Remodeling of Epidural Fluid Hematoma after Uniportal Lumbar Endoscopic Unilateral Laminotomy with Bilateral Decompression: Comparative Clinical and Radiological Outcomes with a Minimum Follow-up of 2 Years
Article information
Abstract
Study Design
Retrospective cohort study.
Purpose
To evaluate the clinical and radiological effects of epidural fluid hematoma in the medium term after lumbar endoscopic decompression.
Overview of Literature
There is limited literature comparing the effect of postoperative epidural fluid hematoma after uniportal endoscopic decompression.
Methods
Magnetic resonance imaging (MRI) and clinical evaluation were performed for patients with single-level uniportal endoscopic lumbar decompression with a minimum follow-up of 2 years.
Results
A total of 126 patients were recruited with a minimum follow-up of 26 months. The incidence of epidural fluid hematoma was 27%. Postoperative MRI revealed a significant improvement in the postoperative dura sac area at postoperative day 1 and at the upper endplate at 6 months in the hematoma cohort (39.69±15.72 and 26.89±16.58 mm2) as compared with the nonhematoma cohort (48.92±21.36 and 35.1±20.44 mm2), respectively (p<0.05); and at the lower endplate on postoperative 1 day in the hematoma cohort (51.18±24.69 mm2) compared to the nonhematoma cohort (63.91±27.92 mm2) (p<0.05). No significant difference was observed in the dura sac area at postoperative 1 year in both cohorts. The hematoma cohort had statistically significant higher postoperative 1-week Visual Analog Scale (VAS; 3.32±0.68) pain and Oswestry Disability Index (ODI; 32.65±5.56) scores than the nonhematoma cohort (2.99±0.50 and 30.02±4.84, respectively; p<0.05). No significant difference was found at the final follow-up VAS, ODI, and MRI dura sac area.
Conclusions
Epidural fluid hematoma is a common early postoperative MRI finding in lumbar endoscopic unilateral laminotomy with bilateral decompression. Conservative management is the preferred treatment option for patients who do not have a neurological deficit. Symptoms last only a few days and are self-limiting. A common endpoint is a remodeled fluid hematoma and the subsequent expansion of the dura sac area.
Introduction
The high prevalence of spinal stenosis is the leading cause of neurogenic claudication in the aging population. A proportional increment of open and minimally invasive spinal decompressive surgeries is performed.
Endoscopic spinal equipment and techniques have advanced, allowing more types of degenerative lumbar procedures to be performed with spinal endoscopy [1–3].
One of the most recent minimally invasive techniques for decompression of lumbar spinal stenosis has been described in the literature as lumbar endoscopic unilateral laminotomy with bilateral decompression (LE-ULBD) [4,5]. Several authors showed good clinical outcomes in patients who underwent LE-ULBD [5–7]. Epidural hematoma is a well-known dreaded complication of open spine surgery that leads to neurological sequelae, prolonged hospital stay, and higher incidence of revision surgery [8–10]. However, the incidence and consequences of postoperative epidural fluid hematoma after uniportal LE-ULBD are poorly documented. The purpose of this study is to compare the clinical and radiological parameters of patients who had LE-ULBD complicated by epidural fluid hematoma to those who did not have the complication of epidural fluid hematoma.
Materials and Methods
1. Indication and inclusion and exclusion criteria
Informed consent was obtained from all patients who participated in this retrospective comparative cohort study. The study protocol was reviewed by the institutional review board of Nanoori Hospital (NR-IRB 2021–009). All procedures performed in studies involving human participants were in accordance with the ethical standards of the Nanoori Hospital’s Ethics Committee and the national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
We included patients who suffered from neurogenic claudication who had failed a minimum of 6 weeks of conservative treatment. They had concordant magnetic resonance imaging (MRI) signs of spinal stenosis. A single-level uniportal LE-ULBD was performed on each patient.
We excluded patients who had surgery, those with a history of spine surgery, trauma, tumor, pseudoarthrosis, infection, vascular claudication, spondylolisthesis with a slip grade greater than grade 1, sagittal and coronal malalignment, and congenital spinal stenosis.
