Introduction
Is it helpful to add petit demineralized bone matrix (DBM) for an instrumented posterior lumbar interbody fusion (PLIF) with auto-local bone?
Arthrodesis of the spine has been used to treat various sorts of spinal disease and more than 50% of bone graft has been used for that purpose [1,2]. Success rate of spinal fusion has been raised up as instrumentation has developed. Increment of patient's satisfaction, however, has been limited significantly due to the morbidities of auto-graft donor site. There are several options that have been used independently or as a combination to avert the auto-iliac bone harvesting. Those were as follows; allogeneic bone graft, auto-local bone graft, bone substitute graft, interbody bone graft, increasing fixation power by pedicle screw system and cages. DBM, which enhances osteoinductibity, was appraised available as a graft extender of the auto-iliac bone in large volume. However, its value was skeptical as an adjunct to the auto-local bone or other ostoeconductive materials. DBM is recognized as an osteoinductive material; hence, it should be meant to act as a graft enhancer for the graft materials, which have a litter or no osteoinductivity. As PLIF technique has been becoming popular, auto-local bone chips fortified by DBM have been used as a graft material more and more. However, there has been no clinical study that supports the availability of such construct thus far. To my knowledge, PLIF using auto-local bone chips and small amount of DBM is regarded as a best sample to appraise this subject. Furthermore, in case of instrumented PLIF with pedicle screw and cage system, structural support can be fortified and an interbody space, which is surrounded by large cancellous plates, would give more favorable circumstance than posteolateral fusion (PLF) for osteosynthesis. There have been many reports that note successful fusion rate in this sort of spinal fusion surgery even without an annexing of DBM. Therefore, we designed two stage investigations to see the early influence and the final consequence of DBM on auto-local bone as a graft enhancer. As the first stage, bone formation status was evaluated at 6 months after the index surgeries, which has been noted as a usual fusion time after spine surgery and as the second stage final fusion rate was evaluated at least 2 years after the index surgeries.
Materials and Methods
1. Materials
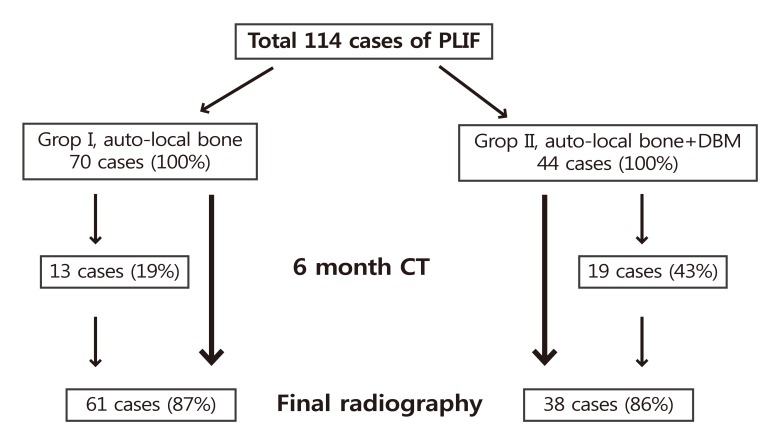
It was designed as a case controlled study; however, data were collected prospectively. The patients of degenerative spinal disease or spondylolytic spondylolysthisis, who underwent spinal fusion surgeries between January 2006 and October 2006, were included. Those who under 50 and over 80 years old, more than 3 segments and more than 3 times of surgery were excluded. A total of 114 cases of 92 patients underwent surgeries during the index period. Seventy cases of group I used auto-local bone chips and 44 cases of group II used auto-local bone chips and 1 mL of DBM per segment. The type of bone graft was alternated according to the date and previous consent was obtained in group II cases. If a patient refused to use DBM, he or she was shifted to group I.
