Lumbar Spinal Stenosis: Who Should Be Fused? An Updated Review
Article information
Abstract
Lumbar spinal stenosis (LSS) is mostly caused by osteoarthritis (spondylosis). Clinically, the symptoms of patients with LSS can be categorized into two groups; regional (low back pain, stiffness, and so on) or radicular (spinal stenosis mainly presenting as neurogenic claudication). Both of these symptoms usually improve with appropriate conservative treatment, but in refractory cases, surgical intervention is occasionally indicated. In the patients who primarily complain of radiculopathy with an underlying biomechanically stable spine, a decompression surgery alone using a less invasive technique may be sufficient. Preoperatively, with the presence of indicators such as failed back surgery syndrome (revision surgery), degenerative instability, considerable essential deformity, symptomatic spondylolysis, refractory degenerative disc disease, and adjacent segment disease, lumbar fusion is probably recommended. Intraoperatively, in cases with extensive decompression associated with a wide disc space or insufficient bone stock, fusion is preferred. Instrumentation improves the fusion rate, but it is not necessarily associated with improved recovery rate and better functional outcome.
Introduction
Degenerative joint disease is a degradative process of the joints that primarily involves the articular cartilage [1]. This disease is the leading cause of chronic disability all over the world and usually presents with joint pain, tenderness, stiffness, locking, and effusion [2]. In advanced cases, muscle atrophy, joint instability, or deformity may develop [2,3]. The arthritic changes in the spinal column (spondylosis) with involvement of the facet joints and intervertebral discs, in addition to these common signs and symptoms, may also cause neurologic impingement [4,5].
Degenerative process of the spine is usually divided into three phases; inflammatory, instability, and re-stabilization [6]. Although these arthritic changes are more common in the area with greater mobility and pressure like lower cervical or lower lumbar spine, different stages of arthrosis can be observed simultaneously in one region of the spine [7]. Lumbar spondylosis is not synonymous with lumbar spinal stenosis (LSS), but it comprises the vast majority of these cases [8].
Clinically, the symptoms of patients with lumbar spondylosis can be categorized into two groups; regional (low back pain, stiffness, and so on) or radicular (spinal stenosis mainly presenting as neurogenic claudication) [5,8]. Both of these symptoms usually improve with appropriate conservative treatment [8]. In refractory cases, surgical intervention is occasionally indicated [8,9]. In these review, we present an updated concept for the necessity of fusion in patients with LSS undergoing surgical treatment.
Lumbar Disc Herniation versus Spinal Stenosis
Although traditionally every case of neurologic impingement with involvement of the spinal cord or nerve roots is categorized as spinal stenosis, the patients who present with only intervertebral disc herniation are usually different from those with LSS [10,11]. In these special cases, the only pathologic finding is herniation of the soft disc without any other abnormality in the adjacent facet joints, ligamentum flavum, or bone. These patients are usually younger and the course of the disease is more acute. Positive straight leg raising test, muscle weakness, and other objective findings are usually more common in these patients. These findings are contradictory to those in patients with LSS who have multiple complaints (inability to walk, inability to stand, or interfere with activities of daily living), but usually no positive objective finding can be detected [10].
Which Patients Should Undergo Decompression?
The only well known absolute indication for surgical neurogenic decompression in patients with lumbar radiculopathies is cauda equina syndrome (CES) [12]. Although CES includes a famous triad of bilateral Achilles areflexia, saddle anesthesia, and sphincter disturbances, these findings are observed in only half of the patients [13]. Therefore, the clinicians should not wait too long to observe all the three features of the syndrome. In other patients with signs and symptoms of LSS, a three-month trial of aggressive conservative treatment is usually recommended, but after this time period, surgery has been found to be associated with significant improvement in all primary outcomes [14]. In ordinary LSS, radicular complaints (other than CES) are usually relative surgical indications, even though most of the authors recommend early neural decompression when the radicular pain is present even at rest [15,16].
