Introduction
Thoracolumbar burst fracture is one of the most common traumatic injuries of the entire human spine and as such, there is always some debate around the indications of operative treatment [12] as well as the optimal method of surgery for this type of fracture. The anterior approach and instrumentation, once considered the gold standard for restoring the weight bearing capacity of the fractured vertebra, has several drawbacks including being time consuming, a difficult technique, demanding as well as posing potential risks of major vascular damage [34]. With remarkable improvements in instrument quality, the posterior approach alone can obviate the need for reconstruction of the anterior and middle columns of the fractured vertebra. The short segment posterior instrumentation and fusion is the current trend as it can reduce the blood loss, preserving segmental motion with an acceptable anatomic and functional outcome [5678910111213]. However, there are also reports of high percentages of instrumentation failure [1415].
We performed short segment posterior instrumentation and fusion treatment on fractured vertebra with reinforcement by pedicle screw augmentation for almost every case of thoracolumbar burst fracture. The purpose of this retrospective study is to evaluate and analyze the radiological outcome of this technique.
Materials and Methods
1. Study population
From January 2006 to July 2012, a total of 31 fresh thoracolumbar (T11 to L2) burst fracture patients (21 males and 10 females) with an average age of 48.0 years (range, 15-77 years) were treated surgically. All patients underwent plain X-rays, computed tomography (CT), magnetic resonance imaging (MRI) and neurologic examination by spine surgeons at the time of admission. All patients were treated with short segment posterior instrumentation and fusion and were monitored for at least 12 months. All patients had neurological complications following surgery.
All patients were evaluated using comprehensive AO classification for thoracolumbar fracture [16] and load sharing classification [17].
This study was approved by our institution review board and informed consent was obtained from all patients.
2. Surgical methodology
We performed emergency operations on patients within a couple of hours following admission. Patients were positioned prone on the Jackson frame in order to reduce the intra-abdominal pressure and to create a positional reduction effect on the fracture site. Conventional longitudinal incision at the midline was routinely used to expose one level above and below the fractured vertebra. Care was taken to protect the surrounding soft tissue from exposure to and damage by the pedicle screw. Posterior fusion was performed with local bone harvested by the spinous process without laminectomy decompression even when the stenotic degree of the spinal canal was more than 50% of its normal value. Reduction of the retropulsed fragment was performed indirectly by distraction of connecting rods.
The rehabilitation program was started the day after surgery. External fixation using orthosis was prescribed for patients during 3 months postoperatively.
3. Radiological evaluation
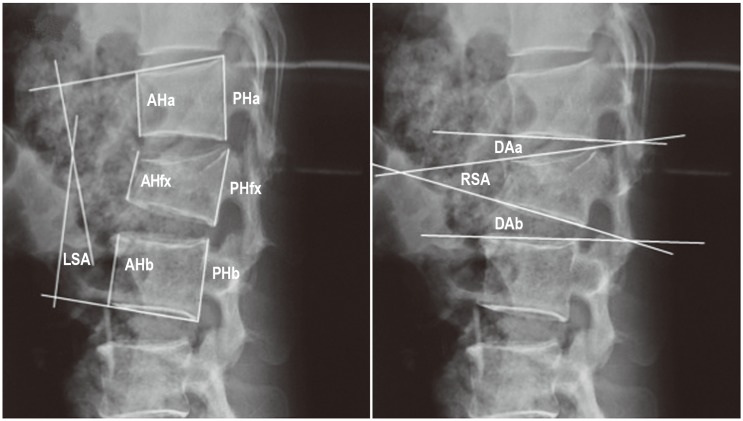
The radiological parameters include local sagittal angle (LSA), regional sagittal angle (RSA), disc angle (DA-designated DAa if above the fractured vertebra and DAb if, below the fractured vertebra), anterior edge height of vertebra (AH-designated AHa if above the fractured vertebra, AHfx for, the fractured vertebra and AHb if, below the fractured vertebra), posterior edge height of vertebra (PH-designated PHa if above the fractured vertebra, PHfx for, the fractured vertebra and PHb, if below the fractured vertebra) (Fig. 1). We defined DA as (DAa+DAb)/2, % AH as {AHfx/[(AHa+AHb)/2]}, and %PH as {PHfx/[(PHa+PHb)/2]}.
