Introduction
Low back pain (LBP) is a common problem, causing both morbidity and socioeconomic loss [1], with a lifetime incidence rates 50% and 90%, respectively. LBP recurrence rates are reported to be up to 90%, even though many cases are self-limiting and require minimal treatment [2]. Prolonged sitting is generally accepted as an important risk factor for LBP and it is frequently suggested that a lordotic posture should be maintained in the lumbar spine while sitting [34].
Sitting on a chair is one of the most common positions for humans. US children and adults spend approximately 55% of their working hours or 7.7 hours/day in sedentary postures [5]. Sitting may contribute to flattening of the lumbar curve and an increase in intradiscal pressure [6789]. Keegan [6] found that using a lower back support can prevent the flattening of the lumbar lordosis (LL) upon sitting. The use of a lumbar support also reduces intradiscal pressure and the myeloelectric activity in the posterior paraspinal muscles [1011].
The relationship between the pelvis and the spine has previously been overlooked as a contributor to sagittal balance. In particular, it is now recognized that spinopelvic alignment is important for maintaining an energy-efficient posture for both normal and disease states [121314]. However, there have been few studies regarding changes in spinopelvic parameters in the sitting position.
Therefore, the purpose of this study was to find the ideal sitting position by measuring the changes in LL and pelvic parameters in various sitting positions.
Materials and Methods
1. Study design and participants
We undertook a prospective experimental radiographic study in our hospital. All participants were healthy volunteers with Institutional Review Board approval (ED11096).
All participants (thirty male), who agreed to participate in this study provided written informed consent. All participants were volunteers and met the following criteria: no history of chronic LBP or spinal surgery and no radiographic abnormality detected prior to or during the study. Hip, knee, and, ankle abnormalities were ruled out by clinical examination. Demographic data, including age, weight, and height were recorded. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of the height in meters.
2. Radiographic measurements
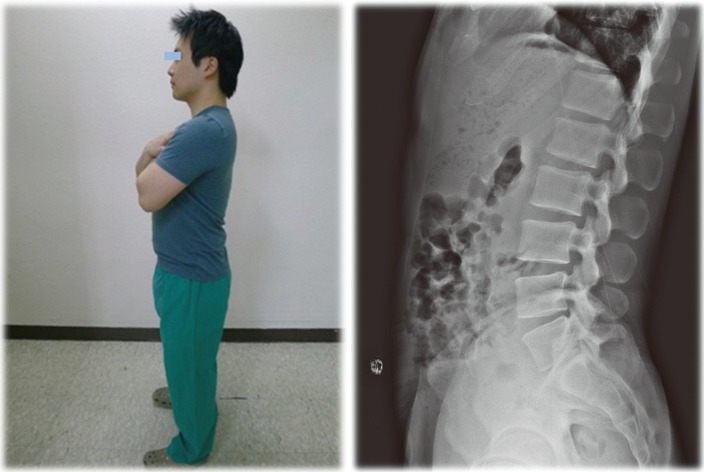
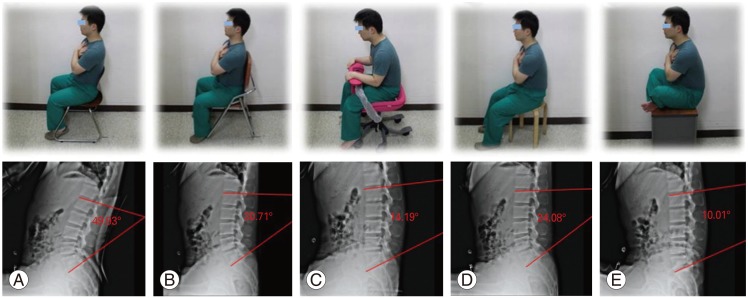
For each participant, a lateral lumbosacral radiograph was obtained using a vertical 30 cm├Ś90 cm film, while maintaining a constant distance between the subject and the radiographic source. The radiograph was centered on the third lumbar vertebra and was obtained during inhalation. Six radiographs, including the hip joint, were taken: one in standing and five in sitting positions. In the standing position, the subject stood in a comfortable position with the knees fully extended and the shoulders flexed 30┬░ (Fig. 1). Five sitting postures with shoulder flexion at 30┬░ were evaluated, which is very common in everyday life (Fig. 2). According to Marks et al. [15], shoulder flexion of 30┬░ is the best position to use for a lateral radiograph to allow repeated measurements of the sagittal vertical axis.
