Introduction
Tuberculosis is the second greatest cause of mortality worldwide due to a single infectious agent [1]. Almost a third of the entire population today has latent tuberculosis (TB), i.e., infected but asymptomatic. In 2012, 8.6 million people fell ill with TB and 1.3 million died from TB. Pakistan ranks fifth among the high burden countries (HBCs) and fourth among multi drug resistant (MDR) HBCs and accounts for 61% of the TB burden in the World Health Organization Eastern Mediterranean Region [1]. The estimated prevalence of the disease is 350/100,000 and mortality is 33/100,000 [2].
Potts disease or spinal tuberculosis is one of the most crippling manifestations of extra-pulmonary tuberculosis. Approximately 10% of all extra-pulmonary cases of tuberculosis have skeletal involvement [3] and the spine is affected in half of these patients [4]. The lesion most frequently involves the thoracic spine (45%-50%) and the lumbar spine (40%-45%) [5]. The spine is usually affected through lymphatic spreading of the bacteria when the primary site might have turned quiescent [6] or from hematogenous seeding [7].
Though the clinical presentation may be highly variable depending on the site of the lesion [7], back pain is a consistent finding. Other symptoms include systemic manifestations (weight loss, fatigue, fever and malaise), neurological symptoms (weakness, paresthesia, numbness, bowel symptoms) [5789] and structural deformity (gibbus, kyphosis) [58]. Laboratory investigations include deranged erythrocyte sedimentation rate (ESR) and C-reative protein (CRP) levels, another consistent finding. Imaging modalities used include plain radiographs, computed tomography (CT) scan and magnetic resonance imaging (MRI). Findings include discitis, paraspinal and prevertebral abscesses, collapse and compression.
Radiological findings are often non-specific, thus non-diagnostic and fail to provide a prognostic perspective if the disease is established. Therefore, a bacterial and/or a histological evidence must be obtained to distinguish one infection from another, or from a neoplasm [10]. Localization using percutaneous CT-guided biopsy, introduced in the 1970s, is believed to be the single most accurate method for performing biopsies [1112] and is now routinely used in the diagnosis of spinal lesions [131415161718].
Due to the lack of image guided biopsy centers and the high prevalence of the disease, most of the patients are diagnosed and treated on clinical grounds. This practice was thought to lead to a delay in the diagnosis of other pathologies and MDR TB. The Aga Khan University Hospital is one of the few centers where percutaneous CT-guided biopsy is available. We therefore decided to evaluate our use of CT-guided biopsy and its effect on the management of Potts disease at our center.
Materials and Methods
This was a retrospective observational study conducted at the Neurosurgery section of Aga Khan University Hospital (AKUH) Karachi. AKUH is a Joint Commission of International Accreditation accredited, International Organization for Standardization) certified, tertiary care hospital with over 43 specialties. Potts disease is treated by a multidisciplinary team consisting of members from Neurosurgery, Infectious Diseases and Radiology Departments. The duration of this study was 7 years (2007-2013). The review of medical records was done over three months (January to March, 2014).
1. Patient selection
All the patients with suspected Potts disease who underwent CT-guided biopsy at the Aga Khan University Hospital during the study period were included in the study.
2. Technique
Radiology of the patients was reviewed by consultant radiologists for feasibility of the procedure. Patients with lesions located anterior to the cord or vertebral bodies did not undergo the procedure. The procedures were performed by 4 different Interventionists using similar techniques as described below. The biopsy route was planned to avoid neurovascular bundles and uninvolved tissue compartments.
The procedure was mostly performed in the prone position. Short bursts of intermittent CT fluoroscopic screening were used to reduce radiation dosage to the patient. Following preliminary axial CT scanning, the most appropriate slice was selected for directing the needle into the lesion. In the case of multiple lesions, the largest and most superficial lesion was chosen. Any soft tissue mass related to the bony lesion was also biopsied and aspirated whenever possible.
3. Data collection
The medical records of the selected patients were pulled out of the medical records room. A pro forma was developed and pre tested before final data collection. The pro forma included such variables as age, gender, symptoms and their duration as well as radiological and clinical features of the disease. Details of the procedure, its complications and information on the requested microbiology and histopathology were also part of the pro forma. We retrieved the radiological images of all patients through Hospital Patient Inquiry to record the radiological features at presentation. We used the same software to record serological markers of ESR and CRP. We pilot tested the pro forma for correct recording of variables. Hospital records were consulted for treatment and follow up progress. We used SPSS ver. 17 (SPSS Inc., Chicago, IL, USA) to record all the data.
