Introduction
Spinal stenosis classically presents with neurogenic claudication. Patients typically complain of leg pain that is exacerbated with extension of the spine, while flexion relieves the symptoms. Atypical presentations of spinal stenosis have been described, including intermittent priaprism [1,2] and a bilateral foot drop [3]. The purpose of this study is to highlight an atypical presentation of spinal stenosis presenting as scrotal and perianal claudication, and discuss the approach to management
Case Report
A 63-year-old Asian male with no significant past medical history presented to our clinic with a 12-month history of progressive perianal and scrotal claudication. He had minimal back pain. The patient was very disabled by the claudication in his perianal and scrotal region. He was unable to stand or walk for more than 5 minutes, and had to sit or lean forward to relieve his symptoms. He denied symptoms of leg claudication or bowel and bladder dysfunction. Neurological examination of the spine revealed no back tenderness and a good range of motion. Power at all myotomes was full (Medical Research Council grade 5). Sensory examination was normal. Reflexes were normal with down going plantars. The numbness was localized to the perineum/scrotal region. Peripheral pulses were present and a digital rectal examination performed was unremarkable.
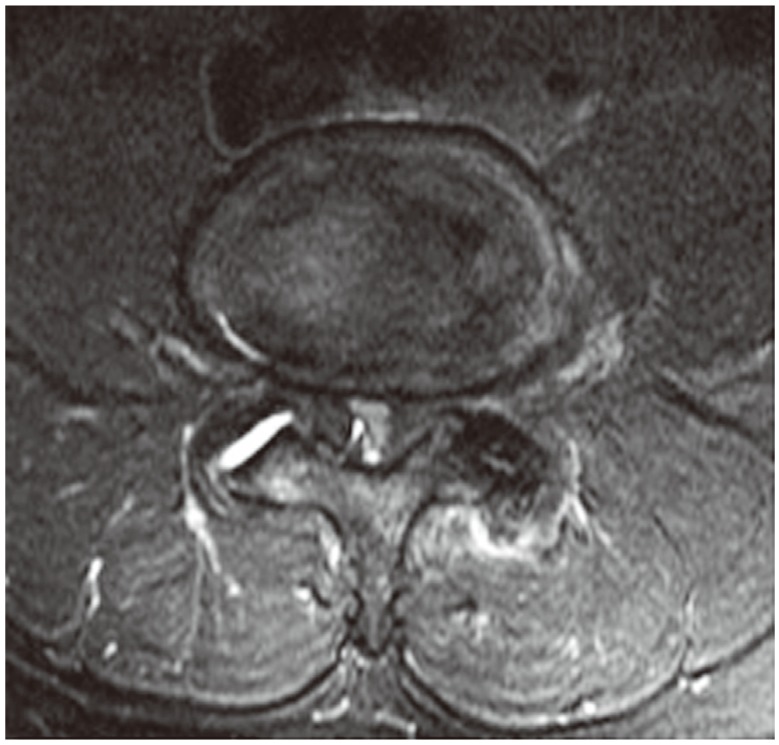
Radiographs showed lumbar spondylosis with a grade 1 spondylolisthesis at L3/L4, and L4/L5 (Figs. 1, 2). magnetic resonance imaging (MRI) revealed severe disc degeneration at L3/4 and L4/5 with severe central canal stenosis, worse at L4/L5, with compression of the cauda equina (Figs. 3, 4). A referral to the Urologist was also made to exclude other urogenital causes but the tests were unremarkable. This included a physical examination, urodynamic testing and an ultrasound. In view of the patient's progressive symptoms and radiological findings, a decompression and fusion of the L3/4 and the L4/5 levels were performed for the patient's spinal stenosis. The surgery was uncomplicated.
Postoperatively, the patient recovered well with immediate resolution of his symptoms. At his 12-month follow up, his scrotal and perianal claudication had not recurred and he was able to exercise again, walking up to 1 hour a day.
Discussion
Spinal stenosis was first described by Verbiest [4] in 1954, classically presenting with discomfort in the thighs, calves and feet on walking. The pathophysiology of neurogenic claudication in lumbar spinal stenosis has been well described. This is believed to arise from ischemia of the lumbosacral nerve roots, as a result of increased metabolic demand during exercise. There is also co-existing vascular compromise of the nerve roots due to pressure from surrounding structures [5].
Our patient presented with atypical symptoms of spinal stenosis, with predominantly scrotal and perianal claudication, in the absence of leg claudication. Apart from the location, these symptoms were consistent with neurogenic claudication-relieved by squatting and sitting and aggravated with standing and walking. The MRI also confirmed spinal stenosis at the levels of L3/L4 and L4/L5. Atypical presentations of spinal stenosis have been described, including intermittent priaprism [1,2] and a bilateral foot drop [3]. To the best of our knowledge, spinal stenosis causing scrotal and perianal claudication has never been reported.
Fraser et al. [6] reported that cauda equina syndrome might present in a variety of ways. This includes bladder and bowel dysfunction, pain, sexual dysfunction, and neurological deficits in the lower limbs. Of these, saddle anaesthesia was found to be the most striking feature of cauda equina syndrome, which is the result of damage to the sensory nerves at the cauda equina. Due to the similarity of dermatomal distribution and complete resolution of symptoms after surgery, we believe that this atypical presentation of spinal stenosis may suggest severe cauda equina compression.
In conclusion, atypical presentation of spinal stenosis should be considered when a patient presents with perianal and scrotal claudication, even in the absence of leg claudication. An MRI is useful to confirm the diagnosis. This rare symptom may be a sign of severe cauda equina compression and we recommend decompression with predictable good results.