2. Technique of LE-ULBD
The detailed technique of LE-ULBD has been discussed in various studies [5–11]. The patient was placed in a prone position under general anesthesia. The skin was incised, and a working retractor cannula was inserted after serial dilation. The uniportal endoscope was inserted into the laminofacet junction of the affected level’s symptomatic side. Bony decompression was performed in the following sequence: (1) we started with the lower part of cephalad lamina, (2) the inferior articular facet, (3) the superior articular facet, (4) the top part of the caudal lamina, (5) the contralateral ventral portion of cephalad laminar, (6) the contralateral top part of the caudal lamina, and (7) the contralateral medial portion of a superior articular facet. After bony decompression, the ligamentum flavum was removed with endoscopic pituitary forceps and Kerrison rongeurs. Endoscopic decompression adequacy was assessed using an endoscope, with pulsating dura visible under endoscopic vision (Fig. 1). After hemostasis was achieved, a drain was placed in each case, and the skin was closed in layers.
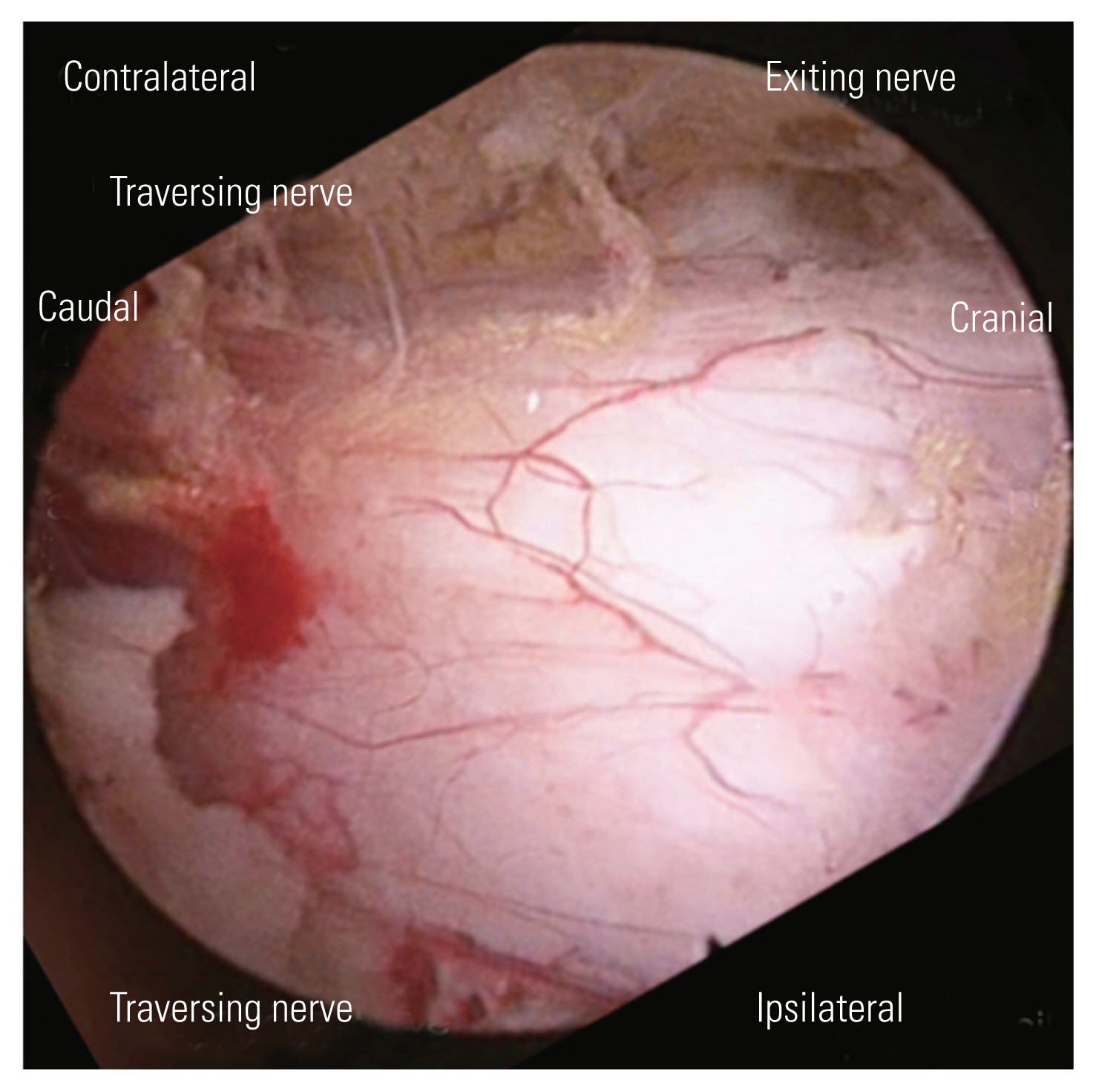
Intraoperative endoscopic picture of right L4/5 lumbar endoscopic unilateral laminotomy with bilateral decompression. There is good visualization of bilateral traversing nerve roots and pulsating dura under endoscopic fluid irrigation.