2. Method of surgery
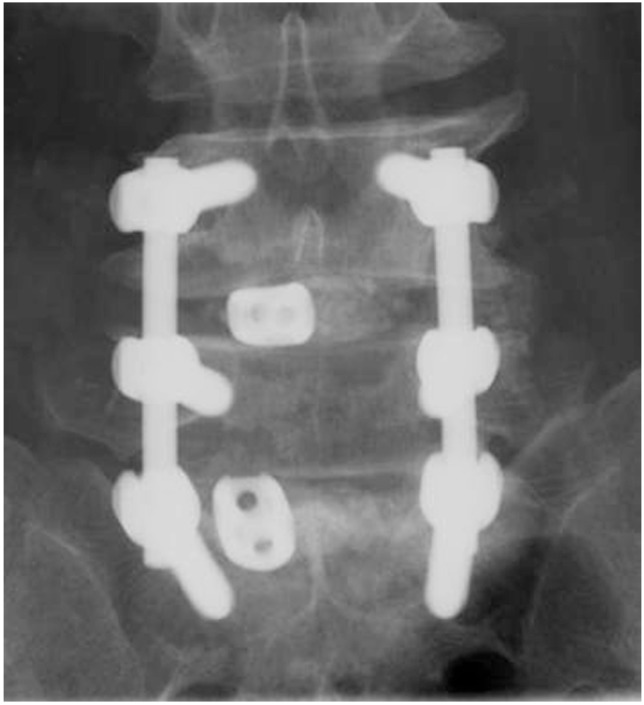
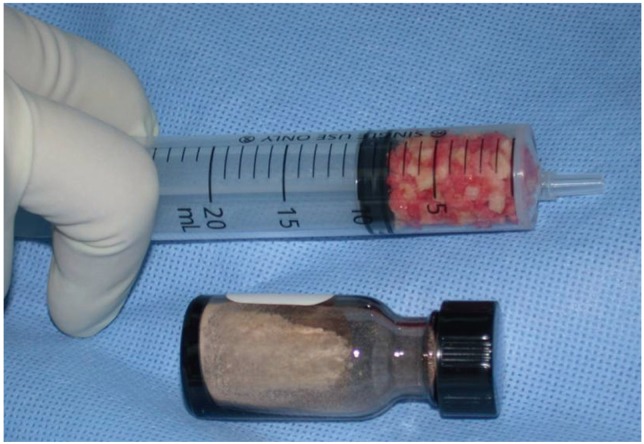
Conventional posterior approach was used. Decompression was performed unilaterally or bilaterally according to the necessity. Disc extirpation was performed unilaterally in all cases. Pedicle screws and rods were instrumented and a cage per a segment was inserted through a symptom dominant side. The auto-local bones that were achieved while performing decompression were made into small chips of 1 to 2 mm. In group I, those were grafted into the interbody space and a cage that was charged with them was inserted at one side. In group II, 1 mL of DBM per segment was annexed to auto-local bone chips and grafted with the same manner as group I (Fig. 1). All cases used Allomatrix (Wright Medical, Arlington, TN, USA). The amount of auto-local bone chips was measured by a 20 mL syringe in the maximum compression state (Fig. 2).
3. Method of analysis
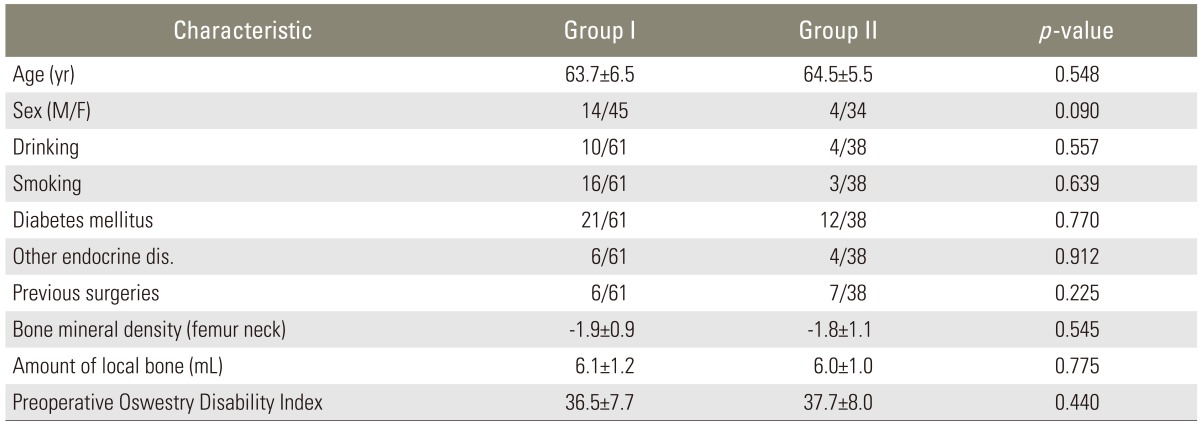
Sampling homogeneity of the two groups was reviewed in terms of age, sex, drinking, smoking, medical comorbidity, such as diabetes mellitus, and other endocrine diseases, previous surgeries at the same segments, bone mineral density, amount of grafted bone per segment and functional score by Oswestry Disability Index ver. 2 (ODI). The norm of frequent alcohol drinker was more than twice a week and more than 1 year before surgery. Bone mineral density was examined at the femur neck by Dual-energy X-ray absorptiometry (Osteoprima, MediRay, Suwon, Korea). Preoperative and final clinical functional status was assessed by ODI. Complications, especially osteoinductive material induced complications, were investigated.