The five sitting positions were as follows: (1) sitting on a chair with lumbar support accommodating the subjects' lower spine curvature; (2) sitting on 90┬░-angled chair; (3) sitting on a chair with anterior support; (4) sitting on a stool; (5) sitting cross-legged.
On each lateral lumbosacral radiograph, two spinal parameters were measured (Fig. 3). The LL is defined as the angle between the cranial end plate of L1 and the cranial end plate of S1 [816]. Lumbar segmental lordosis (LSL) was measured from L1-2, L2-3, L3-4, L4-5, and L5-S1 using the Cobb's method.
Three pelvic parameters, including pelvic incidence (PI), sacral slope (SS), and pelvic tilt (PT), were measured on lateral radiograph (Fig. 4) [17]. The PI is defined as the angle between a line perpendicular to the middle of the cranial sacral end plate and a line joining the middle of the cranial sacral end plate to the center of the bicoxofemoral axis (the line between the geometric center of both femoral heads). The SS is the angle between the horizontal line and the cranial sacral end plate tangent. The PT is the angle between the vertical line and the line joining the middle of the sacral plate and the center of the bicoxofemoral axis. Whole spine radiographs without markings were independently submitted in random order to each of the three observers. Each observer conducted the measurement twice and all mean values of three observers were collected. All measurements were carried out using computer-based digital radiograms on a picture-achieving computer system (PiViewSTAR, Infinitt, Seoul, Korea). There were very low interobserver or intraobserver differences (interobserver correlation coefficients, 0.84; intraobserver correlation coefficients, 0.91).
3. Statistical analyses
The mean and standard deviation of all angles were calculated. Statistical differences between angles in different postures were calculated using one way analysis of variance. Correlations between SS/PT and LL were assessed using Pearson correlation analysis in SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). For all statistical comparisons, p-values <0.05 were considered significant.
Results
Thirty healthy male participants were enrolled in this study. The mean age of the participants was 31.1 years ([25-36]┬▒1.9 years), the mean weight was 73.6 kg ([58-89]┬▒9.2 kg), and the mean height was 175 cm ([160-188]┬▒6.1 cm). The calculated mean BMI was 23.1 kg/m2 ([17-29.1]┬▒2.4 kg/m2).
1. Lumbar lordosis
The mean angle of LL while standing was 47.1┬░┬▒10.5┬░. The LL in the five sitting positions was 36.2┬░┬▒8.4┬░ on a chair with lumbar support, 17.7┬░┬▒4.4┬░ on a 90┬░-angled chair, -4.9┬░┬▒3.3┬░ on a chair with anterior support, 0.6┬░┬▒3.6┬░ on a stool, and -7.4┬░┬▒3.5┬░ when sitting cross-legged. Changes in LL were quite variable according to the sitting position (Table 1). There was a significant decrease in LL while sitting when compared to standing (p<0.05). The reduction in LL was least observed on a chair with lumbar support, and an increased in LL was observed on the chair with anterior support, on the stool, and when sitting cross-legged. Indeed, lumbar kyphosis occurred in these latter positions.
