Introduction
There have been many previous investigations of lumbar spine morphology in the English and Korean literatures [1-12]. According to the senior authorsŌĆÖ understanding, no one has yet conducted a systematic study of the age-related morphological alterations of the lumbar spine. Based on this information, the current authors created and performed the current study to give clinical material data for the practicing spine surgeons for their reference.
Materials and Methods
1. Materials
Case numbers of each decade (from 1st to 9th) are listed in Table 1. The study materials included 1,496 Jeju islanders from Korea from the first to 9th decade, including 555 men and 941 women, who had high-quality anteroposterior and lateral radiograms of their lumbar spines (Table 1).
This study was approved by the Institutional Review Board of Cheju Halla General Hospital (IRB approval no., CMC-MKIOR 121). Informed consent were not obtained because of a non-patient study using simple radiograms.
2. Methods
We performed in this study as follows: (1) age-related normal lumbar curve: coronal alignment, sagittal alignment; (2) abnormal alignment: coronal, sagittal; (3) disc degeneration: incidences; (4) disc degeneration associated spur formation (spur sizes and alignment): coronal alignment-related (normal alignment, abnormal alignment [scoliotic]), diffuse idiopathic spinal hyperostosis (DISH) (normal disc); (4) olisthesis: normally aligned lumbar spine, abnormally aligned lumbar spine; and (5) ballooned discs with biconcave vertebral body.
Different morphological parameters such as anteroposterior and sagittal alignment in an upright posture, incidences of disc space narrowing, corporal spur formation, dorsolumbar kyphosis, degenerative lumbar kyphosis, lumbar scoliosis (idiopathic, osteopathic, and degenerative), spontaneously and/or minor-trauma-induced vertebral body collapse, DISH, ballooned discs related to biconcave vertebral bodies without a cortical break due to severe osteoporosis, and so forth.
3. Coronal and sagittal alignment assessment (Table 2)
1) Coronal alignment
Type of alignment and factors contributing to alignment abnormalities include idiopathic, osteopathic, congenital hemivertebra, trauma-induced lateral wedged vertebra, and discogenic and iatrogenic alignment abnormalities brought on by disc degeneration
2) Sagittal alignment (Table 2)
It is measured by defining the lumbar spine into four categories: normal (40┬░ lordosis), hypolordosis (20┬░ lordosis), kyphosis (<5┬░ lordosis), and hyperlordosis (>75┬░ lordosis).
Results
1. Sagittal spine alignment (Tables 2ŌĆō6)
1) Sagittal lumbar spine alignment
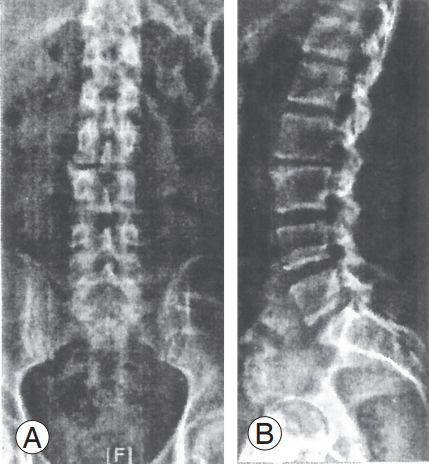
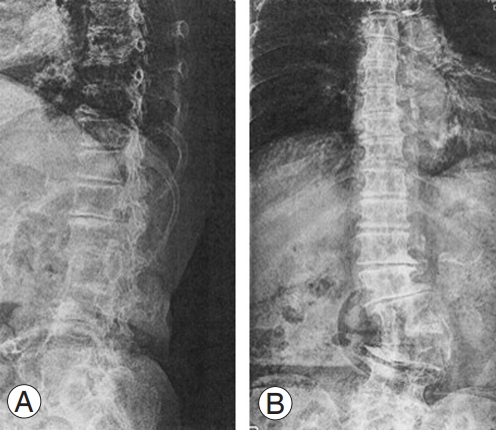
The 1st decadeŌĆÖs normal alignment was altered during the growth phase, set at growth maturity, and then maintained along the lordotic curve to the end of the 5th decade. Afterward, the curve is gradually hypolordotic. The trend of changing alignment is depicted in Table 2 and Fig. 1. A case of compensatory hyperlordotic lumbar spine secondary to osteopathic (osteoporosis) dorsolumbar kyphosis is shown (Fig. 2).