1) Early assessment by computed tomogram
The degree of bone formation was assessed by sagittal and coronal reconstruction images at 6 months┬▒2 weeks. Thirty two cases of 27 patients were examined during the pertinent period. Group I was 13 cases (19%) and group II was 19 cases (43%). Mid-sagittal image and anterior 1/3 coronal image were assessed by the method devised by the senior author (Fig. 3). The details were as follows; grade I is almost no bone formation, grade II is bone formation of less than 50% of grafted zone, grade III is bone formation of more than 50%, but incomplete continuity of bone mass and grade IV is diffuse and continuous bone formation. Numeric scales of 1 to 4 were given to each grade. Two orthopedic doctors, who were blind to the study design read the images independently. The sum of each plane scores of the two readers was counted as a final score for the segment. Each segment was counted as a case.
2) Final assessment by plain radiography
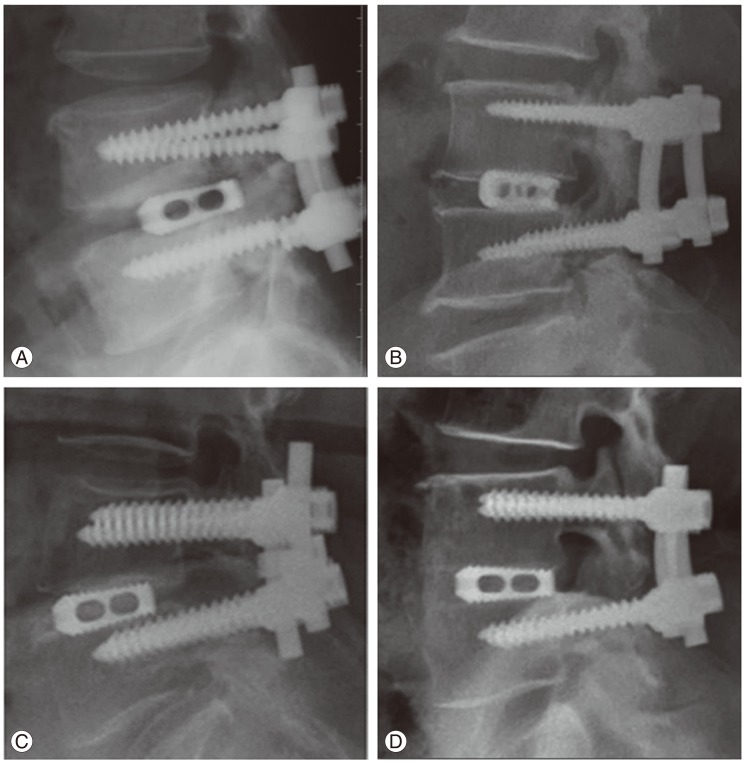
The minimum follow-up was limited to 24 months. A total of 99 cases of 79 patients were legitimate to this norm. Group I was 61 cases (87%) and group II was 38 cases (86%) (Fig. 4). Degree of bone formation was assessed on the final sagittal plain radiography by the 4 grade numeric scale method devised by the senior author. Grade I is no or little bone formation, grade II is bone formation less than 50% of the grafted zone, grade III is bone formation more than 50% of the grafted zone and grade IV is full bone formation of the interbody space, which connects both end plates (Fig. 5). The readers were the same orthopedic doctors with the same condition and same manner as the 6 month computed tomography (CT) assessment. A statistical analysis was conducted by t-test, Fisher's exact test and Likelihood ratio method for the assessment of sampling homogeneity, Kappa test for the concordance between the two readers and Mann-Whitney test for the difference between the two groups. SPSS ver. 16.0 package (SPSS Inc., Chicago, IL, USA) was used.
