Introduction
Ankylosing spondylitis (AS) is a common inflammatory rheumatic disease affecting the axial skeleton and leading to progressive ankylosis of all spinal segments from the occiput to the iliac bone. Because of reduced biomechanical flexibility, the spinal column acts like a long-bone lever, causing severe instability in cases with vertebral fractures. Cervical and cervicothoracic fractures related to AS are common and potentially hazardous. These patients may experience implant failure, pseudarthrosis, and dislocation. In addition, the mortality rate among patients with such fractures is considerably high [1-5]. Recently, the use of antirheumatic treatment for AS has improved the course of the disease considerably. However, the frequency of cervical fractures related to AS is increasing progressively [6,7].
AS leads to total immobility of the spinal column and often fused thoracic hyperkyphosis [8], compromising the ability of the patients to sit, stand, or lie smoothly. Thoracic hyperkyphosis causes hyper-cervical lordosis because patients acquire a horizontal gaze [9,10]. Furthermore, patients with AS are unable to see the horizon, causing severe problems in daily activities. The fusion of the occipitocervical junctions is usually delayed in patients with AS. Although commonly observed, the progression of ankylosis in the upper cervical spine is not well documented.
In this study we present the radiographic features of the occipitoatlantoaxial (OAA) joint in patients with AS using a novel measure termed X-angle [11] and describe the correlation between the ankylosed OAA joint and thoracic kyphosis (TK).
Materials and Methods
1. Study design
This was a retrospective cohort study of prospectively collected data from patients with AS assessed for spinal fracture. The study was performed in the Uppsala University Hospital and approved by the Uppsala regional ethical review board (IRB approval no., 2010/131, no. 2010/297/1) and complies with the criteria of the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) and RECORD (Reporting of Studies Conducted Using Observational Routinely-Collected Health Data) statements for observational studies [12].
2. Setting
The study was performed in a single level-1 trauma-center at the Uppsala University Hospital, Uppsala, Sweden between 2007 and 2014. All patients with a history of AS and minor trauma/inflammatory back pain underwent investigation of the axial skeleton using computed tomography (CT) to exclude AS-related fractures or discovertebral (Andersson) lesions. Patients with spinal fractures treated surgically were registered in the Swedish Spine Registry (SWESPINE) [13]. Surgical treatment included long posterior fixation using a screw-rod construct extending three levels cranially to three levels caudally of the injury. In case of spinal cord injury, additional decompression and evacuation of epidural hematoma were performed (Fig. 1).
3. Patients
Patients meeting all the following criteria were included in the study: (1) AS with thoracic ankylosis; (2) acute cervical fracture; and (3) age Ōēź45 years. Patients meeting any of the following criteria were excluded from the study: (1) incomplete radiographic examination (i.e., no inclusion of the craniocervical junction); (2) incomplete electronic record file of the patient; (3) age <45 years; (4) acute thoracic fractures; (5) acute lumbar fractures; and (6) living in a nursing home for patients with dementia.
4. Variables
1) Classification of ankylosing spondylitis fractures
Fractures were classified into four groups using the classification of AS introduced by Caron et al. [14], based on fracture excursion through the intervertebral disc injury (i.e., type I, transdisc disruption; type II, vertebral body injury; and types III and IV, combination of disc and vertebral body injuries) (Fig. 1).
2) Thoracic sagittal alignment
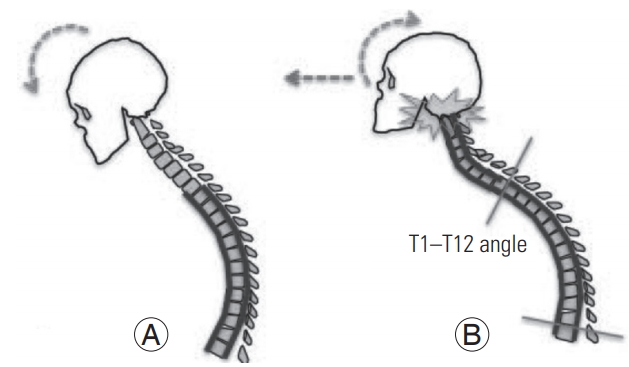
TK was measured preoperatively using the global Cobb angles T1ŌĆōT12 and T5ŌĆōT12 on lateral radiography. A line was drawn along the plane of the superior endplate of T1 or T5 and the inferior endplate of T12.
3) Osteoarthritis occipitoatlantoaxial joint changes: descriptive radiology and X-angle
A sagittal view of the OAA joint was obtained prior to surgery using CT. The narrowing and/or sclerosis on the C0ŌĆōC1 joint space, observed through CT, were defined as osteoarthritic changes. The disappearance and/or fusion of the C0ŌĆōC1 joint space were defined as ankylosed joint.