Results
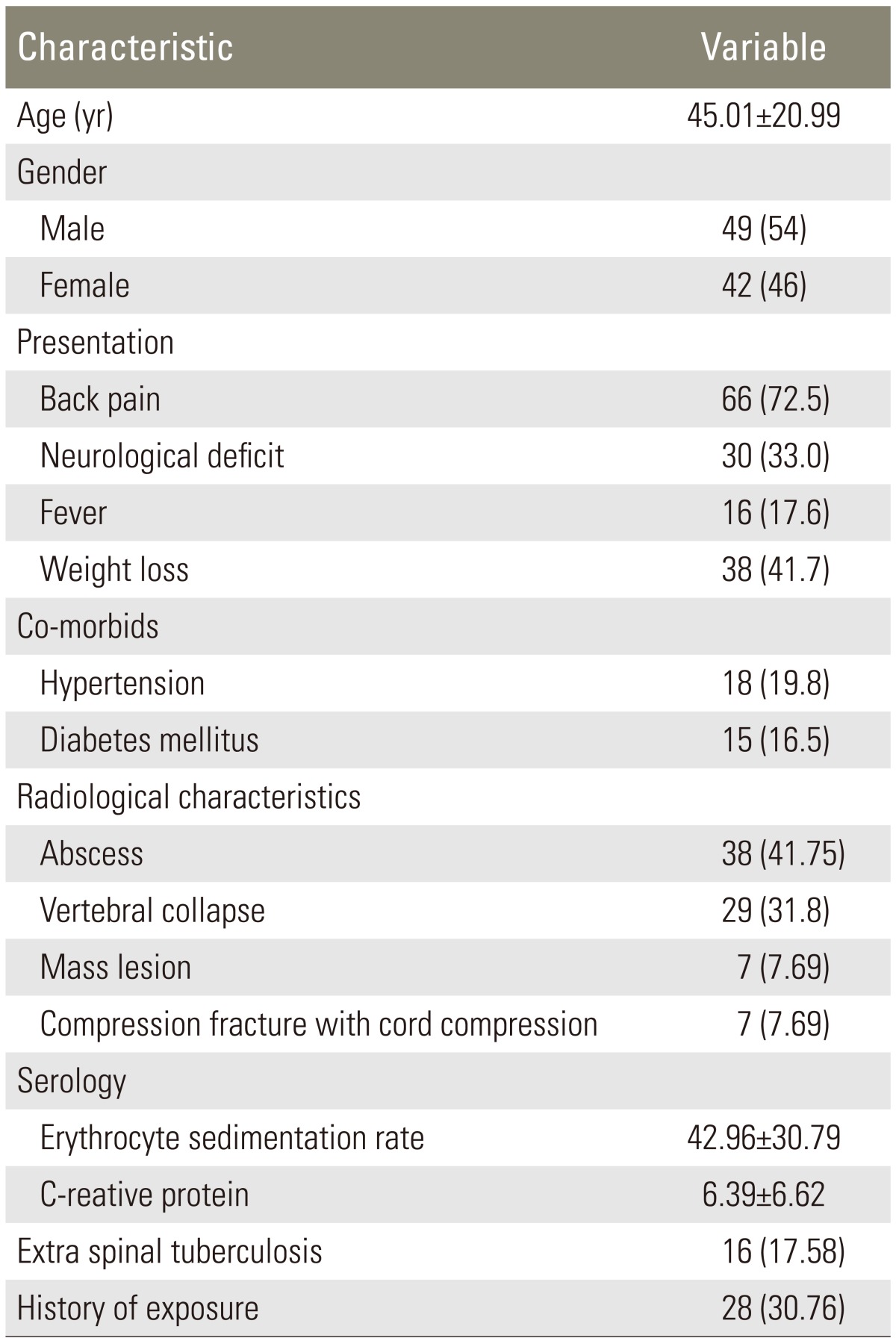
178 patients were treated for suspected Potts disease during the study period. CT-guided biopsies of the spinal lesions were performed in 91 patients (51.12%). There was no preponderance of either gender (Table 1). Majority of the patients presented with back pain and had significant elevations of ESR and CRP (Table 1). Other demographic and clinical characteristics of patients are given in Table 1.
On imaging, 38 patients (41.75%) had abscesses and 7 (7.69%) had mass lesions (Table 1).
