Navigated Pin-Point Approach to Osteoid Osteoma Adjacent to the Facet Joint of Spine
Article information
Abstract
Osteoid osteoma (OO) is a benign osteoblastic tumor. Its curative treatment is complete removal of the nidus, where intraoperative localization of the nidus governs clinical results. However, treatment can be difficult since the lesion is often invisible over the bony surface. Accordingly, establishment of an ideal less invasive surgical strategy for spinal OO remains yet unsettled. We illustrate the efficacy of a computed tomography (CT)-based navigation system in excising OO located adjacent to the facet joint of spine. In our 2 cases, complete and pin-point removal of the nidus located close to the facet joint was successfully achieved, without excessive removal of the bone potentially leading to spinal instability and possible damage of nearby neurovascular structures. We advocate a less invasive approach to spinal OO, particularly in an environment with an available CT-based navigation system.
Introduction
Osteoid osteoma (OO) is a benign bone tumor originally described by Jaffe [1] in 1935. OO predominantly localizes in the long bones of extremities, while its occurrence in the spine remains as low as 10% to 20% [2]. Its curative treatment is complete removal of the nidus. Intraoperative localization of the nidus governs clinical results [34]. However, treatment can be difficult since the lesion is often invisible over the bony surface [35]. Furthermore, we must remember that spinal fusion becomes necessary when spinal stability is compromised by a wide resection of the affected vertebrae.
In recent years, a computer-assisted navigation system has become increasingly popular among spinal surgeons. Many reports emphasize that it increases the accuracy of implantation [6] and bone resection in cases with ossification of the spinal ligaments [78] and bone tumors [59101112] by providing real-time information.
In the present report, we describe 2 cases with OO adjacent to the facet joint of spine. Both cases were successfully treated with a pin-point excision of the nidus without compromising spinal stability or damaging neurovascular structures using a computed tomography (CT)-based navigation system.
Technical Note
From 2008 to 2011, 2 cases of OO adjacent to the facet joint of spine were treated with CT-based navigation surgery in our institutes. Written informed consent was obtained from the patient for publication of this report and any accompanying images.
1. Navigation-assisted surgery
The navigation systems used were StealthStation TRIA (Medtronic Sofamor Danek, Memphis, TN, USA) for case 1 and VectorVision (Spine ver. 5.6, Brain Lab, Feldkirchen, Germany) for case 2. Both systems are commerciallyavailable CT-based navigation systems. The basic data used for navigation consist of preoperative CT data (slice thickness, 1 mm), which are transferred and recorded on the system computer and reconstructed into three-dimensional (3D) images.
The registration procedures of point merging and surface merging produces 3D spinal images on the monitor that are identical to the actual appearance of the spine in the operative field. The accuracy of the images is verified by placing a tool navigator on various parts of the exposed area.
2. Case 1
A 40-year-old man suffered from localized left lower back pain with a 3-year history. The pain deteriorated gradually, particularly during night time. His sleep was constantly disturbed by unremitting pain during the previous year. He visited an orthopaedic clinic where OO of L2 was identified by CT (Fig. 1A) and magnetic resonance (MR) imaging. Nidus was localized in the subchondral region of the left superior articular process of L2 (Fig. 1A). Treatment with non-steroidal anti-inflammatory drug (NSAID) was effective, however, this treatment was halted due to a drug-induced gastric ulcer.

Case 1. Computed tomography images. Preoperative (A), Postoperative (B) and one-year follow-up (C) computed tomography images. Pin-point extirpation of the nidus without excessive bone resection (B) and its remodeling (C) was observed. No tumor recurrence was detected.
Subsequently, he was introduced to us for surgical treatment. Physical examination revealed only a localized tenderness over the left L1/2 facet joint without neurological compromise. After paramedial skin incision, the left L1/2 facet was exposed by splitting multifundus and longissimus muscles. Reference frame was placed to the tip of the L2 spinous process following minimum exposure. Registration was performed by tracing the spinous process, left transverse process, left lamina and left superior articular process of L2. Macroscopically, we could not localize the nidus over the bony surface. Following navigation guidance, a precise localization of the nidus became possible. En-block extirpation was performed from the extra-articular aspect of the superior articular process of L2 without exposing its articular surface. The pin-point approach to the nidus enabled maximum preservation of capsular attachment to the facet joint. Histological examination revealed that the resected specimen was compatible with OO.
Postoperative CT taken immediately after the operation revealed complete and pin-point removal of the nidus (Fig. 1B). At the time of the latest follow-up, 2.5 years after surgery, the patient was free of symptoms, and there was no clinical or radiologic evidence for instability and recurrence of the tumor (Fig. 2). Bone defect of left superior articular process of L2 was completely remodeled postoperatively (Fig. 1C).
