Effects of Methylprednisolone on Neuroprotective Effects of Delay Hypothermia on Spinal Cord Injury in Rat
Article information
Abstract
Study Design
A retrospective study.
Purpose
The aim of this study was to evaluate the effects of delayed hypothermia on spinal cord injuries in rats. In addition, the effect of methylprednisolone on therapeutic window of hypothermia was evaluated.
Overview of Literature
Several studies have demonstrated that early hypothermia is the most effective neuroprotective modality. However, delayed hypothermia seems to be more practical for patients with traumatic spinal cord injuries. A combination of hypothermia and other neuroprotective methods, such as using methylprednisolone, may help extend the therapeutic window of hypothermia.
Methods
One hundred and twenty male rats were categorized into six groups. The rats in five groups were subjected to spinal cord injury using the weight drop method, followed by treatment, consisting of early hypothermia, late hypothermia, late hypothermia plus methylprednisolone, or methylprednisolone only. Biochemical tests including catalase, malondialdehyde, and superoxide level were evaluated in the injured spinal cord. Behavioral functions of the hind limb were evaluated by Basso-Battle-Bresnaham locomotor rating scale and tail-flick tests.
Results
Functional and biochemical evaluation showed both early and late hypothermia had significant neuroprotective effects. The treated groups did not differ significantly from one another in the behavioral tests. Hypothermia had better biochemical results compared to methylprednisolone. Also, methylprednisolone was shown to extend the therapeutic window of delayed hypothermia.
Conclusions
Hypothermia showed a significant neuroprotective effect, which can be improved with further studies optimizing the duration of hypothermia and the rewarming period. Moreover, the therapeutic effect of the delayed hypothermia can be extended by methylprednisolone.
Introduction
Today, hypothermia is known as one of the strongest neuroprotective modalities. It is commonly used during abdominal aortic aneurysm repair to protect the spinal cord from intraoperative ischemia [1]. However, it has not been used clinically to treat traumatic spinal cord injuries. Patients with traumatic spinal cord injury often arrive at the hospital too late to be candidated for early hypothermia, so an effective delay hypothermia would be more practical. The neuroprotective effect of late onset hypothemia on traumatic spinal cord injuries has not been well determined yet and needs to be studied. Some studies have demonstrated that late onset hypothermia has a neuroprotective effect on ischemic and traumatic brain insults, but this effect was found to be less than that of early onset hypothermia [2,3]. The other question that arises is whether the simultaneous use of a neuroprotective agent such as high dose methylprednisolone with late onset hypothermia can enhance or extend the therapeutic window of hypothermia. This study was designed and undertaken to determine whether a neuroprotective agent could extend delayed hypothermia's effective therapeutic window.
Materials and Methods
1. Spinal cord injury
Adult male Wistar rats weighing 250-300 g were used for the study. All the rats were anesthetized with Xylazine (10 mg/kg) and Ketamine hydrochloride (60 mg/kg) [4]. Through a dorsal incision, T8-9 laminectomies were performed in the prone position. spinal cord injury (SCI) was induced with the weight drop method. In this method, a stainless steel rod (10 g, 3-mm diameter tip) is dropped through a 2.5 cm guide tube positioned perpendicularly to the center of the spinal cord [5]. After the surgical and traumatic interventions, the wounds were closed in layers with silk sutures. The Animal Ethics Committee of Neuroscience Research Institute approved the protocols used in this study.
1) Hypothermia
Hypothermia was induced with a hypothermia machine to keep the rectal temperature at 33.5±0.5 degrees [6]. Hypothermia was done via two protocols: early hypothermia, in which hypothermia began 30 minutes after spinal cord injury, lasted for 180 minutes, and was followed by a 30 minute rewarming period to slowly bring the temperature back to 37 degrees; late hypothermia, which started 210 minutes after spinal cord injury, lasted for 180 minutes, followed by a rewarming period to slowly bring the temperature back to 37 degrees [7]. The animals were kept under anesthesia during hypothermia in both methods.
2) Experimental groups
One hundred and twenty rats were randomly and blindly allocated into six groups of twenty rats each: (1) Early hypothermia group: thirty minutes after spinal cord trauma, systemic hypothermia was induced through the early hypothermia protocol. (2) Delayed hypothermia group: three hours after spinal cord trauma, systemic hypothermia was induced through the late hypothermia protocol. (3) Delayed hypothermia+methylprednisolone group: immediately after spinal cord injury, methylprednisolone 30 mg/kg [8,9] was administered intravenously and followed by delayed hypothermia. (4) Methylprednisolone group: animals received a single high dose of methylprednisolone sodium succinate (30 mg/kg) intravenously immediately after trauma. (5) Trauma group: animals underwent laminectomy and spinal cord injury. (6) Control group: control animals underwent all surgical procedures except the spinal cord injury.