3. Collection of operative, clinical, and radiological data
Retrospective data were collected in the cohort of patients who underwent single-level LE-ULBD from September 2018 to December 2019. Baseline demographic and intraoperative data were collected. We measured clinical outcomes with the Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) score at preoperative, 1 week postoperative, 3 months postoperative, and final follow-up. MacNab’s criteria were evaluated at the final follow-up. We defined symptomatic epidural fluid hematoma as patients who presented with a VAS score >4 in the lower back and leg on postoperative 1 week, with a postoperative day 1 MRI scan demonstrating epidural fluid hematoma. At the operative level, we measured the MRI axial cut dura sac areas in the upper endplate, mid-disc, and lower endplate preoperatively, and at postoperative day 1, 6 months, and 1-year intervals (Fig. 2). All the measurements were taken on T2-weighted axial images parallel to the disc space at the level of surgery using an INFINITT PACS M6 version (INFINITT Healthcare Corp., Seoul, Korea). The dura sac area was measured at these axial cuts (Figs. 3, 4).
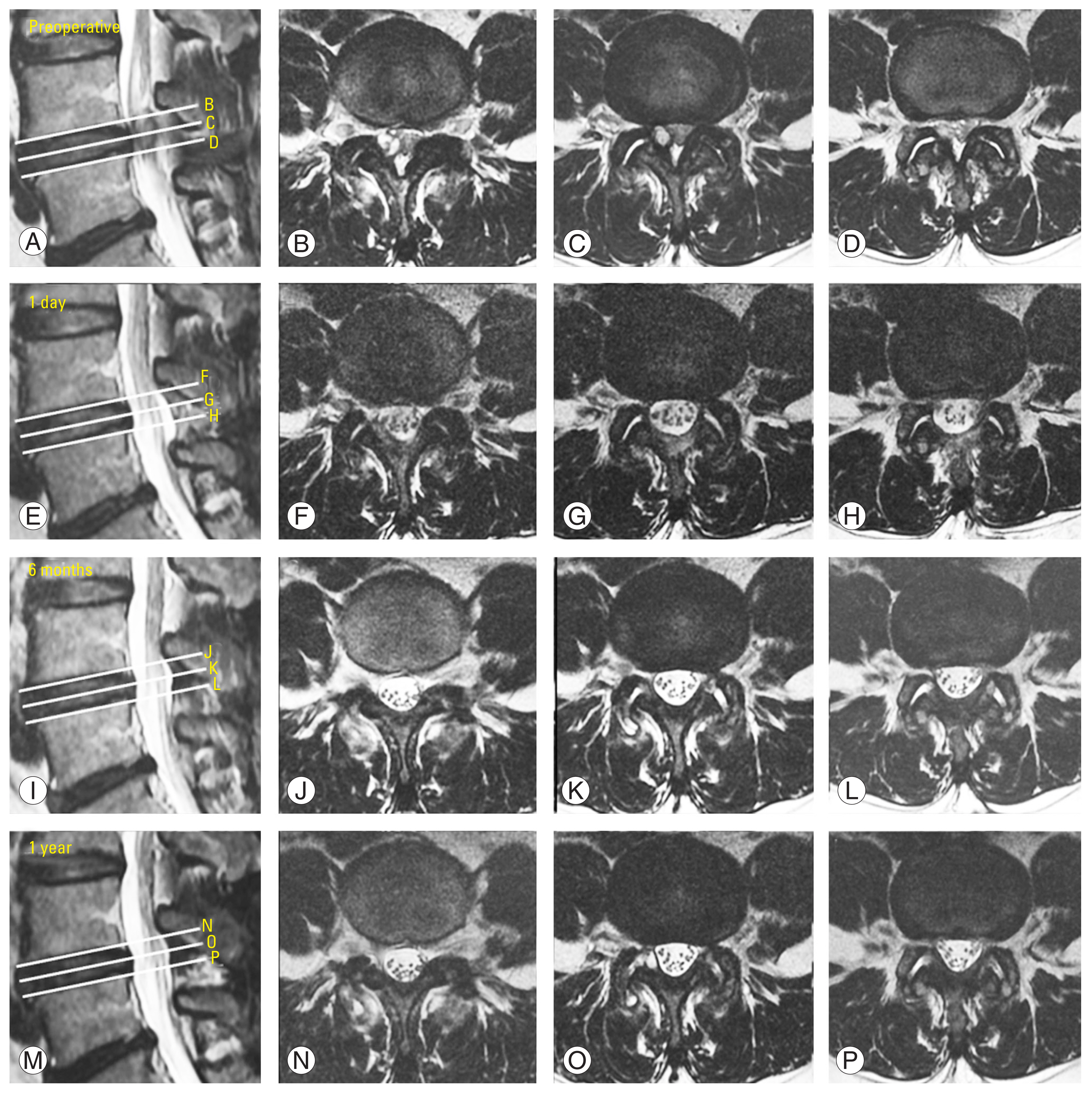
Preoperative and postoperative radiographic magnetic resonance imaging axial cut dura sac area in upper endplate, mid-disc and lower endplate at preoperative, postoperative day 1, 6 months, and 1 year intervals in a patient who underwent lumbar endoscopic unilateral laminotomy with bilateral decompression at L4/5, he had no postoperative hematoma. (A–D) Preoperative upper endplate axial cut, mid-disc, and lower endplate axial cut, respectively. (E–H) Postoperative day 1 upper endplate axial cut, mid-disc, and lower endplate axial cut, respectively. (I–L) Postoperative 6 months upper endplate axial cut, mid-disc, and lower endplate axial cut, respectively. (M–P) Postoperative 1 year upper endplate axial cut, mid-disc, and lower endplate axial cut, respectively.