2) Degenerative lumbar hypolordosis
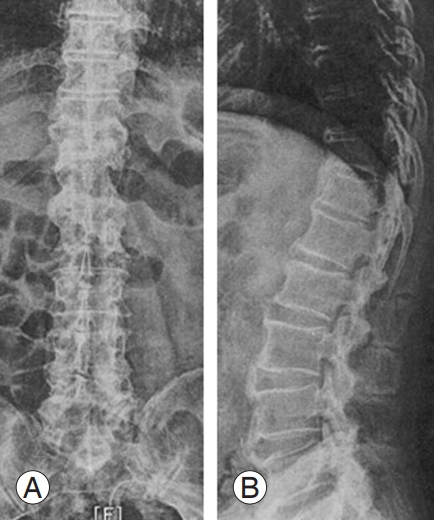
Incidences in 221 6th-decade patients were zero in 113 males and 0.9% in 108 females, 0.9% in 108 males, and 1.0% in 199 females among the 307 7th-decade patient. Patients in the 38 4th decade had 1.3% of men and 3.2% of women, whereas those in the 23 9th decade had 4.5% of men and 5.6% of women (Fig. 3). Post-trauma (fracture) dorsolumbar kyphoscoliosis: There were a few cases of trauma-induced dorsolumbar kyphosis were discovered (Figs. 4ŌĆō6).
3) So-called degenerative lumbar kyphosis (Table 7)
In none, this type of deformity was seen till the end of the 7th decade. A few elderly people in the 8th and 9th decades of life experienced this kind of malformation.
4) Osteopathic (due to osteoporosis) dorsolumbar kyphosis
Incidences were 0% in 108 men and 1.5% in 199 women among the 307 patients in the 7th decade, 0% in 75 men and 3.9% in 384 (75 men and 309 women) in patients in the 8th decade, and 2.3% in 44 men and 9.7% in 195 women among the 239 patients in the 9th decade. There was a case of congenital kyphoscoliosis (Table 8).
2. Disc space narrowing
The degree of narrowing is graded into six categories: normal (0), douftful (┬▒), 25% narrowing (+), 50% narrowing (++), 75% narrowing (+++), and 100% narrowing (++++).
3. Degree of disc space narrowing at each lumbar spine levels
None of the patients exhibited disc space changes by the end of the 3rd decade. In the 101 4th-decade patients two patients (1.9%; one male and one female) had questionable disc space narrowing. Twenty-six patients (25%; 15 males and 11 females) had narrowing (+), nine (five males and four females) had 50% bringing the total of 37 patients (36.0%). None of 3rd- and 4th-decade patients had narrowing over 75% (+++) to 100% (++++) (Table 9). The remainders in the 5thŌĆō9th decades are depicted in Tables 3ŌĆō7.
4. Corporsal spur formation and spur sizes
Two distinct spur shapes (claw and traction) were measured as one in this study. Small size is less than 3 mm in 5 lengths, and large size is over 3 mm. A significant corporal spur that projects horizontally from the spine on sagittal radiographs indicates the presence of DISH.
5. Incidences of corporal spur formation associated with disc degeneration (disc space narrowing)
1) Average percentile incidences of a small spur (Table 9)
The average percentile incidence of lumbar spine curvature in the 4th, 5th, and 6th decades was 2.9%, 4.5%, and 7.2%, respectively. Coronally scoliotic lumbar spine: The average percentile incidences of the 4th, 5th, and 6th decades were 9.5%, 10.7%, and 11.8%, respectively.
