C2 Pars/Pedicle Screws in Management of Craniocervical and Upper Cervical Instability
Article information
Abstract
Study Design
A retrospective study.
Purpose
To evaluate the efficacy and the safety of craniocervical and upper cervical stabilization by using C2 pars/pedicle screw fixations.
Overview of Literature
The management of craniocervical and upper cervical instability has progressed over the past two decades due to good achievements in the instrumentation and the increased awareness on spinal anatomy and biomechanics. However, there is insufficient studies or solid conclusions on this topic, thus, we tried to investigate and present our findings.
Methods
Twenty-two patients were operated upon and were followed up from March 2008 to October 2010. One patient had craniocervical instability (post-surgical), 15 patients had atlantoaxial instability of different etiologies (trauma, tumors, inflammatory and degenerative) and 6 patients had hangman fractures. Patients' ages ranged from 18 to 52 years old. with 5 female patients and 17 male patients.
Results
Radiological follow ups performed immediately post-operation showed good screw positioning and complete reductions in nearly all the cases. All patients were followed up for more than one year. Sound fusions were observed among all patients.
Conclusions
The use of pars/pedicle screws is a very effective, sound, safe and easy surgical modality for treating craniocervical, atlantoaxial and upper cervical instabilities. Increasing studies for the biomechanics of this important region and longer periods of follow-ups are necessary to document the usefulness of this modality when treating such patients.
Introduction
C2 pars/pedicle screws have been a good and sound way of fixation during posterior upper cervical spine surgery [1,2]. The use of the pedicle and pars of C2 as a part of complex upper cervical spine, has allowed spine surgeons to use these structures for fixation of the anterior and posterior segments of the C2 vertebra, as in cases of Hangman's fractures [3,4,5].
Nowadays craniocervical instability is treated with an occipital plate with a C1 lateral mass and C2 pars/pedicle screws using polyaxial screw-rod fixation, atlantoaxial instability with a C1 lateral mass and C2 pedicle screws, and Hangman's fracture is treated by C2 pars screws with or without C3 lateral mass screws and rods. Atlantoaxial stabilization with a C1 lateral mass and C2 pars/pedicle screws has other advantages over the transarticular screws such as the ease of performing the procedure and the possibility of intraoperative reduction. However, the advantages are without risk of vertebral artery (VA) injury [6,7]. The management of craniocervical and upper cervical instability has progressed over the past two decades due to good achievements in instrumentation and increased awareness about spinal anatomy and biomechanics. Posterior fixation of the cervical spine is a popular surgical procedure which is used in a variety of spinal disorders, such as cervical spondylosis, postsurgical deformity or instability, tumor, and trauma [8].
Materials and Methods
Twenty-two patients were operated upon and were followed up from March 2008 to October 2010. One patient had craniocervical instability (postsurgical), 15 patients had atlantoaxial instability of different etiologies (trauma, tumors, inflammatory, and degenerative) and six patients had Hangman's fracture. Patients' ages ranged from 18 to 52 years. Five female patients and 17 male patients. The patient who had craniocervical instability was operated upon by occipital plate fixation, C1 lateral mass screws and C2 pars/pedicle screws. Patients who had atlantoaxial instability were operated upon by C1 lateral mass screws and C2 pars/pedicle screws. Four patients who had Hangman's fracture were operated upon by C3 lateral mass screws and C2 pars/pedicle screws. Two patients who had Hangman's fracture were operated upon by C2 pars/pedicle screws only.
1. Surgical technique
Under general anesthesia using awake intubation and fiber optics guidance, the patient was put in the prone position with the neck neutralized, the head was fixed in a Mayfield and the arms were adducted to the body. A posterior midline skin incision was made from the suboccipital region to the C4 spinous process.
The lateral mass of C1, which lies below the lateral half of the C1 posterior arch, was palpated using a microdissector to detect the medial and lateral limits of this mass. The entry site for the C1 lateral mass was the midpoint between the medial and lateral edges. Under C-arm guidance, a high speed drill was used to penetrate the cortex at 15 degrees of medial inclination and direction towards the anterior tubercle of C1. The track was palpated using a micro sensor then tapped, and a polyaxial, 28 to 30 mm length, 3 mm, 5 mm diameter screw was inserted.
The C2 pars is located between the superior and inferior articular surfaces and its anterior continuation is the pedicle which is short, and is attached anteriorly and originates from the C2 body. The entry point for the C2 pars/pedicle screw is located 5 mm above and lateral to the inferomedial angle of the C2-3 facet joint. With a 10 to 15 degree medial inclination and 45 degree up-pointing toward the anterior C1 tubercle, the drilling was followed by tapping. We inserted a 16 mm polyaxial screw for the pars screw and a 30 to 32 mm for the pars/pedicle screw. In cases of Hangman's fracture, if there was much displacement or angulation (type 2 or 3 Hangman's fracture), this deformity was completely or partially reduced by skull/neck traction before screw insertion. Rods were refashioned to comply with the normal lordotic curve and then were applied over the screws. We decorticated the exposed surfaces of the C1 lamina and C2 lateral masses to accommodate the fragmented bony grafts. We closed in layers and applied suction drainage. Postoperatively, a hard Philadelphia neck collar was applied and maintained for 3 months. All patients were followed up clinically and radiologically for at least one year.