(A) Preoperative magnetic resonance imaging (MRI) mid-disc axial cut of a patient with right facet cyst and spinal canal stenosis at L4/5, his dura sac area measured at 50.69 mm2, he underwent lumbar endoscopic unilateral laminotomy with bilateral decompression. (B) Postoperative day 1 MRI mid-disc axial cut of the same patient who did not have postoperative hematoma, his dura sac area measured at 155.76 mm2. (C) Postoperative 6 months MRI mid-disc axial cut of the same patient, his dura sac area measured at 151.68 mm2. (D) Postoperative 1 year MRI mid-disc axial cut of the same patient, his dura sac area measured at 135.49 mm2. SD, standard deviation.

(A) Preoperative magnetic resonance imaging (MRI) mid-disc axial cut of a patient with spinal canal stenosis at L4/5, his dura sac area measured at 50.69 mm2, he underwent lumbar endoscopic unilateral laminotomy with bilateral decompression. (B) Postoperative day 1 MRI mid-disc axial cut of the same patient who had postoperative epidural fluid hematoma, his dura sac area measured at 68.73 mm2. (C) Postoperative 6 months MRI mid-disc axial cut of the same patient, his postoperative epidural fluid hematoma had resolved, his dura sac area measured at 107.30 mm2. (D) Postoperative 1 year MRI mid-disc axial cut of the same patient, his dura sac area measured at 107.43 mm2. SD, standard deviation.
4. Statistical analyses
Clinical data were analyzed using PASW SPSS ver. 18.0 statistical analysis software (SPSS Inc., Chicago, IL, USA). The continuous variables were expressed as the mean and standard deviation. The paired t-test was used for comparisons of preoperative and postoperative radiological MRI results on digital subtraction angiography. Clinical parameters as well as VAS and ODI scores were analyzed using the paired t-test. A value of p<0.05 was considered significant within each group of data. The clinical data of VAS, ODI, and MRI results were compared using independent t-tests between the epidural fluid hematoma cohort and the nonhematoma cohort.