Results
The demography of the two groups was not heterogeneous (Table 1). The amount ratio of local bone chips and DBM was 6.0:1 in group II. The mean follow up period was 34 months (range, 24-51 months). Surgery related complications and DBM related complications did not develop in both groups. ODI of both groups were improved significantly at the final assessment and there was no difference between the two groups (Table 2). There was a moderate degree concordance between the two readers in sagittal (kappa=0.494, p<0.001) and coronal (kappa=0.467, p<0.001) CT images in preliminary assessment and plain sagittal radiography (kappa=0.57, p=0.000) in the final assessment.
Bone formation at 6 months after surgery was superior in group II. However, there was no significant difference between the two groups at the final assessment (Table 3).
Discussion
The use of bone graft substitutes in spine surgery has been researched and debated. Although auto-iliac bone remains as a gold standard, its potential complications have led to the development of other bone graft options. DBM has been used as one of the alternatives of the auto-iliac bone. DBM has demonstrated an effect on the differentiation of osteoprogenitor cells into osteoblast. Urist [3] first identified an osteoinductive substance, while preparing extracts from the demineralized bone. Since then, the osteoinductivity of DBM has been well established [4,5,6]. DBM is mainly comprised of type I collagen (93%), which provides an osteoconductive surface. Noncollagenous soluble proteins, such as osteoinductive bone morphogenic protsein (BMP) and a cocktail of synergistic proteins (transforming growth factor-beta, insulin-like growth factor, platelet-derived growth factor, fibroblast growth factor) represent 5%. The remaining 2% is made of residual mineralized matrix [7,8,9,10]. In addition to its osteoinductivity, DBM has some degree of osteoconductivity [5].
DBM is combined with other components, so called carrier, intended to make easier to handle and enhance localization. The carrier must be biocompatible with the bone, maintain graft localization and not reduce the osteoconductivity [11]. The first DBM/carrier products were introduced in 1991 and have since become one of the most widely used alternative graft in spine fusion surgery. Even though there are many kinds of growth factor proteins, the osteoinductive ability of DBM largely depends on the activity of BMP [12]. Unfortunately, the production of DBM is loosely regulated by Food and Drug Administration as a minimally manipulated human allograft tissue, with no mandated requirements for the osteogenic growth factors concentration or for the demonstration of osteogenic efficacy. The content of BMP is variable according to the manufacturers and even the different lots of the same manufacturer have variable amounts of BMP. BMP-2 and BMP-7 exist in nanogram concentrations in DBM, which is 1 million times less than the concentration, which is required to produce a lumbar spinal fusion [13]. Herein, it is unavoidable that the amount of osteogenic activity of a particular DBM is highly dependent upon the donor variability [14]. Commercially available DBMs have demonstrated the variability of their osteoinductive potential, which may reflect differences of their BMP content [15]. To avoid variability between the different commercial products, only one product, Allomatrix (Wright Medical) was used in the current study, which is comprised of 86% of DBM and 14% of calcium sulfate hemihydrates as a carrier and electron beam was used for final sterilization.
There have been many animal studies that presented promising results. Several rat studies have demonstrated that DBM can induce a spinal fusion in a dose dependent manner and may have value as a graft substitute, at least as a graft extender [11,15,16]. However, the substances did not perform equally, that some did not demonstrate any significant bone formation. There is also a rat study which noted that DBM is superior to the fresh frozen allogeneic bone in arthrodesis [17]. In a canine study, combination of DBM with autograft achieved more rapid spinal fusion than the autograft alone [6], and in rabit interbody fusion model, composite graft of DBM and hydroxyapatite block showed more rapid and strong fusion than autograft alone [18]. In a study which used more advanced species -nonhuman primate- admitted DBM as a graft enhancer [19].