Results
No major intraoperative complications were encountered. A few postoperative complications in the form of superficial wound infection in 4 cases were treated conservatively. Pre- and postoperative data collection and analysis of the outcomes were completed based on the Oswestry Disability Index (ODI) and American Spine Injury Association (ASIA) Impairment Scale.
1. Oswestry Disability Index
The ODI was scored on a 0-100 scale using the Oswestry Low Back Pain Disability Questionnaire of ten items (personal care, lifting, walking, sitting, standing, sleeping, sex life, social life, travelling, and need for medications). On this scale, 0-20 equates to minimal disability, 21-40 moderate disability, 41-60 severe disability, 61-80 crippled, and 81-100 bed-bound or exaggerating.
The outcome was categorized as in the following: 1) poor outcome (ODI, 81-100): patients who experienced the same preoperative symptoms or worsening of the symptoms after surgery, with significant restriction of their daily living activities; 2) fair outcome (ODI, 61-80): pain had improved compared with the preoperative status but still requiring strong analgesics; evidence of mild improvement in sensory and motor symptoms but the patient still had some difficulty with daily living activities; 3) good (ODI, 41-60): Patients had moderate improvement in the back pain and sciatica, and only mild analgesics were required and only mild numbness and paresthesia experienced, with a noticeable improvement in the weakness. Little constraint in daily activities; 4) very good (ODI, 21-40): moderate improvement in the back pain and sciatica, no analgesics were required at any time and less numbness and paresthesia experienced, with no weakness. No constraint in daily activities anymore; 5) excellent (ODI, 0-20): No more pain or neurological deficits. Normal daily life activities and patient's satisfaction was more than 80%.
2. ASIA Impairment Scale
A) Complete: no motor or sensory function is preserved in the sacral segments S4-S5. B) Incomplete: Sensory but not motor function preserved below the neurologic level and includes the sacral segments S4-S5. C) Motor function is preserved below the neurologic level, and more than half of the key muscles below the neurologic level have a muscle grade less than 3. D) Incomplete: motor function is preserved below the neurologic level, and at least half of the key muscles below the neurologic level have a muscle grade of 3 or more. E) Normal: motor and sensory functions are normal.
There was no deterioration in the patients' clinical condition in any of the cases, whereas clinical improvement started in 80% of the cases. Radiological follow-up done in the immediate postoperative period confirmed good position of the screws. The criteria or definitions of "good screw position" entails the following [9]: 1) The C2 pedicle should be palpated using a fine dissector after removal of the soft tissues with no serrations palpated in the spinal canal. 2) No evidence of VA injury as intraoperative hemorrhage or postoperative neurological deterioration. 3) Intraoperative and postoperative radiological assessment showing complete reduction and screws observed passing through the C2 pedicle to the C2 body without breaching the cortex of the pedicle.
All patients were followed up for more than one year. Sound fusions were observed in all patients and confirmed by postoperative flexion-extension lateral radiographs (Figs. 1,2,3,4).

Intraoperative C-arm image showing an angulateddislocated C2 in this case of Hangman's fracture.
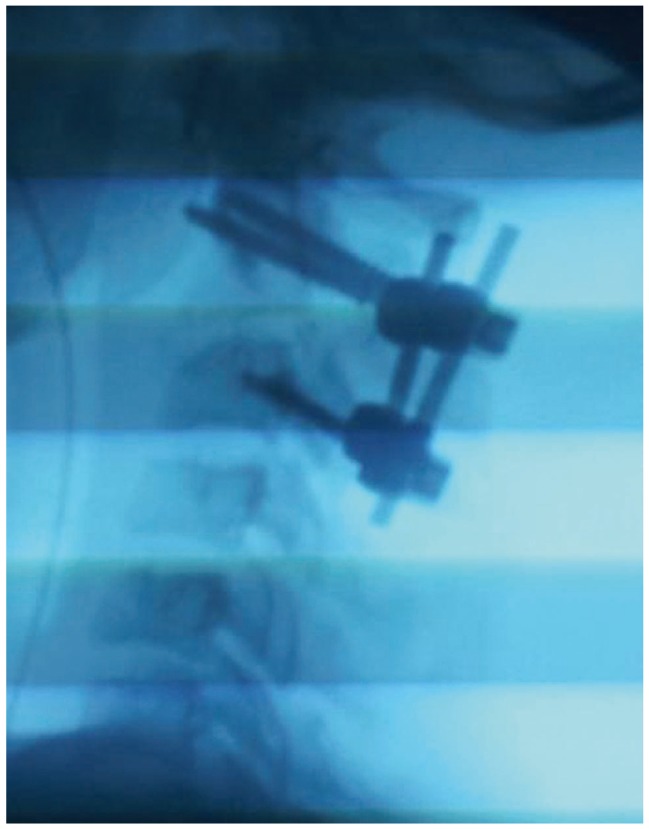
Nearly complete reduction with C2 pars screws and C3 lateral mass.