Results
1. Baseline demographics
From the period of February 2018 to December 2019, a total of 126 single-level LE-ULBDs were performed in 126 patients who met the inclusion criteria. The mean age of patients was 63.8 years (range, 21–86 years), with a mean follow-up of 27.6 months (range, 17–38 months). The incidence of epidural fluid hematoma was 27.0% (34/126). There were 4 (11.7%) intraoperative complications, all of which were incidental durotomies in the epidural fluid hematoma cohort. There were 5 (5.4%) intraoperative complications, including four incidental durotomies and one transient cauda equina syndrome, in the nonhematoma cohort.
There was one case of transient cauda equina that lasted 24 hours and was resolved without complications.
The patch blocking repair technique was used to repair all durotomies [12]. Two patients (5.8%) developed late complications in the epidural fluid hematoma cohort; one patient had symptomatic incomplete decompression, and the patient was treated conservatively. One patient experienced spinal instability following decompression and underwent uniportal endoscopic posterolateral transforaminal lumbar interbody fusion 1 year later [13,14]. There were 11 (9.1%) late complications in the nonhematoma cohort. Three patients had postoperative facet cysts; two of these three patients underwent revision LE-ULBD at 6 months postoperatively, and one was treated conservatively. There were four cases of restenosis. One patient underwent transforaminal endoscopic lumbar decompression 1 year after index surgery, and three patients were treated conservatively. Within 1 year of decompression, four patients with spinal instability following index surgery underwent uniportal endoscopic posterolateral transforaminal lumbar interbody fusion. In terms of complications, there was no statistical difference between the two cohorts.
There was no statistical difference between the baseline parameters (Table 1). There were no statistical differences with regard to comorbidities and medical treatment in both cohorts (Table 2).
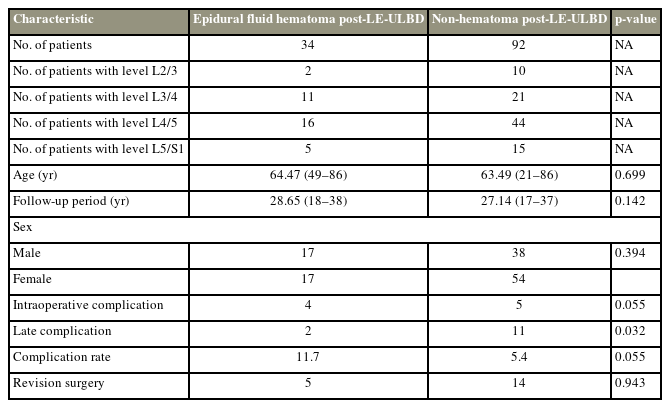
Baseline demographics data of epidural fluid hematoma cohort compared with non-hematoma cohort post LE-ULBD

Evaluation of medical comorbidities and confounding factors in epidural fluid hematoma cohort compared with non-hematoma cohort
When we compared clinical and radiographic preoperative measurements, there was no statistical difference between the two cohorts in terms of preoperative VAS, ODI, and dura sac area (p>0.05).
At postoperative 1 week, the epidural fluid hematoma cohort had a significantly higher VAS score (3.32±0.68) than the nonhematoma cohort (2.99±0.50) (p<0.05). The ODI was also significantly higher in the epidural fluid hematoma cohort (32.65±5.56) than in the nonhematoma cohort (30.02±4.84) (p<0.05). In terms of postoperative MRI measurements in the lower endplate axial cut, there was a significantly smaller postoperative dura sac area in the epidural fluid hematoma cohort at 1 day (122.94±30.17 mm2), 6 months (117.76±31.56 mm2), and 1 year (118.12±34.04 mm2) than in the nonhematoma cohort at 1 day (149.88±42.31 mm2), 6 months (138.28±41.02 mm2), and 1 year (139.66±41.47 mm2) (p<0.05). There was no statistically different dura sac area in the upper endplate and mid-disc at postoperative 1 day, 6 months, and 1 year (Table 3).

Radiographic and clinical parameters of epidural fluid hematoma cohort compared with non-hematoma cohort
2. Clinical and radiological results of the epidural fluid hematoma cohort
In terms of clinical results for the epidural fluid hematoma cohort, there were three patients with symptomatic epidural fluid hematoma. All three patients had VAS pain scores of 5 in the back and leg. They did not present with neurological symptoms, and their pain was relieved after 3 months of conservative treatment.