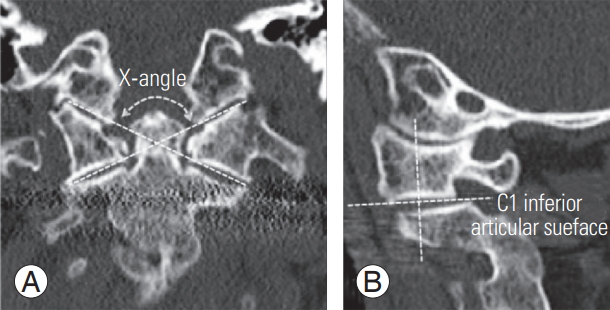
The progressive degeneration of the C0-C1-C2 joints was evaluated using a new indicator termed X-angle. The X-angle is formed by lines drawn from the occipitoatlantal to the atlantoaxial joints on the contralateral side of coronal CT reconstructions, using the coronal plane perpendicular to the center of the C1 inferior articular surface (Fig. 2).
5. Data sources and measurement
All CT scans were analyzed using the multiplanar reconstruction function of the electronic radiographic information system (Carestream PACS, Solna, Sweden). Change in the osteoarthritic OAA joint and the level of cervical fracture were assessed by three experienced investigators (NM, AC, and YR).
6. Bias
The inter- and intra-observer reliability of the X-angle was assessed. The X-angle was measured independently by two investigators, and the intraclass correlation coefficient (ICC) and interclass correlation coefficient were determined.
7. Statistical methods
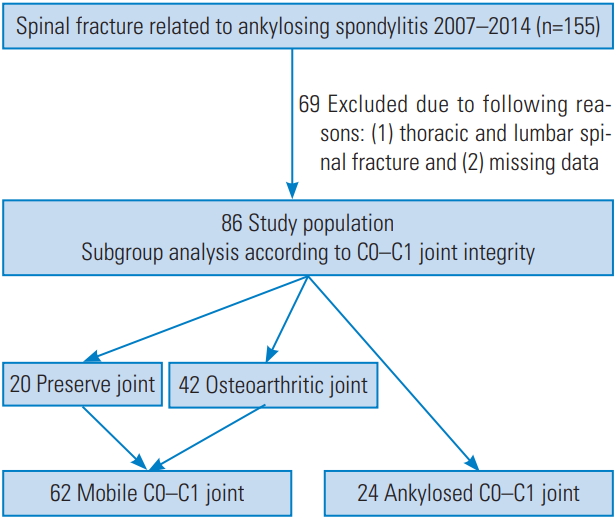
Subgroup analysis was performed according to the integrity of the C0ŌĆōC1 joint. The mobile joint group was characterized by a preserved joint with osteoarthritic changes, while the ankylosed joint group exhibited fused articulations.
The non-paired sample t-test and FisherŌĆÖs exact test were used to identify differences between groups. The ICC two-way mixed model on absolute agreement was used to analyze the reliability of X-angle measurements [15]. This is a ratio of the variance between patients to the total variance (patients, raters, and error). The values of the ICC range from 0 to 1, with a higher value indicating better reliability. The ICC were interpreted as poor (<0.40); fair (0.40 to 0.59); good (0.60 to 0.74), and excellent (0.75 to 1.00) [16].
All analyses were performed using The IBM SPSS ver. 22.0.0 for Mac (IBM Corp., Armonk, NY, USA). The mean values are presented with standard deviation, followed by intervals in brackets. All reported p-values were two-tailed, with p<0.05 denoting statistically significant differences.
Results
1. Patients
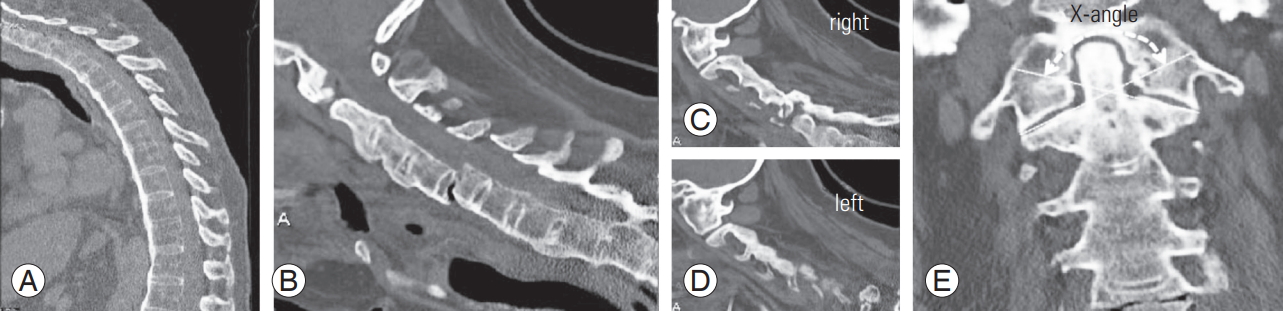
Patients with AS (n=155) underwent spinal fixation for the treatment of spinal fracture between 2007 and 2014. Of those, 69 patients were excluded from the analysis. The inclusion flow chart is presented in Fig. 1. We included 67 male and 19 female patients, aged 69.2┬▒11.8 years (range, 49ŌĆō94 years), with AS and ankylosis of the thoracic spine. Representative cases are shown in Figs. 3ŌĆō5.