Despite promising animal data, DBM has been under a lack significant clinical data that support its efficacy in spine fusion surgeries so far. The initial human study on the efficacy of DBM was performed on the anterior cervical spine fusion in which the freeze-dried allogeneic bone augmented by DBM was compared to the auto-iliac bone. This study did not offer sufficient osteoinductivity of the allograft-DBM construct in anterior cervical fusion [20]. There is a study somewhat encouraging, which compared the fusion rates of auto-local bone and DBM constructs to that of the auto-iliac bone alone cases in the setting of PLF. The result that presented no difference between the two groups indicated that it has a value as a graft extender in humans [21].
We performed the current study to verify the graft enhancing ability of DBM. It was considered that a substance that has osteoinductivity should be able to act as a graft enhancer rather than a graft extender. The construct of PLIF with pedicle screws and cages supplies sufficient stability to reduce the contribution of the graft materials. There have been many studies which showed satisfactory fusion rate with local bone chips in PLIF using pedicle screws and cages. Given our own experience, however, nonunion cases have been developed even with such construct. There is a study that said the necessity of an additional graft adjuvant to increase fusion quality and prevent subsidence in the same kind of surgeries [22].
There have been several reports as to the efficacy of BMP and auto-local bone composite graft in TLIF or PLIF [23,24]. Meanwhile, there also have been many studies that noted complications, such as ectopic bone formation [25], radiculitis [26] and vertebral osteolysis [27], which are attributable to BMP in PLIF. To our knowledge, there have been a few reports which noted the graft enhancing effect and complications of DBM when it is used in PLIF with the local chip bone. We thought that PLIF using pedicle screws and unilateral cage augmented with local chip bone is a good model to evaluate the efficacy of DBM as a graft enhancer because that kind of surgery is already proven to have a high fusion rate; therefore, it would be least detrimental even though DBM does not work and the space opposite to a cage would provide good visualization to appraise the quantity of fusion mass. Furthermore, large cancellous surfaces of the vertebral end plates were presumed to act as a instant source of osteogenic precursor cells as mentioned by Bauer and Muschler [28]. According to the study of Wang and Gilmcher [29], the dominant pathway of DBM osteogenesis is akin to endochondral bone formation in the subcutaneous and intramuscular layer; whereas, it resembles intramembranous bone formation in the cranial defect. The authors have suggested that this distinction may result from the mesenchymal stem cells in different position having a predominance of stem cells with different receptors that selectively bind chondrogenic or osteogenic proteins, respectively. The intervertebral space was considered to resemble to a cranial defect; therefore, DBM was expected to work in a more potent way than the intertransverse plane. We applied the 4 grade quantification scales rather than a dichotomous fusion or nonunion to help discriminate the contribution of DBM more delicately.
At first, we planned to assess whether they are fused or not with a simple radiography at 6 months and last follow-up. It was, however, totally impossible to be decided at 6 months. Nearly all cases of both groups were classified as nonunion, same or less than grade II. Therefore, the early assessment was changed to be based on CT findings. Because of the above reason and time constraint (within the time 6 months┬▒2 weeks), CT follow-up rate became significantly lower. For that reason, the result of early assessment was considered to have a meager significance, though it showed early bone formation.
One of the drawbacks of DBM is inconsistent amount of BMP content [13,15]. We expected superior score in group II, despite the large standard deviation. However, the results showed similar average score and standard deviation. Therefore, we concluded that it does not indicate inconsistent osteoinductivity, but unwarrantable osteoinductivity. Sassard et al. [21] reported that DBM acted as a graft extender when it was mixed with auto-iliac bone in 3:1 ratio. In my opinion, that cannot be as an osteoinductive material. It is rather close to osteoconduction, which is attributable to a large amount of collagen and carrier materials.
There are several limitations in the current study. The sample size of the two groups was not similar because those who refused to use DBM were transferred to the opposite group. The follow-up rate of preliminary CT assessment at 6 months was too low to assert a certain conclusion due to the above mentioned reasons. The concordance between the two readers was not strong enough.
Conclusions
DBM did not present a graft enhancing effect when small amount of it was used as a composite graft with the auto-local bone in PLIF using pedicle screws and cages. The early bone forming effect of DBM was not conclusive due to the significant flaw in the early stage assessment. Therefore, DBM is untenable as a graft enhancer universally.