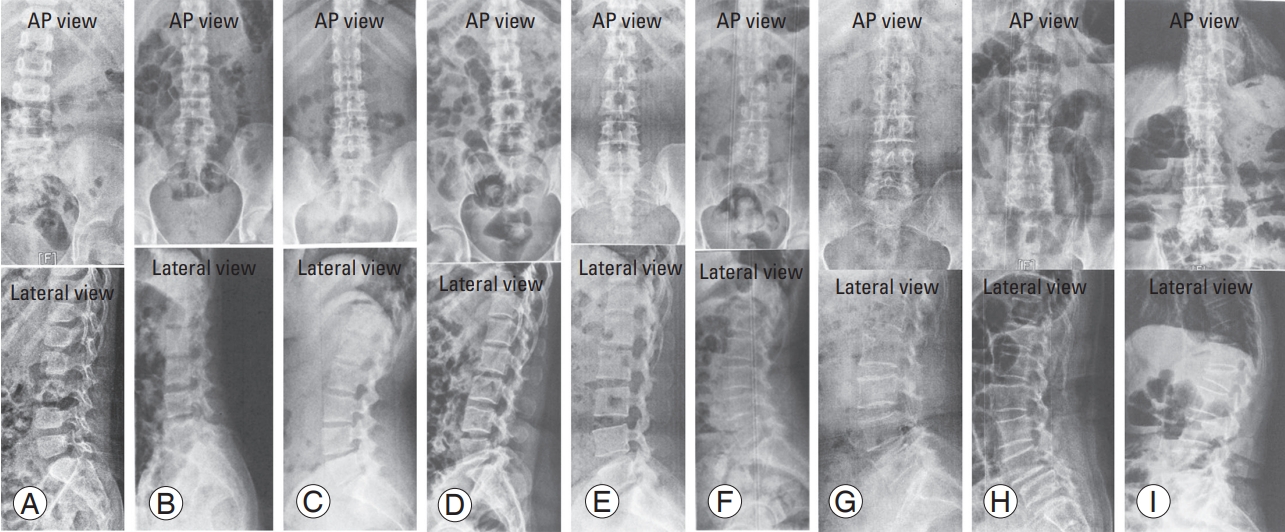
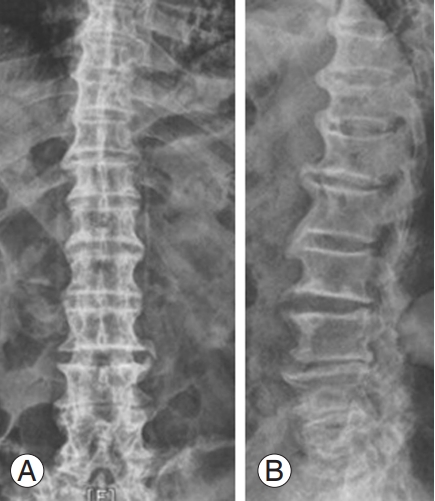
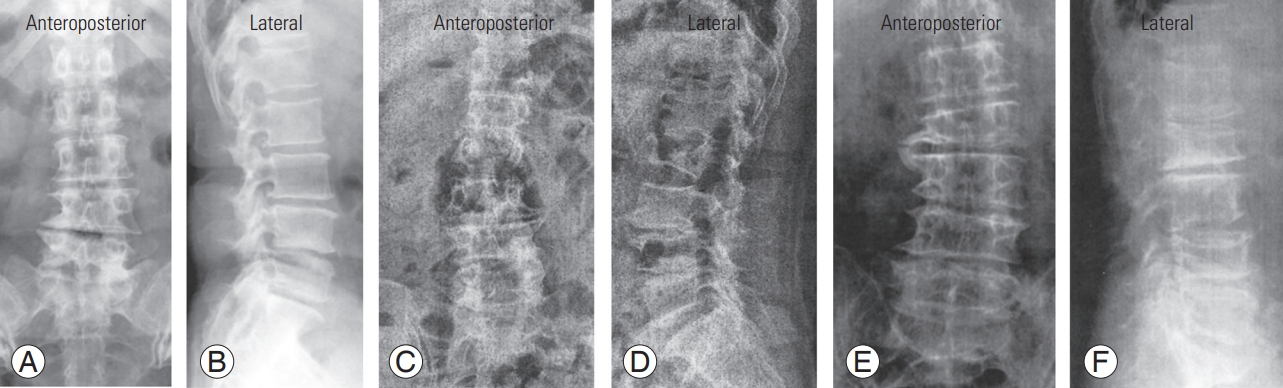
2) Average percentile occurrences of large spur (Figs. 7ŌĆō9)
Coronally straight lumbar spines: Incidences of the 4th, 5th, and 6th decades were 3.9%, 5.2%, and 9.5%, respectively. Coronally scoliotic lumbar spines: The incidences of the 4th, 5th, and 6th decades were 16.8%, 17.4%, and 22.2%, respectively.