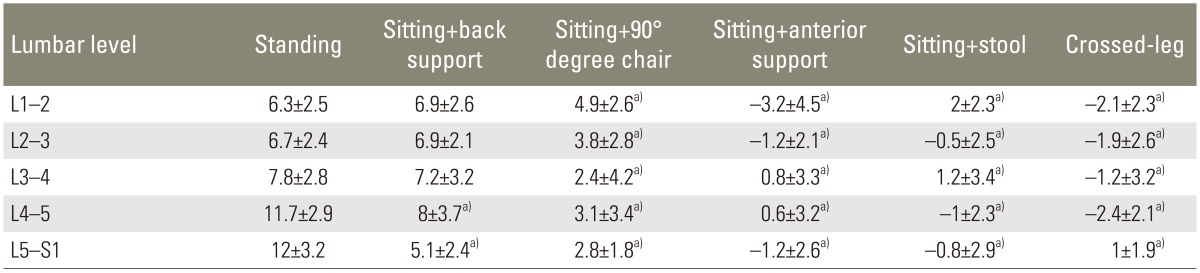
2. Lumbar segmental lordosis
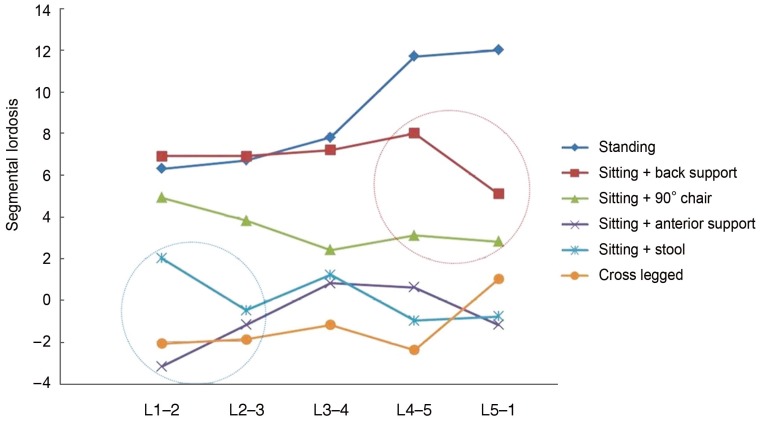
Compared with standing, apart from L1-2, L2-3, and L3-4 on a chair with lumbar support, all segmental angles decreased significantly (p<0.05) (Table 2). The lower lumbar segmental angles (L4-5 and L5-S1) significantly decreased in all sitting positions (p<0.05), but the decrease was relatively less on the chair with lumbar support and in the 90┬░-angled chair. Upper lumbar segmental angles (L1-2, L2-3) also showed a greater decrease on the chair with anterior support, on the stool, and when sitting cross-legged (Fig. 5).
3. Pelvic parameters
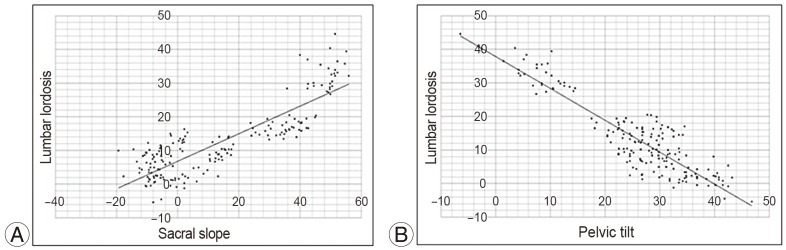
There was no significant difference in the PI according to posture. A strong correlation was observed between the decrease in LL and the decrease in the SS (r=0.731, p<0.01), as well as between the decrease in the LL and the increase in the PT (r=-0.842, p<0.01) (Fig. 6).
Discussion
Physiologic LL in standing position ranges from 40┬░ to 60┬░ [8181920]. Several complex factors affect the lumbar curvature, which has a role in balancing compressive forces. Various studies have examined the relationship between changes in the angle of the lumbar spine and back pain [212223]. Clinical observations suggest that aberrations of posture may play a role in the development of LBP [22]. Abnormal posture places strain on the ligaments and muscles, which indirectly affects the curvature of the lumbar spine.