The animals were allowed access to water and food freely and were kept at the Animal Care Facility at Kerman Medical University Neuroscience Research Center.
2. Biochemical analysis
Ten rats from each group were sacrificed 24 hours after spinal cord injury using a lethal dose of ketamine hydrochloride. The operated area was opened, and a 1.5-2 cm long sample of spinal cord, including the traumatized segment, was obtained. The samples were rinsed with physiologic saline and frozen just after sampling and kept at -70℃; malonyldialdehyde (MDA) levels, as an index of lipid peroxidation, were determined by a thiobarbituric acid as detailed by Mihara and Uchiyama [10].
Super oxide dismutase (SOD) level measurements were determined on the basis of SOD's inhibition of the colorimetric reaction due to the superoxide radical [11].
Catalase activity was measured using a colorimetric assay based on the catalase's dismutation of hydrogen peroxide; absorbance was read in a spectrophotometer at 240 nm according to the method described by Aebi [12].
Protein concentrations were determined according to Lowry's method [11].
3. Locomotor function
Behavioral tests were performed using the Basso-Beattie-Bresnahan (BBB) scale by an investigator blinded to the treatment groups [4]. Testing began 1 day after the 12.5 mm spinal cord injury and then continued for six weeks.
4. Nociceptive function
Nociceptive function of the spinal cord was evaluated by performing a standardized tail flick test [13]. Each measurement was repeated three times, with at least four minutes between each test.
5. Statistical analysis
All the data collected from the experiment were coded, recorded, and analyzed using SPSS ver. 10.0.1 (SPSS Inc., Chicago, IL, USA) software for Windows. Statistical comparisons between the groups were tested with the Kruskal-Wallis test, and the Mann-Whitney U test was used for dual comparisons. In each test, the data were expressed as mean±standard deviation, and p<0.05 was accepted as statistically significant.
Results
The MDA level, as an index of lipid peroxidation, was significantly higher (p=0.006) in the trauma group (92.5±22 µM) compared to the other groups. As shown in Table 1, hypothermia significantly inhibits MDA. Early hypothermia kept MDA at a lower level than late hypothermia, a difference which was statically significant (p=0.004). The differences between MDA level in the early hypothermia group and the late hypothermia and methylprednisolone group (LH+MP) was significant (p=0.001); LH+MP controlled MDA better than just early hypothermia alone. The CAT level was lowest in the trauma group (5.54±3.55) and the highest in the LH+HP group (8.95±5.64). Other biochemical findings are shown in Table 1.

Biochemical results in each study group
The animals that received treatment exhibited significantly (p=0.05) higher BBB locomotor function scores compared with the trauma group 2-3 week after SCI. Importantly, while the animals in the trauma group began to plateau in their locomotor abilities three weeks after injury, the treated animals continued to improve their locomotor abilities for six weeks after injury. There was no significant difference (p=0.1) between the locomotor capabilities of the treated groups. None of the groups achieved full recovery (Fig. 1).
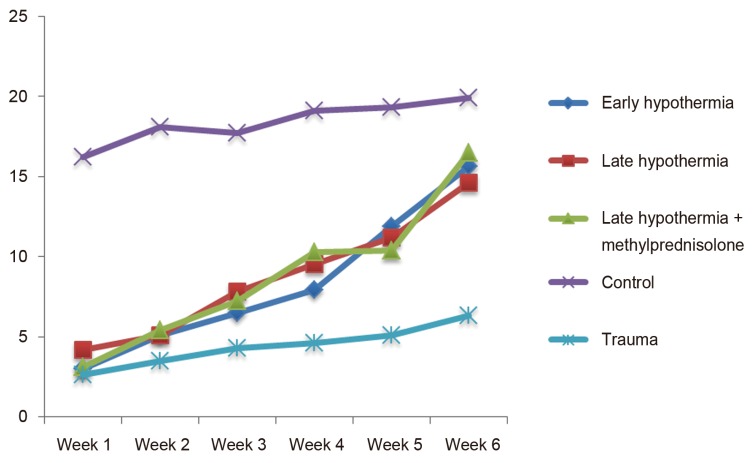
Basso-Beattie-Bresnahan locomotor function scores results in each study group.
The treated groups all had shorter tail flick latency compared to the trauma group. In the treated groups, the best result was seen in the animals treated with late hypothermia plus methylprednisolone, a difference that was marginally significant (p=0.054).
Discussion
Many studies have shown the beneficial effect of neuroprotective hypothermia [8,9]. In line with these studies, our present study also revealed that early onset hypothermia had a neuroprotective effect, which was not only pronounced in biochemical tests (p<0.01), but also significant in the tail-flick test (p=0.008). Hypothermia works through several mechanisms, one of which is controlling the injury-induced immune response [14]. In this mechanism, hypothermia reduces vasogenic edema and controls chemotaxis of polymorphonuclear leukocytes (PMN) cells [14]. The level of PMN cell activity can be measured using the MPO level, which reaches its maximum 3-24 hours after SCI [6]. Hypothermia also delays the glutathione release and reduces the production of O2 free radicals [15]. Meanwhile, it increases the central nervous system's tolerance to ischemia and reduces the anaerobic metabolites [16].