6. Incidences of diffuse idiopathic spinal hyperostosis
ISH cases were nonexistent in the 1st, 2nd, 3rd, and 4th decades. The incidences of DISH in the 5th, 6th, 7th, 8th, and 9th were 1.3% (0.9%/1.9%), 2.3% (2.7%/1.9%), 3.6% (6.5%/1.5%), 39% (12%/1.9%), and 5.0% (15.9%/2.7%), respectively.
7. Vertebral body shape
Vertebral body shape is analyzed by its images on coronal and sagittal radiograms from T11 to L5. The evaluation was conducted using the classification by Genant [13]. of wedged, biconcave, and crush (flat) fractures in osteoporotic bone.
8. Dorsolumbar kyphosis
Dorsolumbar kyphosis is assessed by its shape: angular and round back shape.
9. Incidences of trauma-induced vertebral body collapses
The incidences of all types of spontaneous and/or minor trauma-induced vertebral body collapses from T11 to L5, including the wedge, biconcave, and crush described by Genant [13], were examined. Additionally, fractures severity was divided into four categories: grade 0: no fracture; grade I: mild fracture (approximately 20%ŌĆō25% height reduction); grade 2: moderate fracture (approximately 25%ŌĆō40% height reduction); and grade 3: severe fracture (>40% height reduction).
11. Main characteristics of lumbar scoliosis
Asymmetric disc degeneration-related lateral tilting and/or osteopathy (congenital or fracture-induced laterally wedged vertebral body) are the two main characteristics of lumbar scoliosis (Table 8).
12. Coronal lumbar spine alignment (Tables 9, 12)
Three types of coronal alignment abnormalities can be observed: idiopathic, osteopathic, congenital, or fracture-induced laterally wedged vertebra and discogenic. In the current study series, only three patients had idiopathic hemivertebra: one in the 2nd decade and two in the 7th decade. No one had congenital hemivertebra. The remainder were discogenic (discopathic), especially in females.
1) Idiopathic scoliosis: Only three cases were found: one in the 2nd-decade female and two in the 7th-decade females (Figs. 12, 13).
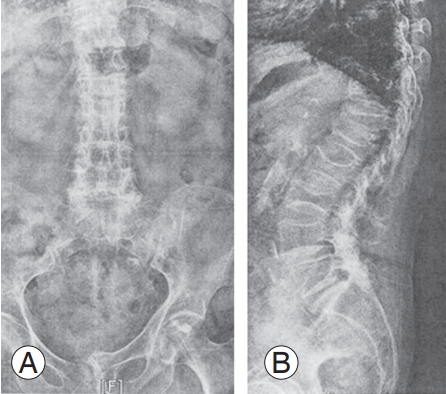
2) Vertebral body fracture-related (osteopathic) scoliosis: There was one case (0.3%) among the 307 7th-decade patients, 19 (6.1%) among the 309 8th-decade females, and 8 (3.0%) among the 195 9th-decade patients.
