Introduction
Scoliosis (meaning "crooked") is a medical condition where a person's spine is curved from side to side [1]. It is the most common type of spinal deformity confronted by the orthopedic surgeons [2]. A scoliosis spinal columns curve Ōēż10┬░ affects 1.5% to 3% of people [3]. Prevalence of curves <20┬░ is almost equal in males and females. It is most common during late childhood [4]. The condition affects approximately 6 to 7 million people in the United States. Considering the most common form of scoliosis, adolescent idiopathic scoliosis (AIS), there is no clear causal factor and it is generally believed to be a multifactor problem [5]. However, a primary muscle disorder and/or genetic factors are believed to be the responsible etiologies. AIS is the most common type of idiopathic scoliosis and the most common type of scoliosis overall [5].
The traditional medical management of scoliosis is complex. The conventional options sequentially include observation, bracing, and surgery. Spinal deformity is surgically operated to correct or improve deformity: to maintain sagittal balance, to preserve or to improve pulmonary function, to minimize morbidity or pain, to maximize postoperative function, to improve or at least not to harm the function of the lumbar spine [6]. Indications for operative treatment of AIS include developed curvature in the growing children, severe deformity C >50 with asymmetry of trunk in adolescents, pain which cannot be controlled by non-operative treatments, thoracic lordosis, and significant physical deformity. Surgical techniques may include anterior, posterior, or combined anterior-posterior fusion surgery [6,7]. Anterior techniques include anterior instrumentation and fusion for idiopathic scoliosis which is now regarded as a well-accepted procedure for certain thoracolumbar and lumbar curves [6,7]. Posterior techniques include posterior fusion and instrumentation by pedicle screws or hooks without using the anterior approach. Combined techniques include two stages: 1) anterior release and fusion and 2) posterior fusion and instrumentation using multi-hook segments [6,7]. A combination of these two stages is used in more severe cases. Scoliosis has been surgically treated for the past 15 years at Tabriz Shohada Hospital. This study aims at comparing two surgical methods, combined anterior-posterior approach using hybrid lumbar pedicle screws and thoracic hooks with posterior-only approach using lumbar and thoracic pedicle screw systems to treat severe scoliosis with curvature >70┬░.
Materials and Methods
Medical records of 50 patients suffering from thoracic non-congenital scoliosis with curves exceeding 70┬░ were reviewed. The case group consisted of 25 patients who underwent posterior spinal fusion using thoracic pedicle screws (group A) and the control group consisted of other 25 patients (group B), who underwent anterior release by thoracotomy approach in the first stage and postoperative traction for 8 to 10 days, respectively. Traction included distal femoral skeletal and skull tractions. At the second stage, the patients underwent posterior fusion and instrumentation using pedicle screws in lumbar vertebra and pedicle hooks and transverse hook to upper thoracic. Considering radiography, all curves of the thoracic, thoracolumbar, and lumbar spine were measured using coronal Cobb measurement.
Patients with congenital scoliosis and anomalies of spinal canal were excluded from the study. The two groups were compared considering correction rate, days of hospitalization, duration of traction, total cost of treatment, and postoperative complications. Written informed consent was obtained from all patients. The study was approved by Ethics Committee of Tabriz University of Medical Sciences.
1. Statistical analysis
The statistical analysis of data was carried out using the SPSS ver. 16 (SPSS Inc., Chicago, IL, USA). Continuous variables are shown as mean┬▒standard deviation. Fisher's exact test or chi-square test was used to study qualitative variables. Independent t-test was used to evaluate the quantitative variables between the two groups. In this study, pŌēż0.05 was regarded as statistically significant.
Results
The present study was conducted on fifty patients. Demographic characteristics of patients of both the groups are shown in Table 1. No significant difference was observed between the two groups with respect to gender and age.
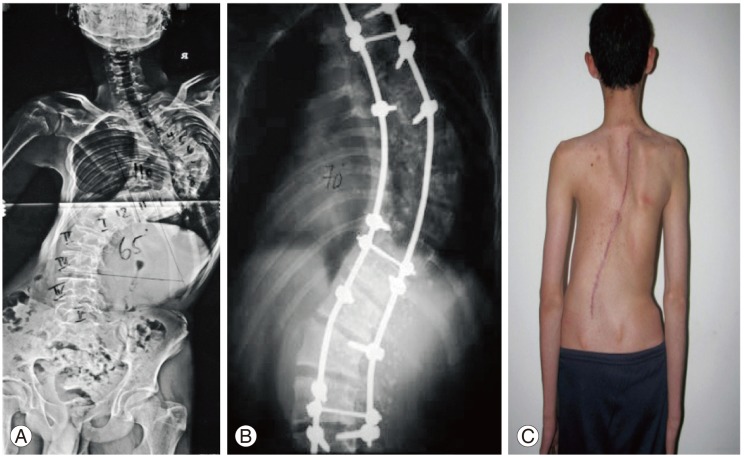
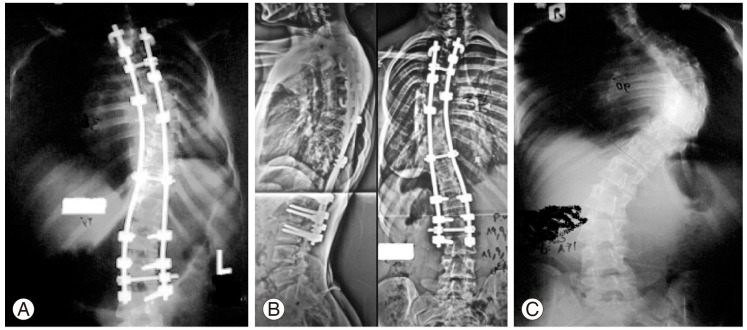
There was significant difference between the two groups considering duration of hospitalization, intensive care unit (ICU), traction, and correction degree seen in lateral view (Table 1). Figs. 1 and 2 refer to radiographic and clinical images of one patient treated using posterior-only method and a combined posterior-anterior approach, respectively.