When sitting, the knees and hips are flexed, the pelvis rotates backward, and LL flattens [21]. At the same time, there is an increased load on the spine, as indicated by measurements of intervertebral disc pressure. The intradiscal measurements reported by Andersson et al. [824] and Nachemson and Morris [25] indicate increased lower intradiscal pressure. Wilke et al. [26] used pressure transducers to show in vivo agreement with Nachemson's findings, i.e., intradiscal pressure was higher when leaning forward in a sitting position than when in relaxed sitting position.
The present study demonstrated that LL varies according to sitting position. A relatively low reduction in LL was observed when sitting on a chair with lumbar support or with a 90┬░ angle. Moreover, a larger reduction in LL was observed when sitting on a chair with anterior support, on a stool, and when sitting cross-legged; all of which resulted in lumbar kyphosis. Because we sit on a chair for long period of time, this severely decreases LL and may be related to increasing intradiscal pressure that resulted in LBP over time. Moreover, preserved LL during sitting position is more important in children while studying.
Lumbar segmental angles also changed according to changes in LL. When sitting on a chair with lumbar support or with a 90┬░ angle, there was a relatively low decrease in LL, which was mostly affected by a decrease in the lower segmental angles (L4-5 and L5-S1). Compared to sitting on a chair with back support or with a 90┬░ angle, lumbar kyphosis owing to a large decrease in LL resulted from sitting on a chair with anterior support, on a stool and when cross-legged. This was greatly influenced by the decrease in the upper segmental angles (L1-2 and L2-3) as well as a decrease in the lower segmental angles (L4-5 and L5-S1). Surprisingly, the changes in upper lumbar segmental angle had a greater influence in the observed decreased angle of LL. This is consistent with the finding of Miyasaka et al. [27]. They found that upper lumbar segment had a more significant role in lumbar motion during daily living.
We spend a lot of time sitting on the floor. Sitting on the floor cross-legged is the usual posture adopted during normal daily living, especially in Asia. Snijders et al. [28] reported that sitting cross-legged resulted in elongation of the piriformis muscle, which contributes to sacroiliac joint instability. Lee and Yoo [29] reported that it also caused back pain due to increased gluteal pressure and pelvic misalignment. This study also showed that a large reduction in LL might result in increased risk factor of LBP.
The present study demonstrated a strong correlation between the decrease in LL and the decrease in SS (r=0.731, p<0.01), as well as between the decrease in LL and the increase in PT (r=-0.842, p<0.01). The sitting position led to a decrease in LL and pelvic retroversion (increase in PT) and a vertical sacrum (decrease in the SS), similar to the findings of Lazennec et al. [30]. These authors demonstrated that patients with persistent postoperative back pain following lumbosacral fusion have a more vertical sacrum, with a decreased SS and increased PT, and do not have sufficient compensatory motion occurring normally at the spine and pelvis. Considering the correlations between different spinopelvic parameters, there may be an obvious adverse effect associated with sitting in patients after spine fusion, as well as in healthy individuals.
In our study, there were several limitations. We were limited to healthy male participants because of the risk of radiologic hazard to young women. By limiting the study to healthy male individuals, they may not represent the broad population with regards to LL and lumbar segmental angles. We also did not perform a comparative study between patient groups (chronic LBP or patients with lumbar spine fusion). Despite the fact that our study had some methodological limitation, it is one of the few cross sectional experimental studies showing some changes in LL and pelvic parameters according to various sitting position.
Because we only considered spinopelvic alignment according to sagittal radiographs, we overlooked the load distribution in the relaxed position with anterior support, which would be load distribution to upper extremity and perhaps lead to reduction of load transmission to spine and pelvis. Further studies should evaluate the effects of load distribution in the anterior support position. In addition, dynamic Magnetic resonance imaging evaluation of disc morphologic changes would be helpful for more precise measurement of the lumbar segments.
Conclusions
Sitting caused a reduction in the LL and SS when compared to standing in healthy volunteers. These changes in LL and spinopelvic parameters could cause a spinopelvic imbalance and may result in chronic LBP. In practice, it is better to select a sitting position that results in minimal change to LL. In our study, sitting on a chair with back support demonstrated the least amount of change to LL and the SS.