
Multiple Vertebral Disease
Although the reported incidence of this atypical form of spinal tuberculosis is approximately 7% [14,105], it is estimated that the incidence of this type of spinal TB would be higher if whole spine MRI is performed. In a study on 40 patients, Pandit et al. [106] found that multilevel involvement of the spine was observed in 25% of patients using bone scintigraphy. In another study conducted by Polley and Dunn [107] in South Africa, an incidence of 16.3% (16 out of 98 patients) was found for noncontiguous, multiple level spinal TB.
Multiple level spinal TB may occur as continuous involvement of two to four contiguous vertebrae, or may affect different levels in different parts of the spine. The lesion in continuity typically is seen in immunodeficient patients and in patients with hemoglobinopathies [14,108-111].
The non-operative treatment of patients with multilevel spinal TB without neurologic deficit is the same as the treatment of a patient with a typical spinal TB. Accurate neurologic examination and MRI before scheduling surgery in patients with multilevel spinal TB is critical to determine the level of compression [106].
Several surgical techniques have been used for the management of multilevel spinal TB. Cavuşoğlu et al. [112] reported long-term results on anterior radical debridement, decompression, and fusion using anterior spinal instrumentation and tibial allograft replacement for management of multilevel spinal TB in 22 patients. Their findings revealed that this technique provides correction of the curvature, prevents further deformation, improves sagittal and coronal balance, and restores neurological function. Ozdemir et al. [113] also suggested that radical debridement followed by anterior spinal stabilization with a structural allograft fibula is effective for interbody fusion and correction of the spinal deformity for the management of multilevel spinal TB.
Zhang et al. [114] used 1-stage anterior debridement, strut autografting, and posterior instrumentation combined with antituberculosis chemotherapy for 12 to 24 months in multilevel TB spondylitis of the upper thoracic region. They suggested that this technique is safe and effective for the management of multilevel TB spondylitis.
Prognosis and Outcome of spinal TB
Effective medical and surgical management of spinal TB has improved outcome of these patients significantly even in the presence of neurologic deficits and spinal deformities [68]. However, since various surgical techniques have been used for the management of spinal TB, reported outcomes are heterogeneous and decision making for the selection of a specific technique in the management of all patients is difficult.
Neurologic complications due to Pott's disease seem to be "relatively benign" if early adequate medical and surgical managements are employed [3]. Younger age and radical surgery in conjunction with antituberculosis chemotherapy have been suggested as favorable prognostic factors [115]. Some of the other more important factors associated with prognosis and the development of deformity during the course of spinal TB have been pointed out in above sections of this review.