Restoration of Lumbar Lordosis in Flat Back Deformity: Optimal Degree of Correction
Article information
Abstract
Study Design
A retrospective comparative study.
Purpose
To provide an ideal correction angle of lumbar lordosis (LL) in degenerative flat back deformity.
Overview of Literature
The degree of correction in degenerative flat back in relation to pelvic incidence (PI) remains controversial.
Methods
Forty-nine patients with flat back deformity who underwent corrective surgery were enrolled. Posterior-anterior-posterior sequential operation was performed. Mean age and mean follow-up period was 65.6 years and 24.2 months, respectively. We divided the patients into two groups based on immediate postoperative radiographs-optimal correction (OC) group (PI-9°≤LL<PI+9°) and under-correction (UC) group (LL<PI-9°). We also classified the patients according to the PI of each patient-low PI group (PI<55°) and high PI group (PI≥55°). Radiological and clinical results were analyzed.
Results
Patients in OC group had significantly less correction loss and maintained normal sagittal alignment (sagittal vertical axis<5 cm), as compared to patients in UC group (p<0.05). LL of low PI group significantly maintained within 9° better than high PI group (p<0.05). Oswestry disability index (ODI) significantly decreased at last follow-up, as compared to preoperative state. However, there was no significant difference in last follow-up ODI between the groups.
Conclusions
In flat back deformity, correction of LL to within 9° of PI will result in better sagittal balance. Thus, we recommend sufficient LL to prevent correction loss, especially in patients with high PI.
Introduction
'Flat back deformity' is a disorder of the thoracolumbar spine that results in chronic back pain and forward inclination of the trunk. The term 'flat back' was originally described by Doherty, as an iatrogenic complication of wherein thoracolumbar scoliosis correction by Harrington-distraction instrumentation [1]. Currently, it generally means sagittal imbalance caused by various factors [2]. Normal sagittal alignment is determined by various shapes and sizes of thoracic kyphosis (TK) and lumbar lordosis (LL) by the position of head, trunk, and pelvis in relation to the center of gravity. Loss of LL due to various causes usually initiates and leads to global sagittal imbalance. In flat back deformity, stooping of the trunk occurs because the lumbar spine, which is naturally lordotic, loses spinal sagittal balance by abnormal decrease in LL [3]. Conservative approach in flat back deformity is inefficient and has uncertain effects. Therefore, it is important to restore abnormal LL to a normal balanced state by realignment surgical treatment [45]. There are various surgical approaches to treat flat back deformity, generally comprising the posterior only and the anterior and posterior combined approach [67]. Recent studies show that the anterior approach with interbody fusion at multiple levels combined with posterior reconstruction is effective in the restoration of LL, especially in lower lumbar levels [8]. After surgical correction of flat back deformity, LL can be well maintained throughout the follow-up period [9]. However, in some cases, correction loss may also occur during follow-up. Each individual has an inherent normal value of LL, which gradually decreases with age [10]. Thus, the target of surgery should focus on the restoration of LL to the original alignment. However, there is no definite criteria for the determination of the degree of restoration because each individual has a wide range of LL that varies from approximately 20° to 60°. Pelvic incidence (PI) is one of the pelvic parameters that is an independent anatomical parameter and unique to individual. It determines pelvic orientation and size of LL. There have been numerous attempts to predict LL in relation to pelvic parameters [111213141516]. Schwab et al. [15] suggested that LL should be within 9° of PI for realignment of spinal deformity. The objective of this study was to provide an ideal correction angle of LL in degenerative flat back deformity based on the relationship between LL and PI from radiological and clinical results.