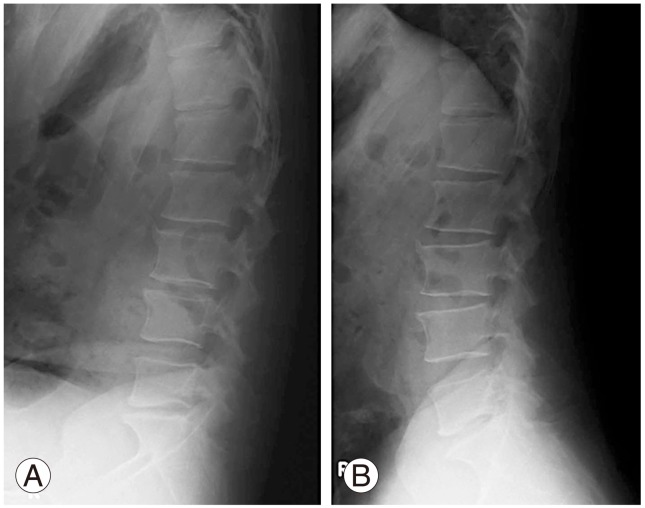
Case 1. Postoperative plain X-ray of lumbar spine in flexion (A) and extension (B) positions at the latest follow-up, 2.5 years after surgery, showed no radiographic instability.
3. Case 2
A 16-year-old man complained of right neck pain. A plain X-ray of the cervical spine at the initial consultation showed a slight torticollis. MR imaging revealed an inflammation/edema pattern at the right side of C2 lamina (Fig. 3) with the diagnosis of bone bruise. He enjoyed playing Judo, though he reported no preceding severe trauma. NSAID was effective during an early stage of his illness, though pain aggravated gradually.
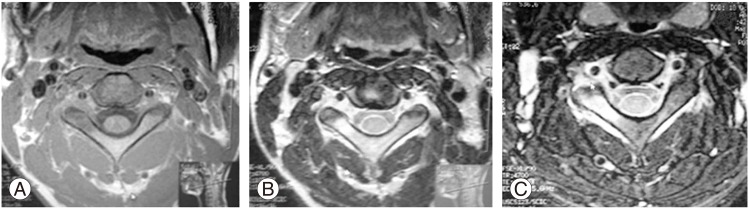
Case 2. Preoperative magnetic resonance imaging of T1-weighted (A), T2-weighted (B) and short TI inversion recovery (C) images showing inflammatory/edema pattern intensity at the right side of the C2 lamina.
Six months after the onset of symptoms, he was referred to us for persistent neck pain. On physical examination, right rotation of the neck was noticeably limited with no neurological compromise. Second-look MR imaging demonstrated a persistent abnormality. Subsequent CT demonstrated a small round nidus at the base of right inferior articular process of C2 (Fig. 4A, B). Technetium bone scan showed a focal uptake at an area corresponding to the lesion detected by CT and MRI.

Case 2. Preoperative coronal (A), sagittal (B), and reconstruction computed tomography (CT) images showing a nidus of C2 (red arrowheads). Postoperative coronal (C) and sagittal (D) reconstruction CT images revealed complete and pin-point removal of the nidus without excessive bone resection around the lesion.
Under a tentative diagnosis of OO arising at C2, removal of the nidus was performed using a CT-based navigation system. To minimize possible navigational error caused by a change in intersegmental relationship after surgical positioning, we carefully positioned the patient to reproduce the alignment of C2–3 in preoperative CT. Right laminae of C2 and C3 were minimally exposed up to the lateral edge of facet joint. Extensor muscles attached to C2 and C3 were maximally preserved. The reference frame of the navigation system was set on the Kirchner wires inserted into the spinous process of C2 and C3. Registration was performed by tracing the inferior articular process of C2, the spinous process and the right laminae of C2 and C3.
Via navigation guidance, a trans-laminar tunnel reaching to the nidus was made using a high-speed drill. Then, complete removal of the nidus was achieved without sacrificing spinal stability (Fig. 5). The CT-based navigation system not only enabled pin-point removal of the nidus but also prevented possible damage of nearby critical structures (Fig. 5). Histopathological diagnosis of the resected lesion was that of OO (Fig. 6). Postoperative CT confirmed the complete removal of the nidus (Fig. 4C, D). At the time of the latest follow-up, 3.5 years after surgery, the patient was free of symptoms and there was no clinical or radiologic evidence for recurrence of the tumor (Fig. 7).