These parameters were taken at the time of admission, postoperation and final observation. At the final observation, we took functional plain X-rays (flexion and extension lateral views) for screening the dynamic instability of the fracture site-indirect sign of non-union and implant failure. We evaluated the instability of the fracture site based on the criteria of poor outcome widely accepted for radiological outcome evaluations which include a correction loss of more than 10° of the LSA value at the final observation compared with postoperation, pedicle screw(s) or rod(s) breakage, any sign of pedicle screw loosening (persistence of radiolucency outline of the screw at the final observation) or pulled-out screw and more than a 5° change in LSA with flexion and extension views (ΔLSA) at the final observation.
4. Statistical analysis
Data were analyzed using the program STATA ver. 12 (StataCorp LP, College Station, TX, USA). Mann-Whitney U-test, Student t-test, Kruskall-Wallis test and Spearman's rank correlation test were used for statistical analysis. A p-value of less than 0.05 was considered statistically significant.
Results
1. Demographic
The mean follow-up duration was 22.7 months (range, 12-48 months). The male:female ratio was approximately 2:1. The most affected vertebra was L1 (19 cases), followed by T12 (12 cases). There were 12 cases of A 3.1, 9 cases of A 3.2 and 9 of A 3.3 based on the comprehensive classification of thoracolumbar fracture [16]. The mean load sharing classification score [17] was 5.3 (range, 3-8).
2. Radiological evaluation
The mean LSA, RSA, DA, %AH, and %PH are presented in Table 1. All of the parameters, except DA, were significantly improved after surgery but all of the parameters except %PH were significantly deteriorated at the final observation when compared with postoperation.
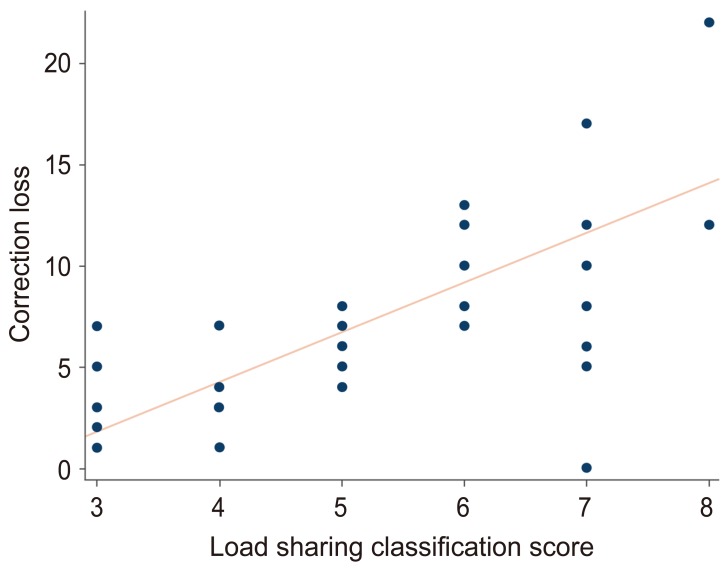
ΔLSA showed no significant correlation with either sex or age (p=0.23, 0.59, respectively). Also, no significant correlations were observed between ΔLSA and the level of injury or the AO classification (p=0.87 and 0.81, respectively). However, a strong correlation was observed between ΔLSA and the load sharing classification score (p=0.0001; Spearman's rho=0.64) (Fig. 2).
For the radiological outcome evaluations which indicate the instability of the fracture site, the radiographic results of short segment instrumentation are presented in Table 2. 71.0% of the patients satisfied the criteria for good radiographic outcomes while 29.0% failed to increase LSA by more than 10° and/or had screw/rod breakage. There were no subjects who demonstrated screw loosening or dynamic instability evaluated by ΔLSA.