2. Descriptive data
A total of 78 patients underwent posterior fixation surgery, while eight patients underwent combined anterior and posterior fixation surgery. Posterior screws were inserted unless they were localized in three vertebrae cranially and three vertebrae caudally from the injury. Of the 86 patients with AS, three patients in the fused joint group were treated with posterior stabilization from the occipital bone to the upper thoracic spine using a screw-rod system (Table 1).
3. Main results
The 86 patients with AS were divided into subgroups according to the integrity of their C0ŌĆōC1 joint: the mobile joint group included 20 patients with a preserved joint and 42 patients with osteoarthritic changes, while the ankylosed joint group included 24 patients with fused articulations (Fig. 1). There was no significant difference observed between the two groups in terms of age and the level of fracture. A C6 vertebral fracture was the most common fracture in the present study. There was a statistically significant difference observed in the T1ŌĆōT12 and T5ŌĆōT12 angles. TK was greater in the fused group than in the mobile joint group. The most significant difference between the two groups was recorded using the X-angle. The X-angle was greater in the ankylosed joint group because of the vertical destruction of the OAA joint (Table 2).
4. Other analyses: intra- and inter-observer reliability of the X-angle measurements
The ICC and interclass correlation coefficient r values for the relationship between the two investigators were 0.945 (p<0.001) and 0.926 (p<0.001), respectively (Table 3).
Discussion
1. Key results
This was the first radiographical cohort study employing the X-angle method in patients with an ankylosed spine related to AS. The X-angle had high inter-observer reliability and could be related to thoracic sagittal alignment.
2. Limitations
Patients with AS underwent radiological imaging testing in the supine position, because of the severe injuries in their spinal bone. Therefore, it was not possible to measure the fractured spine and non-fused mobile segments. We hope to be able to study the alignment of noninjured patients in future studies.
There were no significant differences observed between the age of patients in the mobile and ankylosed groups (p=0.094). However, patients in the mobile group were slightly older than those in the ankylosed joint group. Due to the small sample size of this study, these results may vary.
Previous anatomical studies have described racial differences observed in the atlas and other craniocervical bones. It is therefore important to take such potential differences into consideration [17].
3. Interpretation
The definition of morphological change depended extensively on the investigator and selected measuring technique. Morphological changes were easily definable in patients with AS and a completely ankylosed C0-C1-C2 joint. However, in patients with AS and fusion of only one side of the joint, defining the morphological change was challenging (Fig. 5). The X-angle was a very useful tool in quantifying morphological change in such cases. The X-angle was increased in cases with a collapsed and fused C0-C1-C2 joint. Koller et al. [18] reported the importance of the axial, sagittal, and coronal CT-reconstruction in revealing deformations and rotation of the OAA joint.
The fractures are often caused by low-energy impacts and are highly unstable due to the long lever arms produced by stiffness of the largely ankylosed spinal column. Therefore, most fractures require long-segment posterior fixation [2]. In this study, patients with AS and fracture of the cervical spinal were treated with long posterior stabilization from the upper cervical to the upper thoracic spine using a screw-rod system [19]. In patients with a fused C0-C1-C2 joint or large X-angle, extension of the instrumentation to the cranial bone was comparable in a strong construct.
Scheer et al. [9] reported that increased TK is correlated with increased cervical lordosis, and the Pearson coefficient (r) value between the cervical and thoracic alignment was ŌłÆ0.51. Lee et al. [10] reported sequential correlations between adjacent segments and demonstrated the correlation between the C2ŌĆōC7 and C0ŌĆōC2 angles (the r value was ŌłÆ0.547). In patients with AS and thoracic hyperkyphosis, the head was bending down. However, the occipitocervical joint was held in hyperlordosis to obtain a horizontal gaze. The compensatory hyperextension may lead to accelerated degeneration of the OAA joints. Furthermore, the OAA joint was collapsed and fused in patients with AS (Fig. 6). Finally, there were correlations detected between TK and the X-angle (r=0.338, p=0.02).
The ICC and interclass reliabilities for the X-angle measurements were very high (0.95 and 0.93, respectively) suggesting a strong correlation and high accuracy of this measurement technique (Table 3).
4. Generalizability
We used the new indicator X-angle in patients with AS and craniocervical arthritic or fused joints. Therefore, the X-angle will be useful for the detection of occipitocervical diseases, such as rheumatoid arthritis [20], because this X-angle increased in step with the vertical destruction of the C0-C1-C2 joints. Furthermore, patients with high X-angle values are often characterized by an abnormal craniocervical junction [21]. Therefore, it would be necessary to consider an availability of high riding vertebral artery in such patients.
Conclusions
A fused C0ŌĆōC1 joint in patients with AS was related to thoracic hyperkyphosis. The X-angle is a reliable tool for the quantification of morphological change in the C0-C1-C2 joint. These findings will improve our understanding of challenges in patients with AS related to cervical fractures, occipitocervical degenerative change, and strategy of surgical treatment.