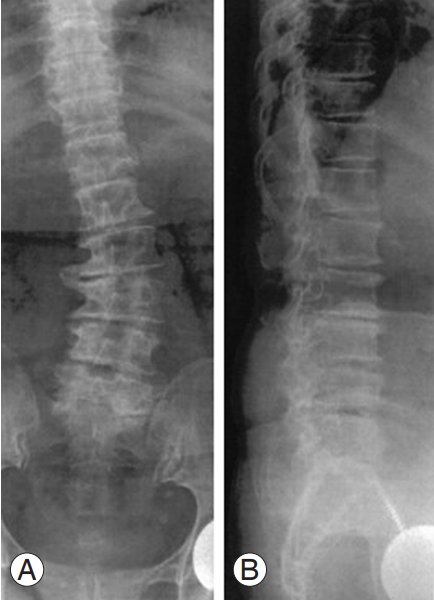
3) There was one case of L1 congenital kyphoscoliosis case (Fig. 14).
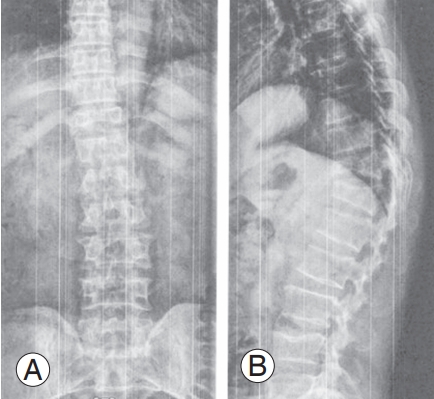
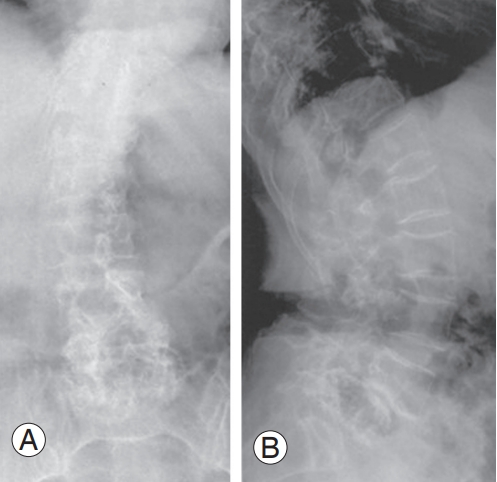
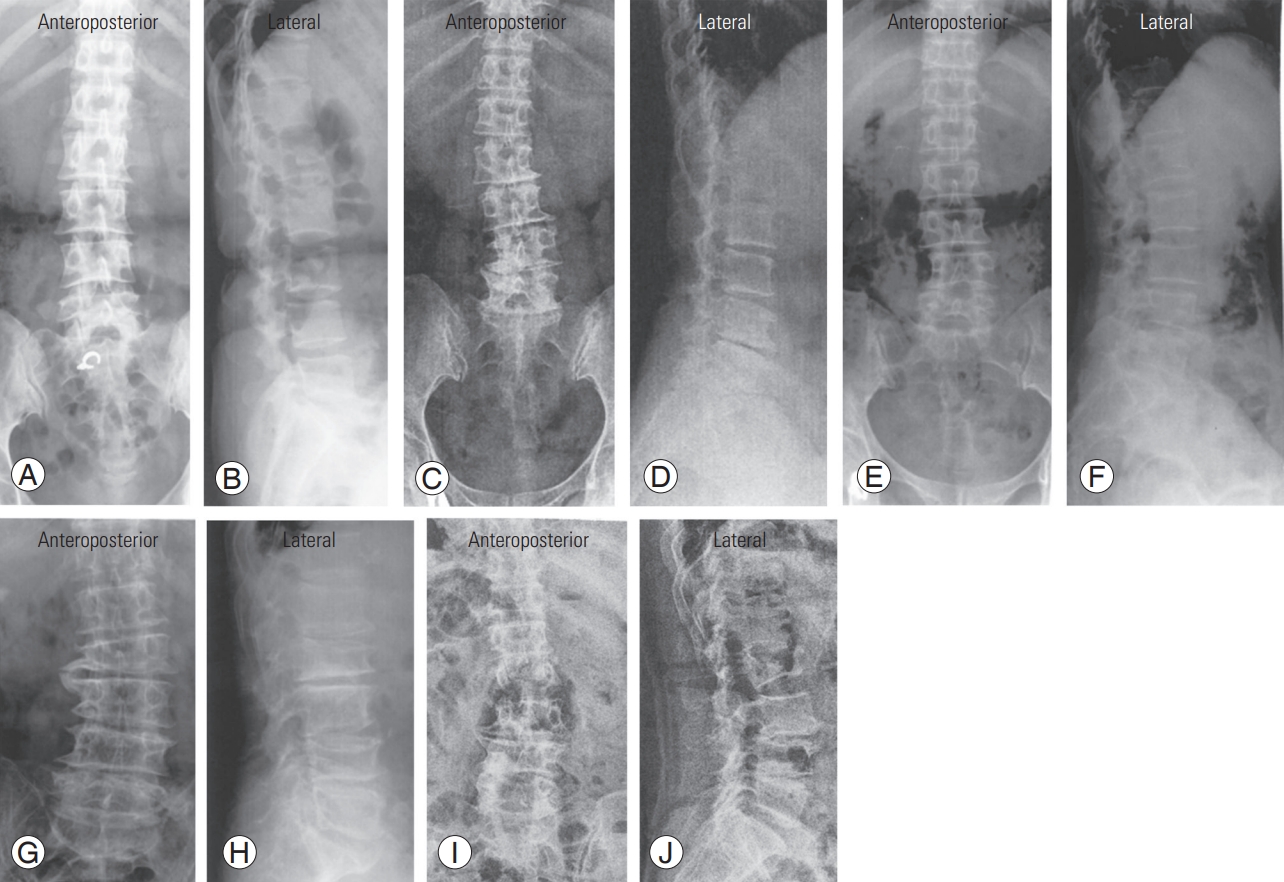
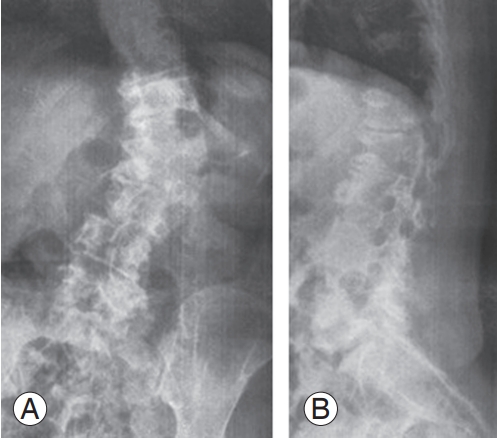
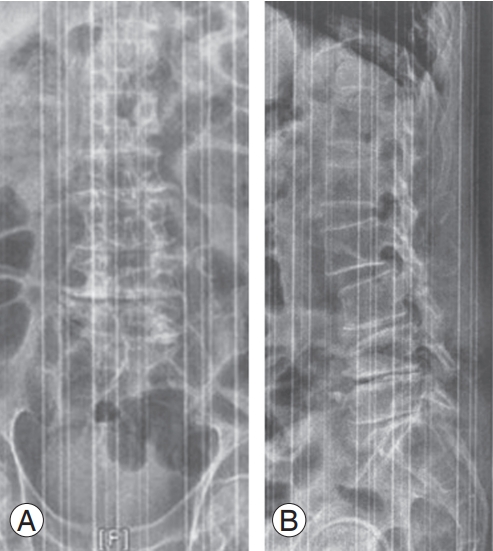
4) Degenerative lumbar scoliosis (Table 9): The occurrences of 29 degenerative lumbar scoliosis (DLS) (13.1%; three males/26 females) among the 221 6th-decade patients (113 males/108 females), 45 (14.7%; 10 males/35 females) among 307 7th-decade patients (108 males/199 females), 64 (16.7%; 11 males/53 females) among the 383 (44 males/309 females) 8th-decade patients, and 64 (25.8%; 18 males/46 females) among 239 (44 males/195 females) 9th-decade patients (Figs. 15ŌĆō24).
