Hypertrophic Posterior Arch of Atlas Causing Cervical Myelopathy
Article information
Abstract
Cervical stenosis, especially of the upper cervical spine, is quite rare which can be developmental or acquired. Clefts or aplasias of anterior and posterior arches of atlas, ossification of the transverse atlantal ligament, hypertrophy of the dens and os odontoideum are rare conditions causing cervical myelopathy reported either singly or in combination. Hypertrophy of the posterior arch of atlas in the absence of any ring hypoplasia as a cause of cervical myelopathy has not been reported earlier. The authors report a case of cervical myelopathy in a 26-year-old female due to hypertrophied posterior arch of atlas which was preoperatively diagnosed as a bony tumor. Being aware of such an entity may avoid diagnostic surprises and facilitate patient prognostication and management.
Introduction
Congenital cervical stenosis as a cause of cervical myelopathy is a well recognized entity described mainly in the subaxial cervical spine. Cervical stenosis, especially of the upper cervical spine, is quite rare which can be developmental or acquired. Clefts or aplasias of anterior and posterior arches of atlas, ossification of the transverse atlantal ligament, hypertrophy of the dens and os odontoideum are rare conditions causing cervical myelopathy reported either singly or in combination [1-4]. Hypertrophy of the posterior arch of atlas in the absence of any ring hypoplasia as a cause of cervical myelopathy has not been reported earlier. The authors report a case of cervical myelopathy in a 26-year-old female due to hypertrophied posterior arch of atlas which was preoperatively diagnosed as a bony tumor.
Case Report
A 26-year-old female presented with complaints of posterior cervical headaches for many years with on and off tingling and numbness involving right arm, trunk, and leg. There was no history of bowel or bladder dysfunction. There was no significant past medical history or preceding trauma. The general physical examination was within normal limits. Neurological examination revealed presence of subtle spastic hemiparesis on the right side (Medical Research Council grade 4+/5) with exaggerated deep tendon reflexes as compared to left. She has positive right Hoffmann's sign. Computed tomography scan of the cervical spine revealed slight kyphosis and degenerative changes within the subaxial cervical spine with an expanded hyperostotic right posterior arch of C1 (Fig. 1). Magnetic resonance imaging of the cervical spine showed constriction of the dural sac with presence of possible right posterior arch of C1 lesion which was hypointense on T1 and T2W images and no contrast enhancement with a small area of increased signal within the spinal cord on the T2 weighted imagesb (Fig. 2). The patient was referred to us with a diagnosis of a benign bony tumor of C1 and a surgical removal was performed. Tc-labeled bisphosphonate nuclear bone scan performed did not reveal any abnormal focal uptake by the lesion which has been described in osteoid osteomas of the spine. Considering the dubious nature of the lesion with equivocal diagnosis, surgical resection was planned. Posterior exposure of the cervical spine in the C1-C2 regions was performed. There was no obvious anomaly seen externally with a normal appearing ligamentum flavum. The right posterior arch of the atlas was hypertrophied with no other abnormality suggestive of neoplastic lesion. The lesion was excised with performance of right hemilaminectomy of the atlas carefully preserving the C1/C2 joint. Final histopathology of the lesion showed the presence of normal bone tissue with no evidence of tumor confirming the diagnosis of hypertrophied posterior arch of atlas. Patient had an uneventful postoperative course with CT showing good decompression and excellent clinical outcome which was maintained at 3 months follow-up.

Bony window of axial (A) and sagittal right paramedian (B) computed tomography scan of the cervical spine showing presence of an hypertrophied right posterior arch of C1 (arrow) with narrowing of the canal diameter as compared to the normal (arrow) left sided posterior arch of atlas (C).
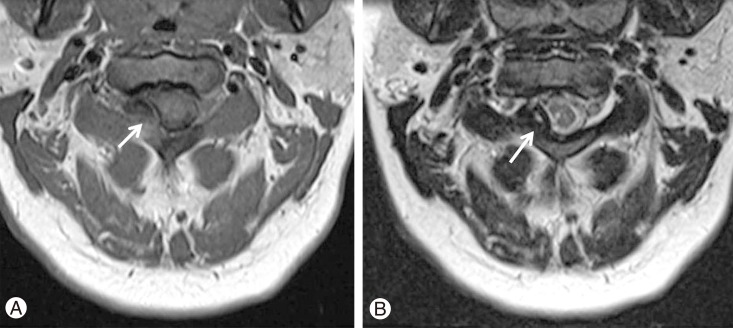
Axial T1W (A) and T2W (B). Magnetic resonance imaging of the cervical spine showed constriction of the dural sac with presence of right posterior C1 arch lesion which was hypointense on T1 and T2W images (arrows) with area of increased signal within the spinal cord on the T2W weighted image.
Discussion
Congenital cervical stenosis as a cause of cervical myelopathy is a well recognized entity described mainly in the subaxial cervical spine. Developmental anomalies at the level of atlas reported in the literature include various clefts or aplasias of anterior and posterior arches of atlas and os odontoideum, both of which can result in myelopathy [4]. Other than these anomalies, hypoplasia with an intact posterior arch of the atlas, ossification of the transverse atlantal ligament and hypertrophy of the dens are rare anomalies have been reported as causes of cervical myelopathy either alone or in combination [1-4]. A case of hypertrophied posterior arch as a primary cause of cervical myelopathy in the absence of ring hypoplasia has not been reported earlier.
Congenital canal stenosis due to a narrow but complete posterior arch of atlas has been described as a cause of cervical myelopathy. Hypertrophy of the dens or transverse atlantal ligament superimposed on a hypoplastic posterior arch can predispose to development of cervical myelopathy [2-4]. Trauma in the form of occipital injury has been implicated in cases of cervical myelopathy due to hypertrophied of the dens [2]. The present case remains distinct as the antero-posterior diameter of the canal was within normal range and there was an isolated presence of hypertrophied posterior arch of the atlas leading to development of myelopathy. Though the radiological findings were non-specific and unusual, the patient was referred to us with a diagnosis of a benign neoplastic bony tumor. Lack of presence of well-delineated nodular bone-forming tumor as described in osteoid osteoma with presence of essentially normal bone tissue on histopathology confirmed the diagnosis of a hypertrophied bony lesion. Wider en bloc resection with potential instability can be potential pitfall of misdiagnosing this lesion as a possible neoplasm.
Though not absolute, lack of increased uptake on the nuclear scan before surgery and absence of any abnormality of the ligamentum flavum intraoperatively are the pointers against presence of osteoid osteom and ossified ligament flavum and indicated the presence of a benign bony hypertrophy. Goel et al. [5] reported a series of four cases of unilateral lateral mass hypertrophy who presented with torticollis and progressive myelopathy hypothesizing the presence of some congenital entity. The lateral mass in our cases were normal with the hypertrophy being restricted to the posterior arch causing eccentric dural compression resulting in myelopathy. Though there was no obvious history of trauma in the past, subtle injury with periosteal reaction and thickening/hypertrophy of the posterior arch appears to be the most plausible mechanism for it. Intact and smooth cortical margins of the expanded posterior arch as present in this case may be a feature indicating the presence of benign C1 posterior arch hypertrophy rather than a tumor.
To conclude, an unusual case of cervical myelopathy due to hypertrophied posterior arch with complete atlas ring is reported which can be misdiagnosed as a neoplasm leading to redundant investigation and management dilemmas. Being aware of such an entity may avoid diagnostic surprises and facilitate patient prognostication and management.