Materials and Methods
1. Materials
From January 2008 to December 2012, 61 patients with abnormal sagittal alignment underwent corrective surgery. The indications of correction were the 4 cardinal symptoms of degenerative flat back (stooping, difficulty in climbing, elbow support when washing dishes, and difficulty in holding in front of body) with intractable back pain or severe limitation to daily living activity, and radiographs showing global sagittal imbalance with sagittal vertical axis (SVA) >8 cm [17]. Patients with <1 year follow-up and patients with post-traumatic kyphosis or degenerative scoliosis without kyphosis were excluded. Eventually, 49 patients (45 females and 4 males) were enrolled in the study (Table 1). Among them, 24 cases were pure degenerative flat back, 10 cases were iatrogenic flat back, and 15 cases were degenerative kyphoscoliosis. Mean age was 65.6 years (range, 55-76 years) and mean follow-up period was 24.2 months (range, 12-61 months). On the basis of the method by Schwab et al. [15], we categorized the patients into 2 groups based on immediate postoperative radiographs-optimal correction (OC) group (PI-9°≤LL<PI+9°) and under-correction (UC) group (LL<PI-9°). There were no patients with overcorrection. We also classified the patients according to the individual size of the PI-low PI group (PI<55°) and high PI group (PI≥55°). We selected 55° as the reference point because the average PI among 61 patients was approximately 55°. Whole spine standing lateral view radiographs were taken preoperatively, immediate postoperatively, and at last follow-up in all patients.
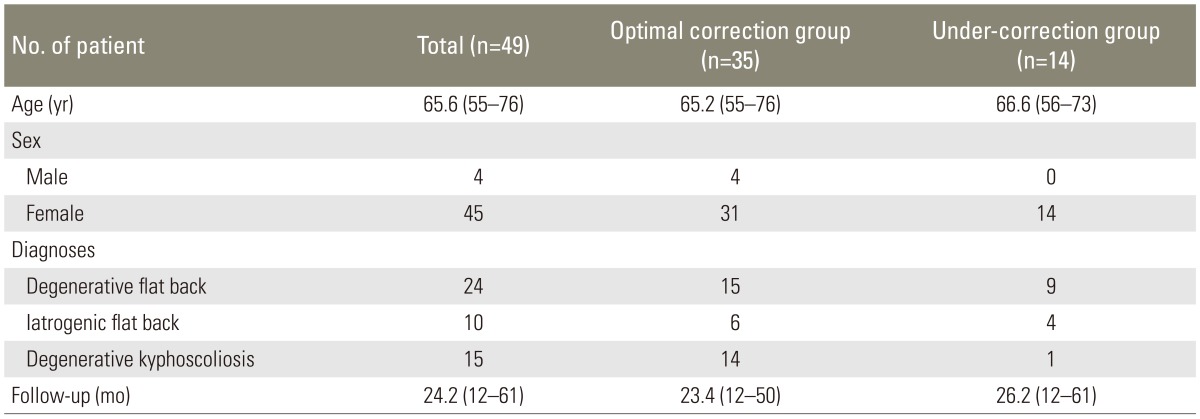
Patient demographics
2. Surgical procedures
All surgeries were performed by a single surgeon. Posterior-anterior-posterior sequential operation was conducted. From 2 to 4 levels of anterior lumbar interbody fusion (ALIF) was performed depending upon the case. The level of upper instrumented vertebra was from T8 to L2, which was determined by the sagittal angle of each individual. Distal fusion was carried out to the S1 and spinopelvic fixation using iliac screws in all cases. Additional osteotomy (pedicle subtraction osteotomy [PSO], 2; partial PSO, 9) was performed if sufficient LL was not achieved with the above method.
3. Radiological analysis
PI, TK, LL, and SVA were measured on 36-inch standing lateral radiographs of the entire spine at preoperative, postoperative, and follow-up examinations.
Cobb's angle between the upper end plate of T5 and the lower end plate of T12 was measured for TK, Cobb's angle between the upper end plate of L1 and the upper end plate of S1 was measured for LL. Kyphotic angle was expressed as a positive value, while lordotic angle was expressed as a negative value. For the SVA, a vertical distance was measured between the C7 plumb line and the posterosuperior corner of the S1 [18]. Positive and negative sagittal imbalance were defined by positive and negative values, respectively. All sagittal parameters were measured by 2 independent observers utilizing Picture Archiving and Communication System (π View, Infinitt, Seoul, Korea) (Fig. 1).