Dislocated C2 in the case of a Hangman's fracture.
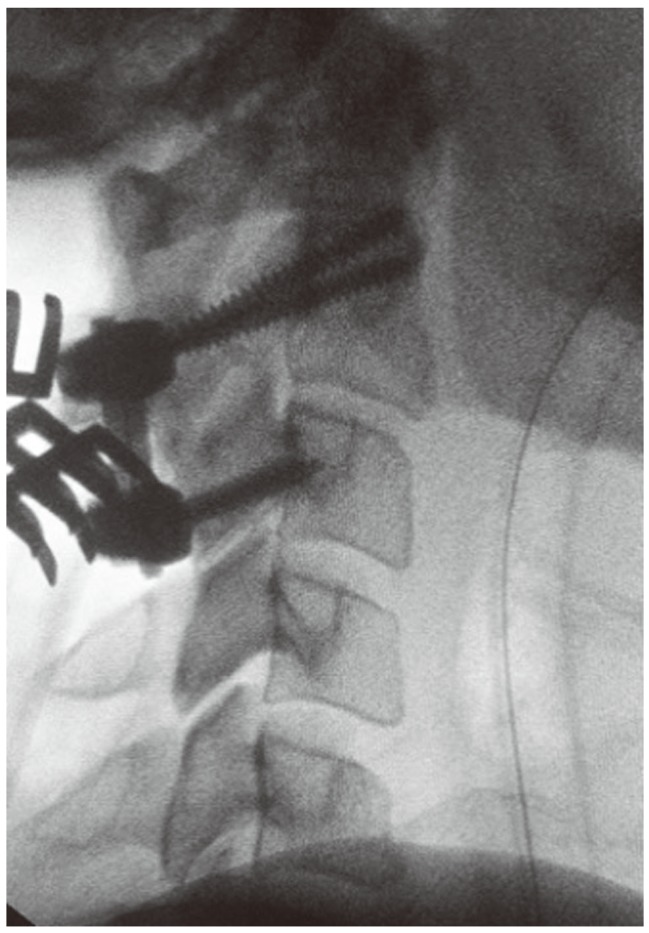
Complete reduction with C2 parsscrews and C3 lateral mass screws.
Discussion
Mixter and Osgood [10] have the first trials to fix C1 and C2 through the posterior approach using silk wires in 1910.
Goel and Laheri [11] and Gupta and Goel [12] were the first surgeons to try to fuse C1 and C2 from the posterior approach by inserting C1 lateral mass screws and C2 pars/pedicle screws. This procedure is done nowadays by the vast majority of spine surgeons. The many advantages of this technique include the allowance of 0.6 degrees more motion than with a C1-2 transarticular screw, anomalies in the VA course have no effect, and insertion of the C2 pars/pedicle screw gives a better bony grip that is more powerful than the C2 lateral mass [11,12].
In atlantoaxial subluxation, many surgeons use the posterior wiring technique, but it does not have sufficient rigidity, needs postoperative halo immobilization and needs an intact posterior arch of C1 and C2 [13].
Hangman's fracture can be treated through the anterior, transoral or extra oral approach, with violation of the C2-3 disc, and insertion of a bone graft and fixation of the 2 bodies using a cervical plate and screws. This approach sometimes is very difficult, especially in obese patients or patients with a short neck. In contrast, the posterior approach using pars/pedicle screws is easy and can be done in most of the patients [3,13]. In cases of Hangman's fracture treated by pars/pedicle screws only, the motion at the C2-3 segment is preserved and normal cervical lordosis is maintained [5,14]. If Hangman's fracture is associated with traumatic C2-3 disc herniation, some authors recommend trying the anterior approach [15].
In cases of high-riding VA or medially positioned VA, 16 mm pars screws are used (not reaching the pedicle) or laminar screws are employed [16].
The use of recent surgical techniques incorporating computer-assisted navigation systems increases the accuracy of C2 pedicle screw fixation. When such navigation is used, greater safety and accuracy may be achieved.
Finally, we spent much time and effort trying to produce good results and to clarify the efficacy of this new technique, with limited facilities, but the study lacked a large series, and longer periods of follow up are required.
Conclusions
The use of pars/pedicle screws is a very effective, sound, safe and easy to use surgical modality for treating craniocervical, atlantoaxial, and upper cervical instability. More studies on the biomechanics of this important region and longer periods of follow up are needed to document the usefulness of this modality of treating such patients.
Notes
No potential conflict of interest relevant to this article was reported.