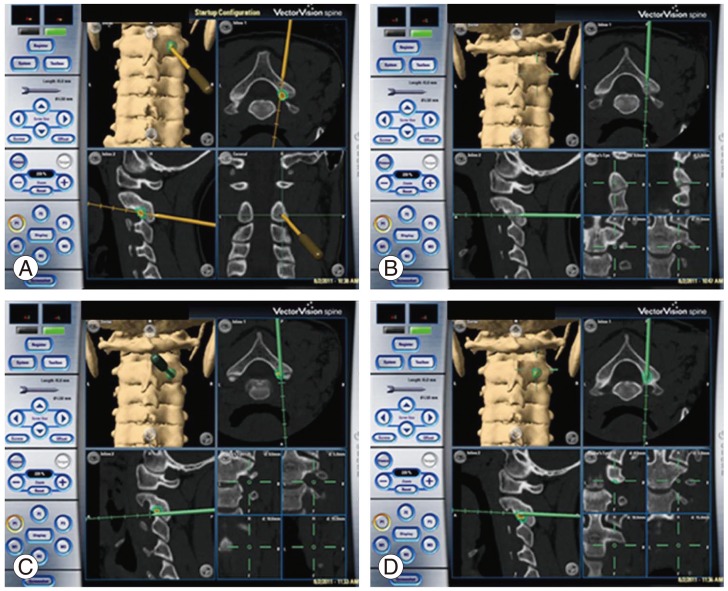
Case 2. Intraoperative navigation monitoring. On the screen, three-dimensional, coronal, sagittal, and axial images in conjunction with the actual instrument tip image. Yellow (A) and Green (B–D) arrows indicate the position of the pointer in the operation field.
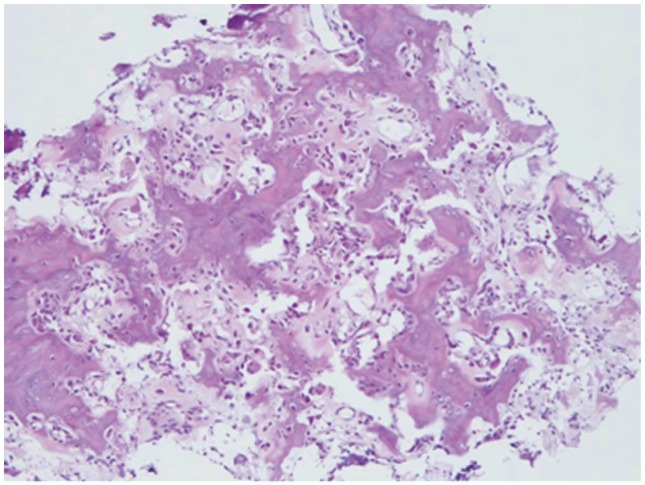
Case 2. Histolopathological examination revealed that the extracted lesion showed an osteoid lined with plump osteoblasts and vascularized connective tissue (H&E, ×100).

Case 2. Postoperative plain X-ray of the cervical spine in flexion (A) and extension (B) positions at the latest follow-up, 3.5 years after surgery, showed no radiographic instability.
Discussion
Several therapeutic modalities to treat OO have been proposed to minimize surgical trauma. Such modalities include radiofrequency thermal coagulation [213] or drill resection [14] under CT guidance. These techniques have been verified in the treatment of bone tumors of extremities. Spinal OO, however, may not allow a straightforward application of these techniques. Namely, application of these techniques in spinal OO carries a latent risk of damaging adjacent structures, such as the spinal cord, nerve root and vertebral artery [213141516]. Indeed, several authors have reported undesirable consequences resulting from damaging the neurovascular structures while performing these techniques on spinal tumors [31417].
Another critical drawback of thermal deactivation of the nidus with electrical coagulation resides in a lack of histological verification of the tumor [25]. Histological examination is recommended in order to confirm the diagnosis of the tumor [15]. Indeed, Sans et al. [15] reported that inconsistent histological diagnosis was made in 6 out of 38 patients with OO treated by CT-guided percutaneous drill resection.
In turn, the recent development of CT-based navigation surgery considerably contributed to spinal surgery. Van Royen et al. [11] reported 5 cases of spinal OO successfully treated with a CT-based navigation system combined with high-speed drill excision. They emphasized that the simultaneous use of γ probe guidance with the CT-based navigation system greatly facilitated matching the spinal anatomy of the patient. However, this technique imposes radiologic exposure on the patient.
Rajasekaran et al. [5] reported use of the Iso-C 3D navigation system for the treatment of spinal OO in 4 cases. The authors emphasized advantages of this system over the CT-based navigation system: anatomical registration is unnecessary, multiple adjacent levels are registered simultaneously, and images for navigation are taken after intraoperative acquisition of optimal alignment. In addition, intraoperative excision is confirmed through reacquisition of data. However, the Iso-C 3D navigation may not provide as fine an image as the CT-based navigation system, particularly when localizing small lesions as in spinal OO [18].
Nagashima et al. [12] recently described a case with an OO of the C2 pedicle successfully treated by using a conventional CT-based navigation system. They used the CT-based navigation system simply to localize the bony lesion after an extensive exposure of the entire posterior compartment of the affected vertebra.
The CT-based navigation system does not only prevent damaging of adjacent neurovascular structures, but also allows pin-point, a minimally invasive approach reaching directly to the target lesion. Since excessive resection of bone and joint structures as well as detachment of spinal muscles greatly compromises spinal stability, we advocate a less invasive approach to spinal OO, particularly in an environment where a CT-based navigation system is available. However, we must keep in mind that computerassisted surgeries still carry latent errors. Iso-C 3D navigation and CT-based navigation have a mean deviation of 0.5 mm and 1.0 mm, respectively [19].
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.