5) SpondylolysisŌĆōrelated scoliosis: In this series, none had scoliosis.
6) Post-laminofactectomy-related scoliosis: There were none. Sondylolisthesis is defined when the vertebral body displaces at the disc level anteriorly, posteriorly, or laterally (rotatory lateral). Vertebral body displacement at the disc level in an anterior, posterior, or lateral direction is known as sondylolisthesis (rotatory lateral). Vertebral bodies typically shift one level, although on rare occasions they shift two levels in the same or the opposite direction.
13. Incidences of spondylolisthesis in normally aligned and scoliotic lumbar spines
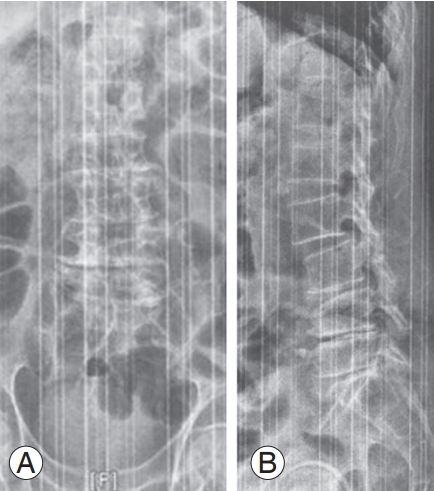
No cases having either type of spondylolisthesis till the end of the 4th decade. The 155 5th-decade patients had spondylolisthesis nine patients (five males/four females) with a coronally straight spine. There were no cases of scoliosis. Among the 221 6th-decade patients (113 males/108 females), there were 19 patients with olisthesis (three anteriolisthesis and one retrolisthesis), while in the patients with scoliosis, eight had olisthesis (two anteriolisthesis, one retrolisthesis, and five laterolisthesis). Table 13 and Table 14 lists the prevalence of olisthesis in the 7th, 8th, and 9th┬Āgrades (Fig. 15).
14. Spondylolisthesis
1) Age-related incidences
Incidences of slip in coronally normally aligned spine is as follows. There were no olisthesis in the 1st-, 2nd-, 3rd-, and 4th-decade patients. Overall incidences in the 5th-decade patients were two (zero in males and two in females): one antero-listhesis and one retrolisthesis at L3, four cases (one male and three females) at L4 levels, and four males at L5. Overall incidences in the 6th-decade patients were zero at L1 and L2, one anterolisthesis at L3, 14 (13 anterolisthesis: five males, 18 females) at L4 disc level, and three anterolisthesis (one male/12 females) at joint L5 level. Overall incidences in the 7th, 8th, and 9th decades and listed in Table 15.
2) Overall incidences of slip in scoliotic lumbar spine
None slip was found. In the 6th-decade patients, there were five laterolisthesis in females at L3 disc level, two slips (one anterolisthesis and one retrolisthesis) at L4 disc level, and one anterolisthesis at L5. In the 7th-decade patients, there were one anterolisthesis and four retrolisthesis in five females at L3 disc level and 16 olisthesis (three males/13 females; 15 anterolisthesis and one laterolisthesis at L4 disc level and one anterolisthesis in one female at L5). In 8th- and 9th-decade patients, slips were not found.