There was a significant improvement from the preoperative state at postoperative 1 week, postoperative 3 month, and final follow-up; the VAS scores were 4.47±1.13, 5.32±1.27, and 5.62±1.35, respectively (p<0.05). There was a significant improvement from the preoperative state at postoperative 1 week, postoperative 3 months, and final follow-up, with the mean ODI and range of 42.23±8.12, 48.41±9.00, and 50.82±9.57, respectively (p<0.05) (Table 4).

Clinical and radiographic parameters of hematoma post-LE-ULBD
In terms of radiographic results, there was a significant improvement in the dura sac area at postoperative day 1, 6 months, and 1 year MRI compared to the preoperative state. The improvements at the final follow-up at the upper endplate, mid-disc, and lower endplate measured 35.43±16.09, 56.72±23.38, and 46.36±23.56 mm2, respectively (p<0.05) (Table 4).
3. Clinical and radiological results of the nonhematoma cohort
In terms of clinical results for the nonhematoma cohort, there was a significant improvement from the preoperative state at 1 week postoperative, 3 months postoperative, and final follow-up, with VAS scores of 4.55±1.42, 5.18±1.62, and 5.39±1.78, respectively (p<0.05). There was a significant improvement from the preoperative state at 1 week postoperative, 3 months postoperative, and final follow-up, with ODI values of 42.61±10.65, 46.22±10.66, and 47.89±11.16, respectively (p<0.05) (Table 5).
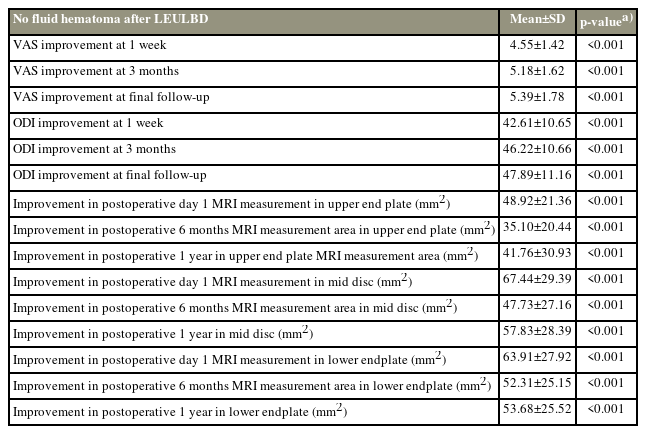
Clinical and radiographic parameters of no fluid hematoma post-LE-ULBD
In terms of radiographic results, there was a significant improvement in the dura sac area at postoperative day 1, 6 months, and 1 year MRI compared to the preoperative state. The improvements at the final follow-up at the upper endplate, mid-disc, and lower endplate measured 41.76±30.93, 57.83±28.39, and 53.68±25.52 mm2, respectively (p<0.05) (Table 5).
4. Comparative clinical and radiological results between epidural fluid hematoma and nonhematoma cohorts
In terms of clinical results comparing epidural fluid hematoma with nonhematoma cohorts, there was no significant difference in the amount of clinical improvement from the preoperative state at 1 week postoperative, 3 months postoperative, and final follow-up in terms of VAS scores and the ODI (Table 6).