The primary goal of neurologic decompression is to improve the radicular pain. The surgeon should know that the patients who primarily present with a complaint of low back pain may not show much improvement after decompression only procedures even though a relatively severe stenosis might be detected in the imaging studies [8,15].
Which Patients Should Undergo Spinal Fusion?
The primary goal of spinal fusion is to improve the regional back pain [17]. Spinal fusion is usually achieved by applying autogenous or allogenous bone graft over the decorticated bone surfaces. Instrumentation may be used to improve the fusion rate and to correct the underlying deformity [18]. Instrumentation may increase the fusion rate (especially in multilevel fusion), but it is not necessarily associated with improvement in the recovery rate [19]. Solid radiographic fusion does not guarantee a successful outcome [20]. Favourable outcome is generally achieved by appropriate patient selection.
Appropriate indications for lumbar fusion are usually categorized into two major groups; preoperative and intraoperative indicators. Paying attention to the patient is necessary for making a logistic decision of performing spinal fusion. Before considering these two groups, the clinicians should not forget that in every spinal procedure for achieving spinal fusion, the fusion stage is the most important stage in the whole procedure. If the fusion fails, the world's strongest implant is doomed to fail.
Preoperative Indicators
1. Failed back surgery syndrome
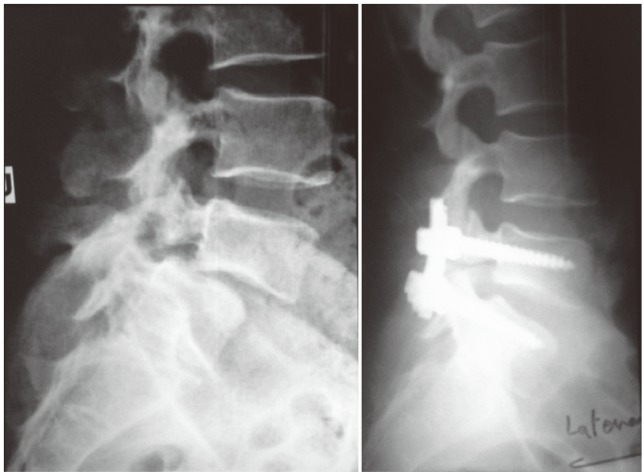
In the patients with a history of previous lumbar surgery who present with instability, deformity (flat back), or recurrence, if revision surgery is found to be necessary, fusion is probably indicated, because revision often requires more resection of the stabilizing structures (Fig. 1) [21]. In those cases in which less invasive techniques were used previously or the previous surgery induced fusion, decompression alone may be sufficient, but instrumentation should be routinely used in the operating room during all revision lumbar surgeries.

A 52-year-old female was treated with decompression and instrumentation 1 year ago. She presented with flat back syndrome, refractory low back pain, and walking disability. During revision surgery, no evidence of fusion was observed, the instrument was removed, and lumbar lordosis was re-created.
2. Degenerative instability
In patients with debilitating lumbar degenerative spondylolisthesis with spinal stenosis, surgery compared to nonsurgical treatment can provide substantial improvement in pain and function at least for a period of two years [22]. It is obvious that fusion is not needed in all of the cases with underlying spondylolisthesis. If decompression surgery in patients with stable low grade degenerative spondylolisthesis does not cause injury to the facet joints, it will not increase the probability of greater slippage relative to its natural history [23]. In patients who mainly present with radicular complaints without significant pain in the lumbar spine, if the spondylotic vertebra was re-stabilized in the slipped position, decompression alone is sufficient. In those cases with significant disc space, and instability on dynamic views (>5 mm displacement or >10°-15° rotation on lateral standing flexion-extension lumbosacral radiographs) in especially those cases with slip greater than 25%, accompanying fusion is also necessary [24,25]. When the chief complaint of the patient is a refractory low back pain and no significant stenosis is apparent on imaging studies, fusion is recommended (without any accompanying decompression) [26].