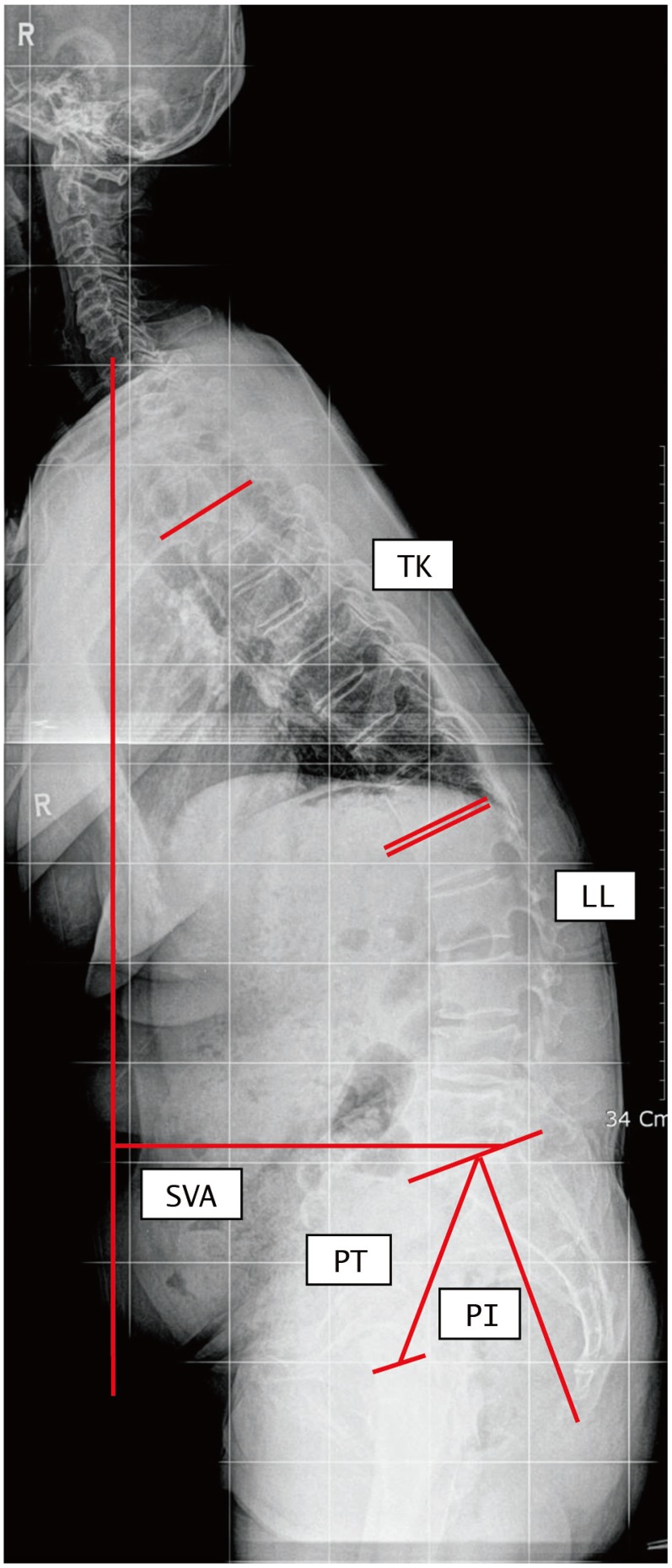
Measurement of sagittal parameters. Sagittal vertical axis (SVA) was the distance between the C7 plumb line and the posterosuperior corner of S1. Thoracic kyphosis (TK) was the Cobb's angle between upper end plate of T5 and lower end plate of T12. Lumbar lordosis (LL) was the Cobb's angle between upper end plate of L1 and S1. Pelvic incidence (PI) was the angle between the perpendicular to the sacral plate at its midpoint and the line connecting this point to the middle axis of both femoral heads. Pelvic tilt (PT) was the angle between the line connecting the midpoint of the sacral plate to the axis of the femoral heads and the line perpendicular to the floor.
