Eleven Levels of Spinous Process Fractures in Thoracolumbar Spine
Article information
Abstract
Cases of over 5-level spinous process fractures are extremely rare. Thoracolumbar region of spine is superimposed on ribs; and as such additional studies such as computerized tomography are needed to diagnose fractures in this region. We report a case of 11 contiguous level thoracolumbar spinous process fractures, which has been treated conservatively.
Introduction
Isolated spinous process injury on thoracolumbar vertebral fractures is rare [1], and especially few multilevel spinous process fractures have been reported [1]. The reported mechanisms of injury are stress fractures from playing golf [2,3,4] and direct trauma of traffic accident [5]. Thoracolumbar region is superimposed on the ribs, and as such it is difficult to diagnose fractures on this region by simple X-ray [1]. Often additional studies such as computed tomography (CT) scan are necessary. The management of multilevel spinous process fractures is not clear. We report a case of multilevel (11-level) thoracolumbar spinous process fractures, treated conservatively.
Case Report
A 47-year-old man was admitted to our emergency department with back pains, after a 7 m-fall injury. He complained of severe back pains of visual analog scale (VAS) score 8, and had no past medical history. On physical examination, localized tenderness was checked from upper thoracic area to lower back area. He had neither ecchymosis nor swelling of the back, and was without neurological deficits. There were no significant fractures on simple lateral thoracic and lumbar X-ray (Fig. 1). We performed CT scans, which revealed the following: spinous process fractures on T6-L5 (Fig. 2); both transverse process fractures on T2 to T8, L1 and L5; and left transverse process fractures on C6-T1, T12, and L2-L4. There was neither compression fracture of vertebral body nor encroaching of vertebral canal. To evaluate posterior column of thoracolumbar vertebrae, magnetic resonance imaging (MRI) was performed. On MRI was seen the injury of superficial half on interspinous ligaments from T6 to L5, but the deep half was well-maintained continuously (Fig. 3).
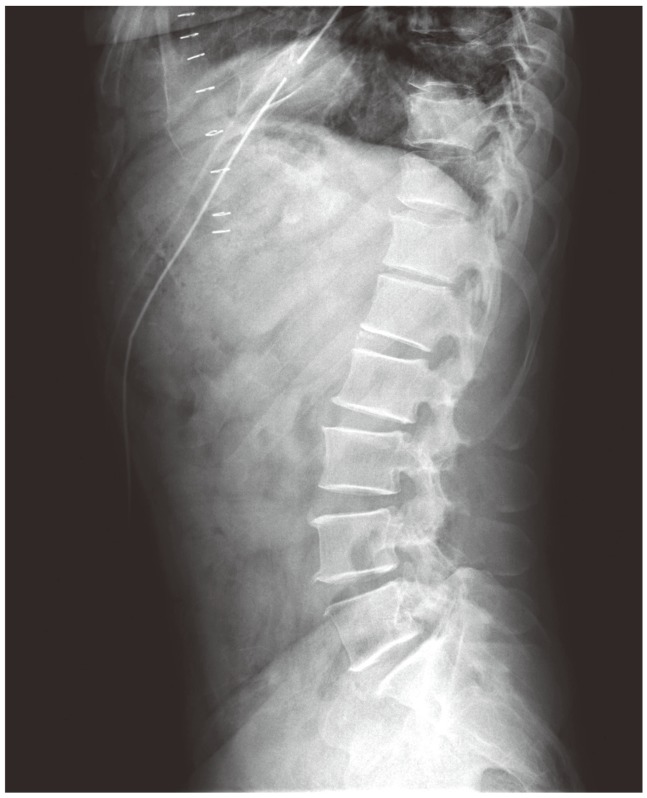
Simple lateral thoracolumbar X-ray.
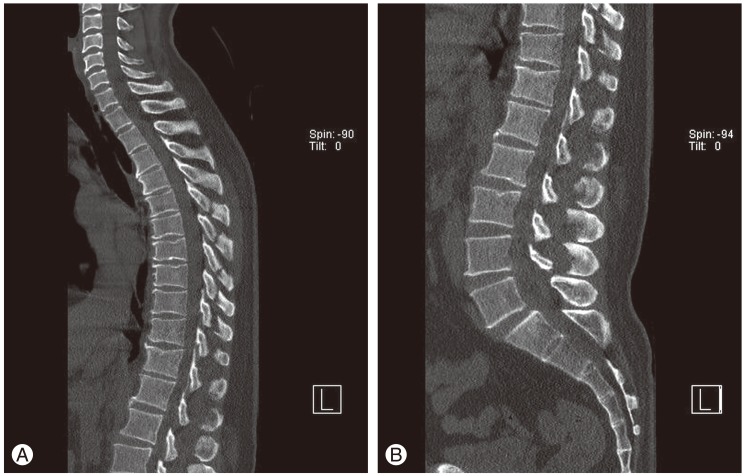
Sagittal view of computed tomography of (A) thoracic spine and (B) lumbar spine. It's found that multiple spinous process fractures, T6-L5, are continued.