Discussion
Rate of correction is one of the most important goals of all the surgical methods [7]. There are various reports in the literature comparing anterior releasing and posterior fusion methods in treating scoliosis [7]. Yamin et al. [8] published a retrospective study on a staged surgery for severe rigid scoliosis with coronal Cobb angle>80┬░ treated by staged surgeries including anterior release and halo-pelvic traction as the first and posterior instrumentation and spinal fusion as the second stage. They concluded that staged operation offers a safe and effective way in treating severe rigid scoliosis [8]. Min et al. [9] assessed clinical, radiological and outcomes of the patients suffering from idiopathic AIS and its treatment by selective short anterior fusion of the major thoracolumbar/lumbar (TL/L) curve. They concluded that selective short anterior fusion of the TL/L curve scoliosis with a thoracic curve Ōēż25┬░ (according to Lenke classification, type V) results in a satisfactory corrected and a balanced spine. Short fusions leave enough mobile lumbar segments for establishment of global spinal balance [9].
Considering correction rate of the curves, treatment of AIS >80┬░ using posterior-only fusion method is comparable to most of the series of combined anterior-posterior surgery with shorter operation time without leaving any adverse effect on pulmonary function of anterior transthoracic exposure [6,9]. Compared with hybrid construct, posterior spinal fusion method used by only pedicle screws in severe cases of thoracic AIS allowed a greater coronal correction of both main thoracic and secondary lumbar curves, and resulted in less loss of the postoperative correction achieved, and fewer revision surgeries were required. Using posterior-only fusion method with pedicle screws enabled a good and stable correction of severe scoliosis. However, severe curves may be amenable to hybrid instrumentation, which has produced results similar to those of the screw-only construct with regards to patient satisfaction [10].
Suk et al. [11] compared segmental pedicle screw fixation method with multi-hook segmental fixation systems in treating thoracic idiopathic scoliosis. The correction rate was estimated as 55% and 72% using hooks and segmental thoracic pedicle screws, respectively. The study reported a 3% malposition rate for thoracic pedicle screws based on plain radiographs. There was neither medial intracanal malposition nor any neurological complications [11]. Luhmann et al. [12] found that posterior-only thoracic pedicle screw constructs provided correction rate equal to that of hook constructs with anterior release.
Thoracic pedicle screw instrumentation, therefore, eliminates need for an anterior approach. Sanders et al. [13] found significantly better major and minor curvature correction rates without any neurological problem and improved pulmonary function with posterior pedicle screw instrumentation as compared with segmental hook instrumentation. Betz et al. [14] reported that coronal correction and balance were equal in both anterior and posterior groups. In the anterior group there was a better correction of sagittal profile in patients with a preoperative hypokyphosis <20┬░. However, hyperkyphosis (with a mean of 54┬░) occurred in 40% of members of the anterior group with a preoperative kyphosis >20┬░ [14].
Thoracic pedicle screws improved correction in both coronal and axial planes. Lumbar lordosis can be satisfactorily controlled to produce more thoracic hypokyphosis in comparison with posterior segmental hook instrumentation.
However, sagittal correction of scoliosis was significantly different between the two groups but there was no statistically significant difference with respect to coronal correction. Bi-step surgery to correct scoliosis may result in some complications since wound or anesthesia-related complications might be at a risk of increase. Complications of thoracotomy (haemothorax, pneumothorax, etc.) are other potential threats. Postoperative events should also be noted. Because of special complications of ICU admissions, statistically significant difference is an important factor considering ICU admission. Total hospitalization duration is another factor that should be mentioned. Long-term hospitalization may result in increase in risks related to hospitalization (medical errors, nosocomial infections, psychological effects, etc.) [15].
The risk of scoliosis surgery is estimated to be 5%. Inflammation of the soft tissue or deep inflammatory processes, breathing impairments, bleeding, and nerve injuries may be regarded as possible complications. As early as five years after surgery, about 5% of the patients require reoperation [16]. The most common form of scoliosis never exceeds 80┬░ [16]. Unfortunately, the physical effects of surgery are not necessarily stable [5]. Posterior segmental pedicle screw fixation without anterior release had resulted in satisfactory deformity correction in severe scoliosis without significant loss of curvature correction. In this series, a single posterior procedure obviated the need for the anterior release and eliminated complications related to anterior surgery [13].