3. Correction of the deformity
Whenever it is necessary to correct the underlying deformity as well as spinal stenosis, instrumented fusion is needed. Correction of the spinal deformities such as degenerative scoliosis or degenerative kyphosis in elderly patients is a major operation, and it should be performed only in patients who have appropriate indications [27,28,29]. An important principle of spine surgery is that "proceed with less interfere that helps more" and it's better this not to be forgotten at all.
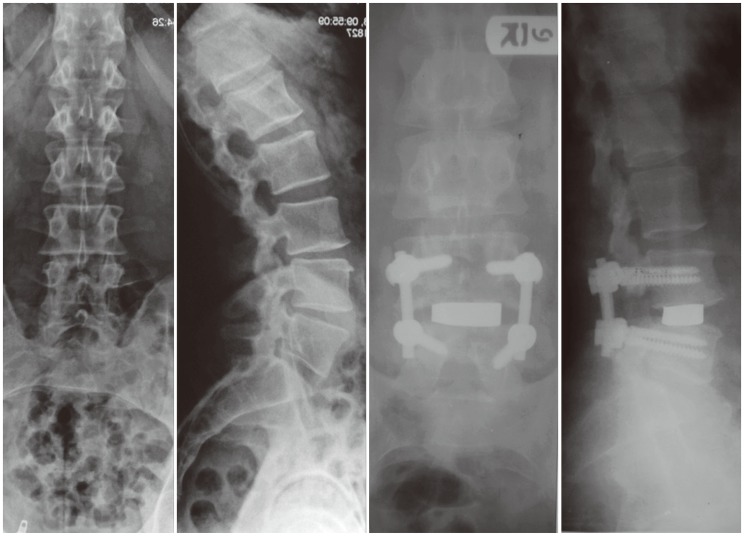
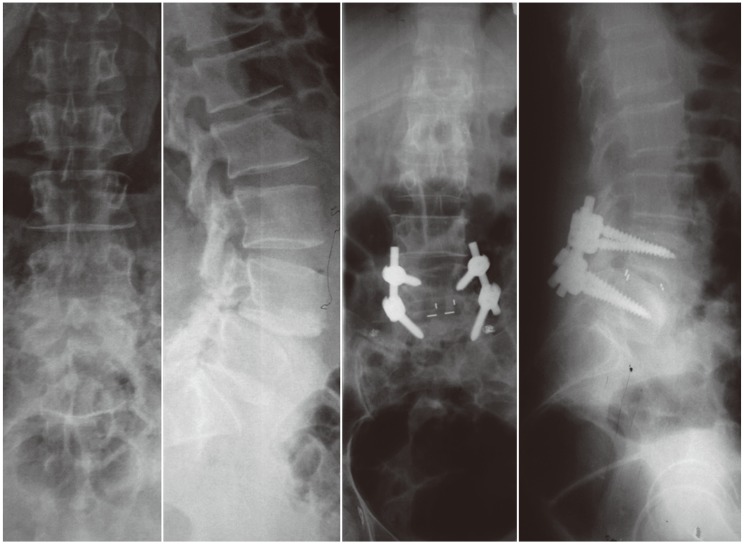
In the refractory cases with significant lumbar degenerative scoliosis (>20°), kyphosis, or spondylolisthesis, when correction of the underlying deformity is intended, instrumented fusion is certainly indicated (Figs. 2, 3) [30,31].

An 87-year-old male patient presented with annoying claudication and low back pain. In preoperative imaging studies, degenerative scoliosis associated with significant stenosis was observed. He was scheduled for neural decompression, deformity correction, and instrumented posterolateral fusion.
A 36-year-old man presented with L5-S1 isthmic spondylolisthesis. He was treated with laminectomy, slip reduction, and instrumented posterolateral fusion.