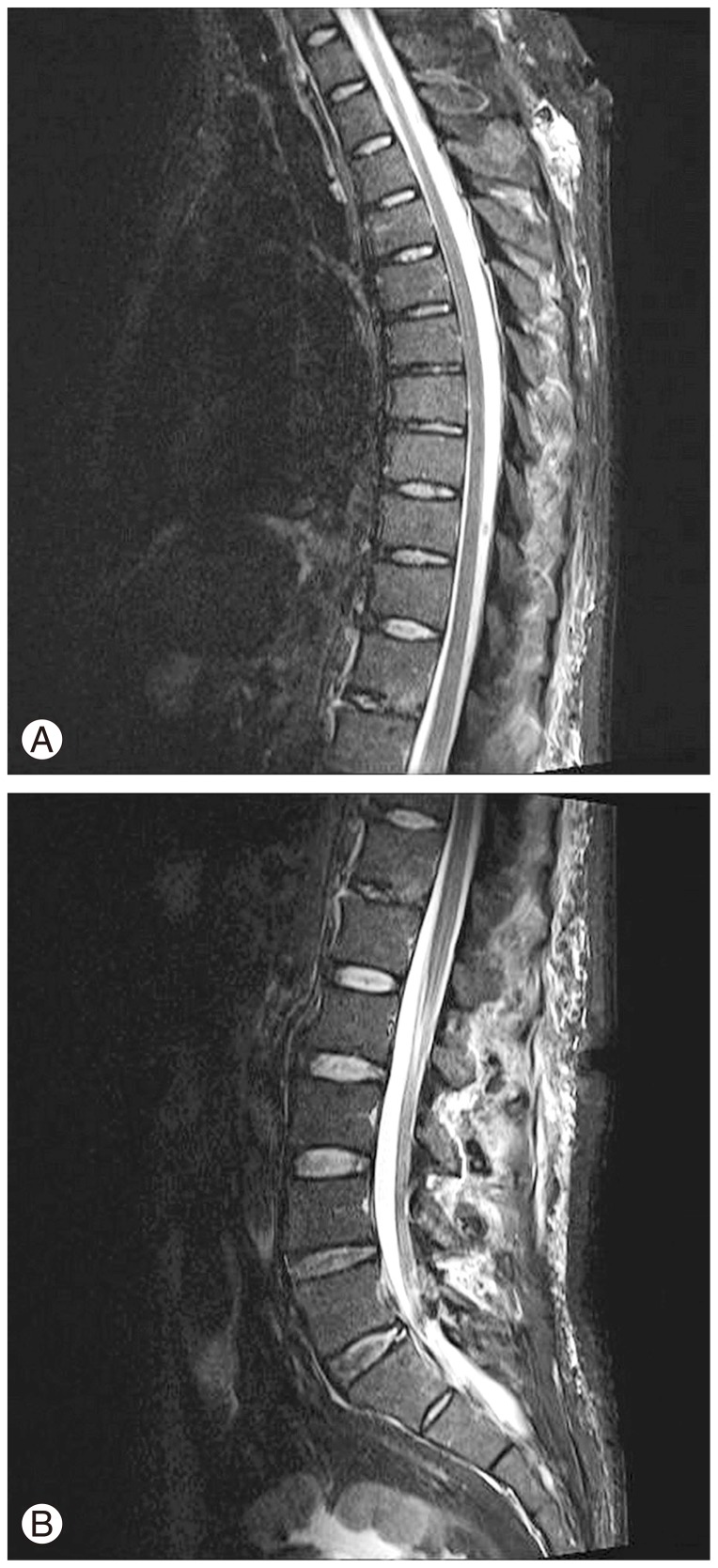
Sagittal view of magnetic resonance imaging of (A) thoracic spine and (B) lumbar spine. Deep part of interspinous ligament is intact and well connected.
The patients was treated conservatively by thoracolumbosacral orthosis (TLSO) for four-week and discharged. On the six-week follow-up, the standing whole spine lateral X-ray showed 20° thoracolumbar kyphosis and 57° lumbar lordosis (Fig. 4). VAS score was improved to 2, and the patient was satisfied with the improved symptoms. He was recommended to medication and TLSO-wearing for further six weeks.

Standing whole spine lateral X-ray. It seems well maintained in a sagittal balance of thoracolumbar spine.
Discussion
Isolated spinous process fractures are rare. Clay-Shoveler's fracture (an isolated spinous process fractures of the cervical or thoracic vertebrae) was first reported in 1997 [2]. Such fractures may occur by direct trauma or shear forces on flexed back [1,2,3,4,5]. Our case may have occurred by direct trauma after a 7-m fall. On literature, cases of over 5-level spinous process fractures were extremely rare; and all were treated conservatively [1,2,3,4,5,6].
Our case differed from other cases, as being multilevel thoracolumbar fractures involving only posterior column and especially 11 contiguous level spinous process fractures. Thoracic spinous process fractures are difficult to diagnose by simple X-ray only, because of the superimposing ribs. As such, CT scans is recommended to be performed to diagnose the easily-missed fractures. We performed CT scans and MRI to evaluate morphology and integrity of injury, and were able to diagnose accurately.
According to Farcy's sagittal index and Vaccaro's classification [7,8,9], these injuries are regarded as stable fractures and can be treated by conservative methods. We prescribed pain medication and applied TLSO for twelve-weeks. The follow-up whole spine lateral X-ray demonstrated neither kyphotic nor lordotic changes on sagittal balance.
Notes
No potential conflict of interest relevant to this article was reported.