Table 3 shows the correlation between the radiological outcome and the load sharing classification score. A load sharing score of more than 7 points tended to demonstrate the failed radiological outcome with an odds ratio of 12.67.
Discussion
In the early era of spinal instrumentation, posterior approach alone was proven to be inadequate for maintaining stability of the injured spine and yielded poor results in both the anatomical and functional aspects [8111415]. However, with the development of metallurgic technology and instrumentation design, pedicle screws nowadays seem to obviate the need for anterior approach.
Long segment instrumentation is strong enough to stabilize the spine. However, the fused spine becomes less flexible and more susceptible to low back pain. Therefore, short segment posterior instrumentation is thought to be a better option able to stabilize the fractured vertebra efficiently. It is also a simple technique and allows for more segmental motion of the spine. Age, osteoporosis and degree of comminution of the vertebral body are risk factors for poor surgical outcomes [910].
In our study, kyphotic deformity was corrected to a considerable extent with posterior instrumentation and indirect reduction. However, the correction of kyphotic deformity which was evaluated by LSA and RSA was gradually lost during the follow up period. Although the indirect reduction by ligamentotaxis had a positive effect on the wedging deformity of the fractured vertebra, preservation of the correction might be difficult. The large bone defect created inside the fractured vertebra after height restoration had been speculated to be the most important cause of that correction loss. Moreover, the evolution of the intervertebral disc height may contribute to the loss of kyphotic correction. During the correction maneuver, the distracting effects by ligamentotaxis influenced mainly the bone, not the discs as the disc angles did not change after reduction. At the final observation, both the disc angles and the disc heights decreased in value. Several authors reported similar observations and it is believed that this decrease correlates with the post-traumatic degeneration of the discs above and below the fractured vertebra [1819].
In our results, the correction loss and the load sharing score had a strong correlation and a load sharing classification score of more than 7 points tended to demonstrate the failed radiological outcome with an odds ratio of 12.67. These results affirm previous studies [1520] that have shown that a load sharing classification score of more than 7 points is an important risk factor in the development of losing initial anatomical restoration.
McLain et al. [15] recorded 52.5% of poor postoperative radiological results in their research and suggested that short segment instrumentation may be inadequate for thoracolumbar burst fracture treatment. On the other hand, Lee and Sung [13] reported only 12.5% of poor results in their study. We believe that our results satisfied an acceptable percentage (29.0%; 9 cases out of 31) of poor radiographical outcomes. All of these 9 cases of poor results demonstrated instrumentation failure in the caudal pedicle screws. In 8 cases with correction loss of more than 10° at the final observation, the upper screws were almost in good positions. The caudal screws, on the other hand, sank downward into the vertebral body or were partially pulled out. Other cases with broken screws were also observed at the caudal screw. There are few reports focusing on whether the cranial or caudal pedicle screws have a higher risk of instrumentation failure. Our results suggest that the caudal pedicle screws might have a higher risk of instrumentation failure than the cranial screws. The thoracolumbar spine is the junction between the less flexible thoracic spine and the more flexible lumbar spine. In the majority of cases, the cranial pedicle screws were inserted at T12, and the caudal screws at L2. The caudal pedicle screws might receive further sharing force than the cranial screws, therefore, caudal screws might exposed to a higher risk of failure. Based on our results, the subjects with load sharing classification scores of more than 7 points should extend their internal fixation using instrumentation (pedicle screws or offset hooks) to caudal segments. Even subjects with load sharing classifications of less than 7 points should adopt longer length and wider diameter of screw for the caudal pedicle screws.
The radiological outcomes do not always correspond to the clinical outcomes. The relationship between radiological findings and clinical outcomes is still a matter of discussion. Therefore, using this investigation as a pilot study, further research involving a larger patient population and long-term follow-up may help resolve several issues left unanswered.
Conclusions
Loss of kyphotic correction after surgical treatment of thoracolumbar burst fracture by short segment instrumentation is common and has a close correlation with the degree of comminution of the vertebral body. Patients with high load sharing scores are more susceptible to correction loss and postoperative kyphotic deformity than those with low scores.