4. Wide disc space
It is a radiologic landmark that is measured on lateral lumbosacral radiographs, when the radiation beam is perpendicular to the intended disc; an intervertebral disc height of more than two millimeters (versus spondylotic re-stabilized motion segment) is supposed to be one of the predisposing factors for postoperative instability [32]. In these cases, extensive decompression surgery (from pedicle to pedicle) associated with facetectomy can significantly increase the probability of spinal instability.
5. Symptomatic spondylolysis
Spondylolysis is such a common radiologic finding (6% of general population), and some authors consider it as a normal variation like sacralization, lumbarization, or spina bifida occulta [33]. It is not reasonable that all of the lumbar problems should be attributed to the presence of spondylolysis on the radiographs. It should be proved that this condition is the cause of the pain (by injecting local anesthetic agents adjacent to the suspicious area under fluoroscopic control). Only a limited number of patients with spondylolysis finally require surgery.
For surgical treatment of L5 spondylolysis, neither repair (trying to heal the non-united area of the pars interarticularis with local curettage and bone graft) nor instrumentation is usually recommended. Here, the spine is inherently stable and in situ L5-S1 fusion is sufficient [31,34]. However, there are some papers that indicate the possibility of direct repair of L5 vertebra even if a vertebral slippage of 3-4 millimeters is present [35,36].
For L4 spondylolysis, there are two treatment options. In young patients with an intact intervertebral disc, the preferred treatment is repair and instrumentation (without any intervertebral fusion), but in cases with an underlying degenerated disc, fusion is the treatment of choice (Fig. 4) [31,37].
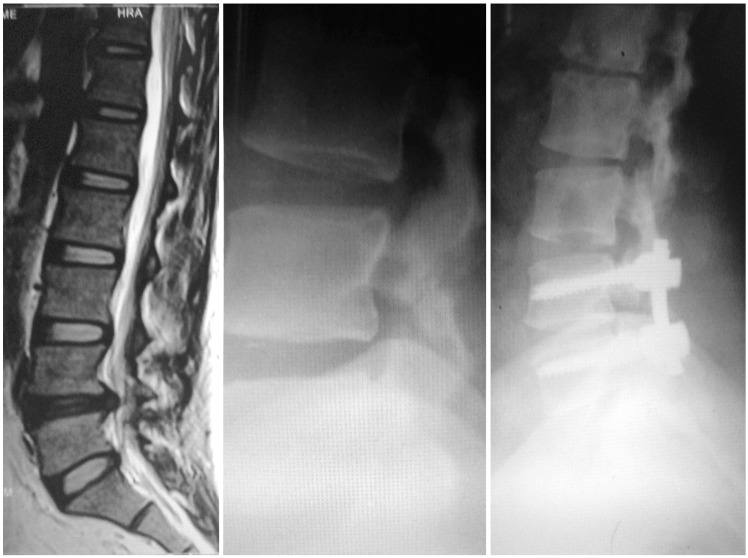
A 32-year-old woman presented with refractory L4 spondylolysis, L4-L5 degenerative disc disease, and L4 radiculopathy. She was treated with decompression, and in situ instrumented fusion.
6. Refractory degenerative disc disease
Some patients may complain of chronic low back pain refractory to routine treatment, even to aggressive conservative treatment. Chronic low back pain is a challenging problem all over the world, and a definite etiology cannot be found in most of the patients [38]. Although in some spinal centers, diagnostic procedures like discography or intradiscal (local anesthetic) injection are carried out preoperatively, these procedures are not routinely performed all over the word and not all of the authors agree with the use of these procedures. Some authors even oppose the use of these measures and believe that discography itself may lead to a degenerative process in otherwise healthy intervertebral discs, and therefore the recently published guidelines do not recommend discography [39,40]. According to a systematic review carried out by Hancock et al. [41], magnetic resonance imaging findings such as endplate changes and presence of disc degeneration were found to increase the possibility of a discogenic origin related to discography. In patients with underlying degenerative disc disease and in whom other pathologies are completely ruled out, spinal fusion especially with an intervertebral cage may be recommended, but the clinicians should remember that these patients are not very good surgical candidates, and therefore, a trial of aggressive nonoperative management for >12 months should be carried out preoperatively, and all secondary gain issues should be sufficiently resolved (Fig. 5) [42,43].