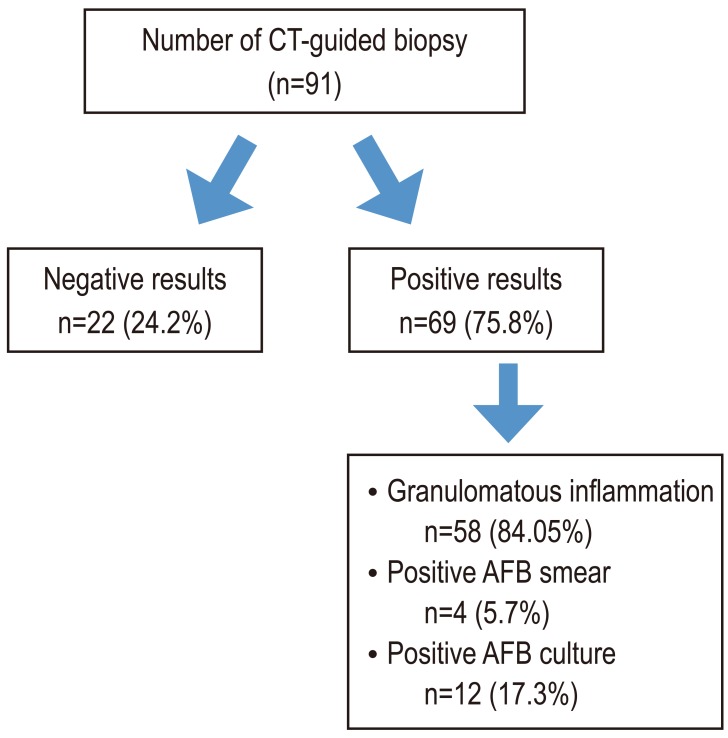
Of the 91 procedures, 22 (24.2%) were inconclusive because of inadequate sample (10), normal tissue (6) or reactive tissue (6). 69 biopsies came back positive (75.8%) (Fig. 1). The results of the procedure are presented in the flow diagram in Fig. 1.
We had a mean follow up of 14.7±7.8 months. The response to antituberculosis therapy (ATT) was determined by the infectious disease team on the basis of ESR, CRP, clinical and radiological features. All 91 cases in which CT-guided biopsy was performed responded positively to ATT. Among the remaining 87 cases in which CT-guided biopsy was not performed, 80 cases responded positively to ATT.
Only 2 patients (2.1%) had a hematoma at the procedure site.
Discussion
Potts disease is diagnosed on the basis of clinical and radiological data [19]. We treated 49% of the patients without biopsy in this series. But with the emergence of resistant strains it is being recommended that a biopsy be performed whenever possible. Diagnostic yields of CT scan guided biopsies for Potts disease differ. We got a positive answer in 75.8% of all the cases where a CT-guided biopsy was performed. However all the patients with a positive diagnosis had Potts disease. Francis et al. [20] reported the best results in literature so far, (82%) but their study had a comparatively small sample size of 29. The discrepancy in success rates has been attributed to accessibility of the lesion, the operator's technique and experience and the number of microbacteria and Langarhan giant cells in the specimen (Sp. Nature) [21]. The current study is the largest case series assessing the diagnostic value of procedure. In a systematic review, Colmenero et al. [19] reported positive histopathology results ranging from 29% to 100%.
Positive acid-fast bacillus (AFB) cultures were seen in 13.2% of cases. The percentage of positive AFB smear was 4.4%. These values are the lowest in reported literature. The percentage of positive AFB cultures ranged from 50% to 83% with an average of 66.2% and the percentage of positive AFB smears on Potts disease samples ranged from 30% to 57.5% with an average of 37% [19].
As noted above, the discrepancy in the success rate is probably due to the accessibility of the lesion, the operator's technique and experience and the number of microbacteria and Langham giant cells in the specimen. Both microbiology and histopathology are recommended on tissue samples obtained through CT-guided biopsy. Bacillary population is lower in samples of tuberculosis obtained from extra pulmonary samples when compared to pulmonary disease [19]. Micrscopic examinations for Mycobacterium tuberculosis were positive 36% of the cases [1922] or less. Our study had the lowest number of positive microscopic examinations (4.4%). This raises the question as to whether every sample obtained through CT-guided biopsy should be sent for microscopic examination.
All the patients who had positive histopathological and microbiological results responded to ATT. Although all granulomas are not tuberculosis, the patients who were treated with ATT responded well.
The rate of complications in CT-guided biopsy for spinal lesions vary from 0% to 10%. In our study two patients had local hematoma that was managed conservatively. Every patient was screened for any coagulation derangement by a prothrombin time and activated partial thromboplastin time. The procedure was not performed on patients with deranged coagulation parameters.
The study however has several limitations. It was a retrospective study with an inherent bias of patient selection. Lesions were heterogeneous in location and had diverse clinical presentations. The procedures were performed by different interventionists and different pathologists were involved. However, the study presents 7 year results from an established neurosurgical center in an endemic area. The results are comparable to available data and encourage the use of CT-guided biopsy.