4. Clinical analysis
Oswestry disability index (ODI) [19] and visual analog scale (VAS) of low back pain were measured and compared before surgery and at the last follow-up. Medical records were evaluated for perioperative and postoperative complications.
5. Statistical analysis
The IBM SPSS ver. 21 (IBM Co., Armonk, NY, USA) was used for statistical analysis. Pearson's chi-square test were used to determine whether there were any significant differences among the 2 groups. A significance level of 95% was chosen and a p-value <0.05 was considered statistically significant.
Results
1. Radiological results
Preoperative/immediate postoperative/last follow-up PI was 56.4°±9.5°, 53.4°±8.7°, and 56.8°±9.3°, respectively. PI was constant during the entire period (p=0.165). Overall LL was +9.4° (range, -14.9° to +48.1°) preoperatively, -48.7° (range, -67.3° to -26.7°) postoperatively, and -47.2° (range, -69.7° to -12.4°) at last follow-up. Overall preoperative pelvic tilt (PT) was 36.8° (range, 15.6° to 57.2°), which significantly decreased to 16.2° (range, -5.2° to 37.1°) immediately after surgery and slightly increased to 23.0° (range, 4.9° to 45.4°) at the last follow-up. Overall SVA was +24.5 cm (range, +6.8 to +50.3 cm) preoperatively, which significantly improved to normal range of +2.1 cm (range, -6.9 to +9.8 cm) postoperatively, and +4.2 cm (range, -3.1 to +12.9 cm) at the last follow-up. Based on SVA, 31 patients (63.3%) had good maintenance (SVA<5 cm) and 18 patients (36.7%) has loss of correction (SVA≥5 cm) at the last follow-up (Table 2).

Radiologic results
Considering the adequacy of immediate postoperative correction angle of LL, 35 (71.4%) of 49 patients were in OC group and 14 patients (28.6%) were in UC group. Grouping according to size of PI, 22 patients were in low PI group (PI<55°) and 27 patients were in high PI group (PI≥55°). In low PI group, 19 out of 22 patients (86.4%) were included in OC group, whereas in high PI group, only 16 out of 27 patients (59.3%) were included in OC group.
In OC group, 25 of 35 patients (71.4%) had good maintenance, whereas in UC group, more than half of the patients had loss of correction (57.1%) and only 6 of 14 patients (42.9%) were within normal range of SVA at the last follow-up (p<0.05). Due to small number of cases, we could not obtain statistical significance in comparisons between low and high PI patients. However, among the patients of OC group (35 patients), low PI group showed a tendency of better results (84%), as compared to high PI group (56%) without statistical significance (p=0.068) (Tables 3, 4).

Results of maintenance (by correction angle)
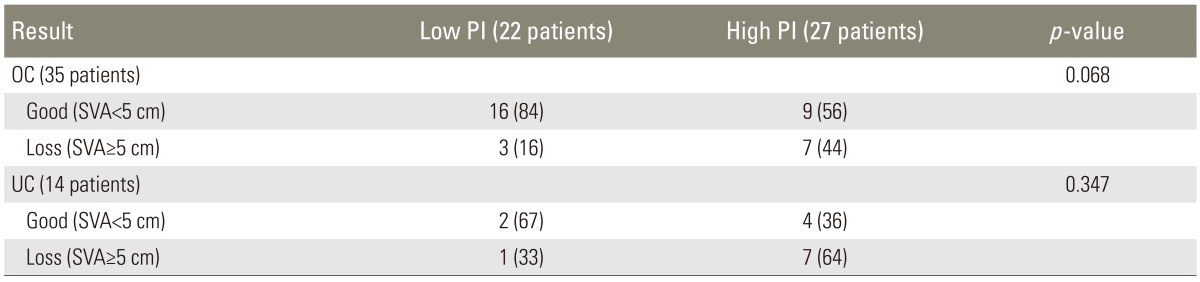
Results of maintenance (by pelvic incidence)
2. Clinical results
There was a significant decrease in ODI and VAS of low back pain at the last follow-up, as compared to the preoperative ODI and VAS in both OC and UC groups (Table 5). The mean ODI at the last follow-up of OC group (24.8±10.0) was lower than that of UC group (32.7±10.1), which was not statistically significant (p=0.975). In the same way, the mean VAS at the last follow-up of OC group (3.1±1.9) was lower than that of UC group (2.7±1.4) (Table 5).