A 42-year-old man presented with chronic refractory low back pain, and a degenerative disc disease in the L4-L5 space. His pain was almost completely eliminated after a trial of local anesthetic injection during discography. He ultimately underwent instrumented transforaminal lumbar interbody fusion. During the latest follow-up visit at 32 months post-operatively, he was completely pain free and could work like an otherwise healthy man.
7. Adjacent segment disease
In the patients in whom the stenotic segments are located adjacent to a previously fused or immobilized segment, neural decompression with instrumented fusion is preferred (Fig. 6). As more stress is concentrated on this segment, even with limited neural decompression, the probability of postoperative instability is high [44].

A 56-year-old female patient presented with L4-L5 stenosis and spondylolisthesis associated with a relatively spontaneous fusion of L5-S1. The instability may be de novo or secondary to the relatively stabilized L5-S1 segment (arrow). She was treated with decompression and instrumented posterolateral spondylodesis.
Intraoperative Indicators
1. Extensive decompression
In the patients who underwent bilateral facetectomy>1/3-1/2, excision more than 50% of the pars interarticularis, bilateral discectomy in addition to partial facetectomy, spinal fusion is recommended [44,45].
2. Available bone stock
For achieving a successful fusion, adequate bone graft on the host bed is needed. To improve the fusion rate, especially in the presence of small transverse processes (for successful posterolateral fusion) or high grade spondylolisthesis (with horizontal versus vertical position of the graft), instrumentation is highly recommended [46]. However, it should be kept in mind that severe osteoporosis is a contraindication of instrumentation due to the high probability of implant dislodgement, and it is recommended that pedicular screws should be augmented with polymethyl methacrylate in these osteoporotic patients [47]. Other known strategies that are recommended for insertion of pedicular screws into the osteoporotic spine include supplementary hook application, screws with longer length and greater diameter, or the effect of screw insertion angle [48,49,50].
What is the Purpose of Using Interbody Cages in the Surgical Treatment of LSS?
Application of interbody cages in spine surgery for achieving lumbar interbody fusion (LIF) is gaining popularity. Complete excision of the intervertebral disc tissues and interbody fusion can significantly improve the discogenic pain. On the other hand, the interbody cage not only restores the normal intervertebral lumbar lordosis, but also increases the likelihood of achieving an appropriate fusion in the weight bearing area of the vertebral body [51]. During the postoperative healing process until solid fusion is achieved, there will be much less stress on the pedicular screws that have already been augmented with interbody cages (less occurrence of implant failure) and postoperative braces can be removed much earlier [52].
Although there are no absolute indications for LIF in LSS, the most probable indications include intractable lumbar discogenic pain, spondylolisthesis (Fig. 7), revision surgeries for recurrent disc herniation, symptomatic pseudoarthrosis, et cetera [53,54,55,56].
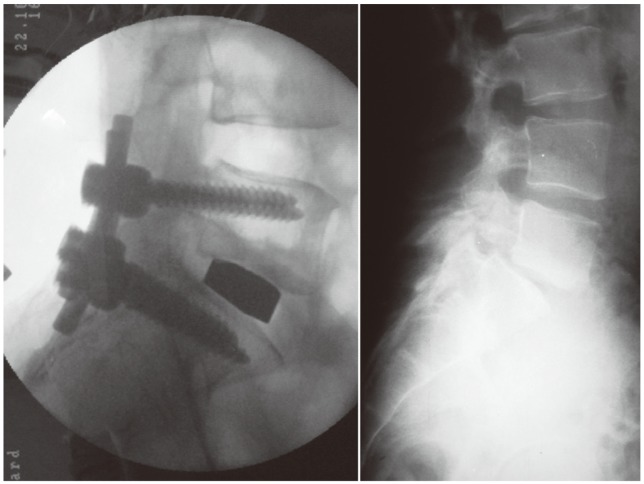
A 35-year-old man presented with L5-S1 isthmic spondylolisthesis (grade II), severe low back pain, and right leg pain since six months. He was treated with slip reduction, TLIF cage, and instrumented posterolateral fusion. Right image shows the intraoperative fluoroscopic lateral view of the lumbosacral area. TLIF, transforaminal lumbar interbody fusion.