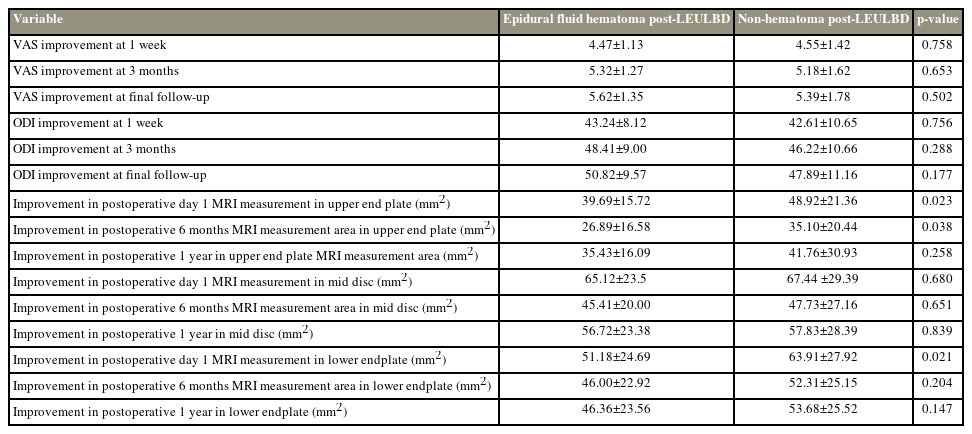
Comparative clinical and radiographic parameters of epidural fluid hematoma and non-hematoma post-LEULBD
In terms of radiographic results, there was significantly less improvement in dura sac area expansion at the upper endplate axial cut MRI in the epidural fluid hematoma cohort (39.69±15.72 and 26.89±16.58 mm2) than in the nonhematoma cohort (48.92±21.36 and 35.1±20.44 mm2) at postoperative day 1 and 6 months, respectively (p<0.05). There was significantly less improvement in dura sac area expansion at the lower endplate axial cut MRI in the epidural fluid hematoma cohort (26.89±16.58 mm2) than in the nonhematoma cohort (63.91±27.92 mm2) at postoperative day 1. There was no statistical difference, despite a trend of lower dura sac area measured at other timelines and locations (Table 6).
Discussion
With the improvement of endoscopic equipment and techniques, an increasing number of lumbar endoscopic decompressions are performed for spinal stenosis [3,5,15]. Shorter hospital stay, less perioperative pain, and less blood loss are the promising benefits of endoscopic surgery [16]. Patients who had undergone LE-ULBD did not have any neurological symptoms, and their pain was relieved after 3 months of conservative care [4,5,17,18]. The limited literature evaluating the radiographic efficacy of LE-ULBD using cross-sectional area increment measurements demonstrates statistically significant increments in spinal canal parameters [6,19,20]. However, one of the limiting factors of endoscopic spine surgery is the steep learning curve.
The use of an arthroscope in biportal endoscopic spine surgery (BESS) and an endoscope in uniportal endoscopic spine surgery is not a standard curriculum in spinal residency [21,22]. Although the literature supporting the use of irrigation fluid in surgery in arthroscopic orthopedic limb surgeries is well established, the literature in spinal endoscopy is still evolving [3]. One of the dreaded complications of endoscopic spine surgery is the development of an epidural fluid hematoma [23,24]. Although it is a known and common complication, Ebata et al. [25] found that the incidence of epidural hematoma does not decrease with more experience in spinal endoscopy.
Epidural fluid collection is a common finding after endoscopic spine surgery. The use of saline under 25–40 mm Hg irrigation pressure can result in the discovery of a fluid hematoma early after surgery.
After endoscopic lumbar discectomy, Liu et al. [26] found an epidural fluid collection rate of 90.1% on early postoperative MRI. The vast majority of their cases were resolved over time, without the need for treatment or complications. In their series, no medium- or long-term clinical or radiological data are provided [26].
Kim et al. [24] showed that 24.7% of their patients who underwent single-level BESS for spinal stenosis had epidural hematoma, with 3.2% requiring revision decompression and evacuation of hematoma for neurologic symptoms. The same group of surgeons looked at the use of a gelatin–thrombin matrix sealant after BESS and discovered that it helps to reduce the rate of postoperative spinal epidural hematoma, with improved clinical outcomes in MacNab criteria but not in VAS back pain [27]. The perioperative risk factors of postoperative hematoma in BESS include old age >70 years, female, preoperative anticoagulation medication, usage of intraoperative water infusion pump, and surgery requiring more bone work (laminectomy and interbody fusion) [23].
Although any epidural fluid hematoma after open spine surgery is likely due to blood clot formation [28], the incidence of epidural fluid hematoma in MRI performed at less than 1 week after spinal surgery ranges from 33% to 100% [29,30]. However, the interpretation of the presence of epidural fluid hematoma in endoscopic spine surgery is more challenging. The use of irrigation fluid in endoscopic spine surgery correlates with a higher incidence of the presence of epidural fluid hematoma; in the limited literature, the incidence of hematoma ranges from 24.7% to 90.1% in uniportal endoscopic discectomy and biportal endoscopic decompression surgeries.