Clinical results
3. Complications
Revision surgery was carried out in cases of surgical complications; 1 case due to pedicle screw malposition and 3 cases due to postoperative neurologic deficit in the lower extremity. Exploration with microscopy was performed in 3 cases with neurologic deterioration and no definite sign of nerve injury was found. Additional decompression and irrigation were conducted. All the patients showed progressive recovery of motor weakness after the revision surgery.
Discussion
Understanding the concept of sagittal spinal balance and compensatory mechanism is essential to planning surgical treatment of sagittal spinal deformity. Sagittal imbalance can be caused by decreased LL and increased TK, and can furthermore be influenced by the PI and flexion contracture of the hip and knee joints [3]. Basically, flat back deformity occurs as a result of decrease in LL and thus restoration of LL to the normal state is the main target of surgery. In the past, it was recommended to restore LL to normal range. However, since there is a wide normal range among individuals, some surgeons attempted to correct LL by approximately 20° more than TK. Kim et al. [20] analyzed postoperative sagittal balance following long adult spinal instrumentation and fusion. They reported that a sagittal Cobb angle difference between LL and TK of >20° is advisable to achieve optimal sagittal balance [20]. However, in flat back deformity, it is difficult to determine the accurate amount of correction with the method mentioned above, because TK usually decreases due to the compensatory action, as a result of loss of LL. Moreover, chin-brow vertical angle method is another means of predicting LL. However, it is usually used in gaining horizontal gaze in fixed global deformity such as ankylosing spondyltis, thus it is inappropriate for flexible types.
Recently, numerous studies emphasized the relevance of LL and corresponding influence of pelvic parameters [18212223], including pelvic incidence (PI), PT, sacral slope, and overhang (Fig. 1). PI is defined as the angle between the perpendicular line to the sacral end plate at its midpoint and the line connecting this point to the axis of the femoral heads [12]. Among the pelvic parameters, PI is the most critical factor because it is the only parameter that is unique to each patient and is independent of the position of the pelvis. In present study, preoperative, postoperative, and last follow-up PI of each individual showed no significant difference, suggestive of constant and unique features. Functionally, PI is closely related to optimal LL [232425]. There have been various attempts to predict LL using pelvic parameters. Legaye et al. [12] measured pelvic parameters in 49 adults free of vertebral disease and demonstrated a predictive equation for lordosis based on the parameters. Moreover, they suggested that a low value of PI implies low values of pelvic parameters and a flattened lordosis, whereas a high value implies well-tilted pelvic orientation and pronounced lordosis [12]. Vialle et al. [13] measured sagittal parameters of 300 asymptomatic volunteers and analyzed the relationships among them to predict maximal LL. Boulay et al. [11] evaluated 149 healthy adults to determine a lordosis predictive equation based on PI. They additionally used T9 tilt to predict LL and claimed that it increased reliability [11]. In 2010, Schwab et al. [15] analyzed radiographic values and ODI of 125 patients with spinal deformity and suggested that realignment objectives should include SVA<5 cm, PT<25°, and LL proportional to the PI (LL=PI±9°) [15]. In our study, patients who were under-corrected eventually had more loss of correction at the last follow-up (57.1%). We focused on the degree of OC of LL to restore normal sagittal alignment. We used Schwab's method (LL=PI±9°), which was relatively simple and tried to realign LL proportional to PI for prediction of target LL. Nevertheless, 14 of 49 patients (29%) were under-corrected (UC group; LL<PI-9°) on immediate postoperative radiographs. Patients in OC group had significantly better maintenance of sagittal balance (SVA≤5 cm) with less correction loss at the last follow-up (p<0.05). Thus it is critical to realign LL proportional to PI, within 9°, to get a satisfactory result (Fig. 2).