Anterior LIF by restoring the intervertebral height and unfolding of the ligamentum flavum indirectly decompresses the spinal canal, and therefore, it may be useful in mild or moderate central LSS [57]. In severe stenosis, especially in cases with lateral recess or foraminal stenosis, direct decompression of the neural elements is necessary. Posterior LIF (PLIF) (Fig. 8) and transforaminal LIF (TLIF) (Fig. 7) are two modalities for the application of intervertebral cages via the posterior approach. Nowadays, extreme lateral LIF (XLIF) and axial LIF have also been described and they have some specific novel advantages [53].
A 54-year-old woman presented with clinically debilitating L4-L5 spondylolisthesis. For surgical treatment, vertebral reduction, instrumented posterolateral fusion, and posterior lumbar intervertebral fusion were performed.
There is an important issue that is worth remembering. In lumbar spine surgery, a stand-alone cage (either via the anterior, posterior, or lateral approach) is not an acceptable spinal procedure [58]. The lumbar cage acts as a scaffold for promoting bone ingrowth. It does not work as a non-fusion technique, cannot provide any segmental stability, and therefore, it should be supported by some types of stabilizing devices. Favorable clinical outcome depends on achieving a solid intervertebral spondylodesis.
Non-fusion Techniques for Treatment of LSS
Recently, numerous stabilizing devices have been introduced in the spinal arena. Common features of these non-fusion (dynamic stabilizing) implants include retention and protection of the intervertebral disc and most of the soft tissues and bony structures of the posterior spine, application of minimally invasive technique, short operative time, earlier surgical intervention, preservation of the motion (versus fusion), and therefore a reduction in the probability of adjacent segment disease [59]. These devices may be used alone or in combination with other decompression surgeries. They are categorized as interspinous process spacers (like X-Stop, Device for Intervertebral Assisted Motion [DIAM], Interspinous Posterior Device [IPD], et cetera) or pedicle-based systems (like PercuDyn, or Dynesys). These devices fairly distract the intervertebral space, reduce stress on the affected segment, and may provide a better environment for recovery of the spine. They are not proven to be completely effective, but they are usually safe and do not jeopardize other therapeutic options in the event of failure [59].
Minimally Invasive Surgery for LSS
Nowadays, a large proportion of spinal surgeries are carried out using minimally invasive techniques. These techniques preserve the neural and vascular supply of the paravertebral muscles (especially multifidus), and therefore they significantly facilitate postoperative rehabilitation and recovery [60]. Currently in the case of spinal stenosis surgery, numerous operations such as TLIF, PLIF, XLIF, multilevel decompression, and multiple instrumentations can be easily performed using these techniques and minimal tissue dissection [61].
Conclusions
Fusion of the lumbar vertebrae not only prevents the movement of mobile vertebrae but also increases the stress on the adjacent intact segments. In appropriately selected patients, fusion can stabilize the unstable lumbar vertebrae and also eradicate the source of pain originating from the diseased intervertebral disc or facet joints. Instrumentation may improve the fusion rate, but it is not necessarily associated with improved recovery rate. To achieve a favorable outcome after spine surgery, a perfect surgery in appropriately selected patients is necessary.
Acknowledgments
The author would like to thank Dr. Shahrzad Ariamanesh, MD for her valuable comments while reviewing and revising this manuscript.
Notes
No potential conflict of interest relevant to this article was reported.