Currently, the only neuroprotective action which is clinically widespread is methylprednisolone prescription [17]. However, in most of the studies, the hypothermia neuroprotective effect was stronger than that of a high dose of methylprednisolone [4,18]. In our study, early onset hypothermia had a better neuroprotective effect than methylprednisolone alone. Theearly onset hypothermia group performed slightly better than the methylprednisolone group, but the difference was not significant. However, the tail-flick test in the early onset hypothermia group was marginally (p=0.054) better, and MDA level was significantly (p=0.035) better than that of the methylprednisolone group. This finding has been also reported by other studies, and it seems hypothermia can play a major role in spinal cord injury treatment going forward.
Some studies on ischemic and traumatic brain injuries have shown that the sooner the hypothermia starts, the better the effect will be [19,20]. The only study on the effect of delayed onset hypothermia on SCI found that early onset hypothermia has a better result as compared with hypothermia starting three hours after the injury [21]. In the present study, early onset hypothermia clearly had a stronger neuroprotective effect than delayed hypothermia in the biochemical tests (p=0.004). However, there was not a significant difference between the early and the delayed onset hypothermia groups in the functional tests (p=0.384). The lack of a significant difference in the functional tests between the two groups might have several reasons. Using a non-optimal method of hypothermia is probably the most important reason. Duration and depth of hypothermia and speed of rewarming are factors that influence the results of this method. It has been reported that longer hypothermia has a better effect [22], but the optimal period has not yet been determined. In addition, the length of the rewarming period is important, and using short term rewarming may lead to the return of some of the damaging processes [23]. Nanda et al. [24] have suggested that the rewarming speed of 0.25 degrees centigrade per hour is suitable; in our study, we used a rewarming speed of about 6 degrees centigrade per hour. In the current study, we found that applied hypothermia was more effective on the biochemical tests, possibly because they were checked relatively soon after rewarming. If the duration of hypothermia or rewarming period was not ideal, it is possible the secondary damaging processes started again, which in turn negatively affected the functional tests because they were checked a relatively longer time after rewarming.
Trauma intensity is another factor that may influence the effects of any neuroprotective treatment [25]. The differences between early and late onset hypothermia methods may be more apparent in different severities of spinal cord injury. The lack of a significant difference between early and late onset hypothermia in functional tests can also be explained differently; it is possible that early onset mechanisms, like calcium hemostasis which starts minutes after injury [26], have less powerful effects on functional disability after spinal cord trauma. Additionally, mechanisms like inflammation [6] and glutathione release or the production of free radicals, which start about three hours after trauma [15], may have more important roles in functional outcome.
Nevertheless, delayed onset hypothermia is more practical in traumatic patients. The transferring and primary stabilization of the patients takes time and makes it difficult to induce hypothermia in the early hospital hours. Combining hypothermia with other neuroprotective actions may intensify the hypothermia neuroprotective effect while also can increasing its therapeutic window. We could only find one other study on the simultaneous use of methylprednisolone and late onset hypothermia [21]. The study found that methylprednisolone did not increase the therapeutic window of moderate systematic hypothermia in mild SCI in rats. On the contrary, in our study, the delayed onset hypothermia with MP had better results in biochemical tests than those of the early onset hypothermia group. This difference was statistically significant (p=0.001). In the study undertaken by Karamouzian et al. [21], the researchers only counted the number of white cells in the injury site to determine the effect of hypothermia, but in our study, we used the myeloperoxidase method, a standard method to examine inflammation [18].
It seems that there is high potential in hypothermia's neuroprotective action and the clinical benefits of delayed hypothermia require researchers to carry out more comprehensive studies to optimize this hypothermia method of treatment.
Our study was limited in that the optimal parameters for hypothermia have not been established, so the results from the present study should be interpreted with caution. However, the result of this study should serve as preliminary results to motivate further research.
Conclusions
Hypothermia as a neuroprotective modality is more effective compared to MP, and the simultaneous use of hypothermia and MP can increase the effective therapeutic window of hypothermia. However, optimizing the hypothermia method through further study would likely result in a better neuroprotective effect.
Acknowledgments
We are grateful to Ehsan Mehrabi Kermani (MA TEFL Shahid Bahonar University, Kerman, Iran) for editing the English text.
Notes
The study was supported by Neuroscience Research Center, Institute of Neuropharmacology, Kerman University of Medical Sciences, Kerman, Iran.
No potential conflict of interest relevant to this article was reported.