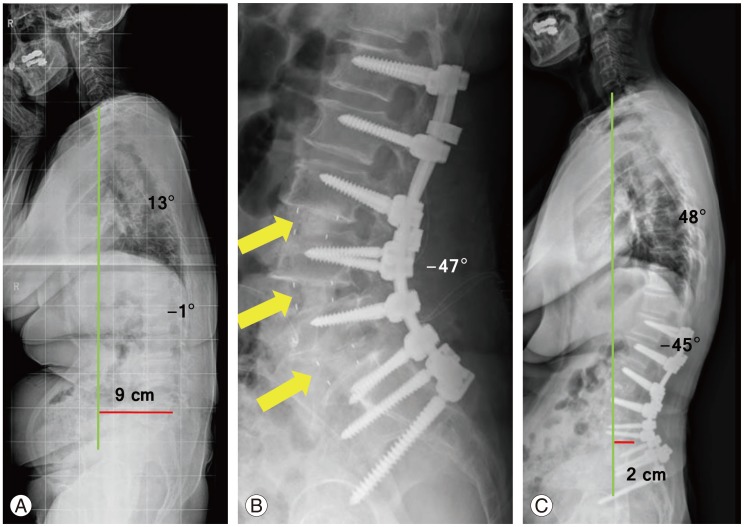
A 63-year-old female with degenerative flat back (A) received corrective surgery via 2 staged posterior-anterior-posterior approach. The patient had low pelvic incidence (PI) of 46°. Lumbar lordosis was optimally corrected to 47°, which was within 9° of PI (B). At last follow-up, correction is well maintained with sagittal vertical axis within normal range (<5 cm) (C). Arrows, interbody fusion cage.
Each individual has unique size of PI and therefore we hypothesized that if a patient has low PI, it would be easier to get OC since less LL is required to be corrected, resulting in better prognosis. Lee et al. [16] reported that mean value of PI in healthy adults was 52.5°. In addition, Legaye et al. [12] indicated the mean value of PI as 51°. The mean PI of 49 patients included in this study was 55.6°. Therefore, we classified the patients into 2 groups-low PI group (PI<55°) and high PI group (PI≥55°). The low PI group showed a tendency of better OC (86.4%), as compared to high PI group (59.3%) although it was not statistically significant (p=0.057). It means that if a patient has high PI, more LL is required to be corrected in order to make LL proportional to PI, which results in more chances of under-correction and correction loss at the last follow-up. Therefore, we recommend for sufficient LL in relation to PI, and in high PI patients, any type of osteotomy should be performed if optimal LL is not achieved with ALIF (Fig. 3).

A 64-year-old female with degenerative flat back showing severe forward inclination of trunk (A). Pelvic incidence (PI) was 58°. After anterior lumbar interbody fusion on L4-L5-S1, lumbar lordosis (LL) increased to 42° which was not in the target range (LL=PI±9°) (B). Therefore, we additionally underwent partial pedicle subtraction osteotomy on L4 and acquired sufficient LL of 51° (C). At last follow-up, sagittal balance is well maintained (D). Arrows, interbody fusion cage.
ODI improved at the last follow-up, as compared to the preoperative ODI in both OC and UC groups (p<0.05). However the mean ODI at the last follow-up of both groups showed no significant difference (p=0.975). This is because ODI not only reflects stooping symptoms due to sagittal imbalance but also reflects back and leg pain and other factors influencing daily living activities.
The limitations of the study were that it was a retrospective study with short follow-up period. Other factors influencing the outcome of surgery (e.g., age, osteoporosis, condition of hip and knee joint) should also be considered. Further study with a higher number of cases and longer follow-up will be needed to confirm our preliminary report.
Conclusions
Correction of LL proportional to PI (LL=PI±9°) will result in better sagittal balance with less correction loss in corrective surgery of flat back deformity. Loss of sagittal balance due to insufficient correction may often occur in patients with high PI (PI≥55°). Therefore, care should be taken to obtain sufficient LL proportional to PI.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.