To the best of our knowledge, there is no medium- or long-term follow-up study on the effects of epidural fluid hematoma on the MRI dura sac area after LE-ULBD. In our cohort, we found that despite having less dura sac area expansion on postoperative day 1 and 6 months in the epidural fluid hematoma cohort than in the nonhematoma cohort, the difference was not significant at 1 year. One intriguing finding was that the dura sac area at the mid-disc level was not significantly affected in either the epidural fluid hematoma or the nonhematoma cohort, whereas it was significantly affected at the lower endplate level. Based on this finding, it appears reasonable to direct the drain toward the interlaminar space’s lower endplate region after LE-ULBD.
There are varying descriptions in the literature for a postoperative fluid hematoma in endoscopic spine surgery. Liu et al. [26] termed it “epidural fluid collection,” whereas Kim et al. [23,24] termed it “postoperative spinal epidural hematoma.” We believe that “epidural fluid hematoma” is the correct term to describe the fluid collection in the epidural space following endoscopic spine surgery, which is frequently an admixture of irrigation fluid and blood from the epidural space. In our series, patients who underwent LE-ULBD surgery had a 27.0% (34/126) incidence of epidural fluid hematoma. We felt that a standardized terminology would help to refine research in epidural fluid hematoma in spinal endoscopy in the future. A specific MRI protocol that differentiates the content of the epidural fluid hematoma as “more fluid dominant” or “blood clot dominant” would be helpful for endoscopic surgeons to evaluate the epidural fluid hematoma.
We have 8.8% of patients (3/34) with symptomatic epidural fluid hematoma, with VAS scores of 5 in the back and leg after the operation. Although they improved from the preoperative state, they had more pain than other patients in both cohorts, with a range of 0–4 VAS pain scores.
Through our operative experience in endoscopic decompression, we recommend the following steps for hemostasis during LE-ULBD: (1) keep the patient’s mean arterial pressure at around 70 mm Hg; (2) LE-ULBD should be performed on the Wilson frame, Jackson table, or Proaxis table, where there is free space for the abdomen; (3) maintain the irrigation pump at 25–40 mm Hg during surgery; (4) careful hemostasis of muscles around the bony lamina using radiofrequency ablation before performing bony decompression of the interlaminar space; (5) application of radiofrequency ablation for bone edge bleeding; (7) removal of the ligamentum flava only after bony decompression is completed as significant epidural bleeding would occur once the ligamentum flava are removed, which blurs the endoscopic visualization; and (8) application of radiofrequency ablation on epidural bleeders [5,11].
Despite epidural fluid hematoma being a common postoperative MRI finding, the symptoms associated with epidural fluid hematoma are mild and self-limiting in our series. All the patients with epidural fluid hematomas were treated conservatively because none of them developed neurological deficits. Patients with epidural fluid hematoma have a statistically significant higher VAS pain score and ODI value in the early postoperative period than the nonhematoma cohort in our series. However, at the final follow-up, both cohorts had made comparable and significant progress from their preoperative states. There was no statistically significant difference in clinical or radiological outcomes between the two cohorts at the end of this study.
There are several differences and possible confounding factors in this study: the data were obtained as a retrospective cohort study with subgroup analysis; hence, there could be inherent selection and performance bias in the study. As the authors in this study performed all cases of single-level stenosis with the endoscope, we limited the selection bias. Comorbidities, the Charlson Morrison Index, body mass index, non-steroidal anti-inflammatory drugs, anticoagulant use, and smoking history were not collected before surgery, which may have introduced confounders into the study. We limited these confounding factors by having the same team of anesthetists and surgeons for both cohorts of operations performed in the data set for both groups. The follow-up was of medium-term duration and we continued to follow-up on these patients to show the effect of a longer follow-up in the future to evaluate the clinical and radiological data in the long term.
Conclusions
Epidural fluid hematoma is a common early postoperative MRI finding in LE-ULBD. Conservative management is the treatment of choice for patients without neurological deficits. The duration of symptoms is short and self-limited. A remodeled fluid hematoma and the subsequent expansion of the dura sac area is a common end point.
Acknowledgments
We would like to acknowledge scientific team members, Ms. Seonghee Park and Mr. Kyeong Rae Kim for providing assistance in statistical support, acquiring full-text articles and managing digital works.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.