15. Incidences vertebral body collapse in the 5th, 6th, 7th, 8th, and 9th decades
The incidences of all types of vertebral body collapse (wedged, biconcave, and crush [flat]) in the 5th, 6th, 7th, 8th, and 9th decades were 12.3% (6.5% in male and 23.5% in female), 18.5% (10.0%/25.9%), 25.4% (18.5%/29.1%), 32.5% (34.7%/32%), and 38.4% (27.3%/41.0%), respectively. In patients in the 7th, 8th, and 9th decades, the overall percentile occurrences of biconcave vertebral bodies linked to inflated discs were 0.95% (0.9%/1.0%), 4.4% (1.3%/5.1%), and 16.7% (9.1%/18.5%), respectively (Tables 14, 16).
Discussion
It was stated by the authors in the introduction that there are many previous studies related to lumbar spine morphology. However, nobody has yet carried out repeated systematic research on the age-related morphology of the lumbar spine. In the current study, the senior author created the survey chart and performed the roentegenological study of the lumbar spine, according to the study design.
A recent study on sagittal alignment revealed that once normal lordosis in the lumbar spine develops, it is maintained through the end of the third decade, and that disc degeneration causes it to become increasingly hypolordotic after that. The incidences of disc degeneration in the 4th decade lumbar spine were higher (36.6%) than those (13.2%) of the cervical spine. More load-bearing is thought to be the root of the higher occurrence. When vertebrae collapsed, the lumbar spine in certain cases became hypolordotic.
Dorsolumbar kyphosis is created by osteoporotic vertebral fractures of dorsolumbar spine (Table 2), and in some cases developed lumbar kyphosis due to disc degeneration.
Regarding the three types of coronal lumbar spine alignment abnormalities in the present series, there were no congenital ones (hemivertebra), and only three patients among the 1,496 surveyed patients had idiopathic scoliosis. The majority of discogenic remaining syndromes (DLS) were found in females over 50 years, and as time went on, the prevalence of DLS increasingly rose. This fact has great clinical significance related to lumbar spinal stenosis in DLS patients. There were no incidences of spondylolysis- and post-laminofacetectomy-related scoliosis in the current series (Table 12).
It is a known fact that spondylolisthesis can occur either in the normally aligned or scoliotic lumbar spine. No cases were having degenerative spondylolisthesis till the end of the 4th decade in the current series. It is interesting to notice that anterior- and retro-listhesis occurred both in the normally aligned and scoliotic lumbar spine, while laterolisthesis (rotatory) occurred only in the scoliotic spine. Additionally, these facts imply that disc degeneration owing to facet disease is what drives the progression of scoliosis with age.
It was discovered that age-related disc degeneration begins to develop in the 4th decade and steadily increases in incidence and severity in conjunction with the growth of the corpus callosum (Tables 8, 9). Spur formation in association with the disc space narrowing occurred only in the non-porotic spine, while disc space narrowing and spur formation did not occur in porotic spine, and the osteoporotic spine revealed wedged, biconcave, and crushed bodies (Genant [13]). In contrast to the coronally scoliostic spine with a huge spur, the straight-aligned spineŌĆÖs spur diameters were smaller. This fact suggests the reason for the clinically relatively higher incidence of lumbar stenosis in the degenerative scoliosis patient in comparison with those of the non-scoliotic spine.
DISH was not discovered in first to 4th-decade patients and then occurred from the 5th decade onward. However, the current authors failed to find out reasonable causes.
Regarding vertebral body collapse brought on by spontaneous or minor trauma, collapses were noted in patients as early as the 5th decade and gradually increased over time, and biconcave vertebral bodies related to the ballooned disc were observed in the 7th-, 8th-, and 9th-decade patients with an increasing tendency (Table 14).
The shortcomings of this research are inequality of case numbers in each decade, lack of computed tomography and magnetic resonance imaging images in all cases, and lack of study on the musculature contribution to the lumbar spine morphology.